Unresectable Stage III EGFR NSCLC - AstraZeneca
Explore Trial Data















Top 10 by impressions - click to view on X
#LungSeries: w/ @BalazsHalmosMD we 🗣️ the SoC for mNSCLC w/🎯mutation in 1L (Osi, Ami, Alectinib, Lorlatinib, et al) Full discussion: - - - Also on the “Oncology...

LAURA passes the "truck test" to a rousing ovation at #ASCO24 plenary session, with osimertinib given to patients with locally advanced unresectable stage III EGFRmut NSCLC...
Laura curves . Incredible. HR of 0.16 . 39. 1 months vs 5.6 months. With almost 80 % Cross over. Definitely practice changing . @DrRiyazShah @OncBrothers @OncoAlert...
Impressive increase in PFS with consolidation osimertinib after CRT for pts w unresectable stage III lung cancer. Crossover on progression 82% higher than in most other studies. OS far from mature....

LIFETIME osimertinib after a treatment with curative intent? In pts with EGFRmut stage III NSCLC, chemo-radiotherapy can CURE pts. Were pts in LAURA properly staged by petscan/brain RMI? Why not...
Overheard at Best of #ASCO24 Albuquerque: “Wait. Are you that doctor that dances while giving updates on lung cancer?” Why yes, that’s me 😂
IT DOESN’T MATTER IF YOU CALL IT ADJUVANT OR CONSOLIDATION, USE YOUR BEST SYSTEMIC TREATMENT AFTER DEFINITIVE TREATMENT FOR EGFR M+ LUNG CANCER (AND PROBABLY ALK AND RET+)!

🔥🚨Hot off the press. Press Release by @AstraZeneca. #LAURA Phase III trial of #Osimertinib vs placebo after chemoradiotherapy for pts with unresectable...
With news of the positive results from LAURA (consolidation osimertinib for stage III #EGFR NSCLC post chemoradiation), how would you approach a similar setting today: unresectable...

80% is false. Crossover to OSI was only given to 50/66 75% of patients I guess the other 25% of patients didn't deserve the best care? Paper also doesn't...
LAURA is a landmark Phase III, double-blind, placebo-controlled trial that established consolidation osimertinib (Tagrisso) as the new standard of care for patients with unresectable stage III EGFR-mutant NSCLC who have not progressed during or after definitive chemoradiation therapy. The trial randomized 216 patients across 17 countries in a 2:1 ratio to receive osimertinib 80 mg daily or placebo until disease progression. LAURA is the first phase 3 study to assess a targeted agent following chemoradiotherapy in unresectable stage III NSCLC, filling a critical treatment gap where durvalumab (PACIFIC) showed inconclusive efficacy in the small EGFR-mutant subset.
Phase III, international, double-blind, 2:1 randomized, placebo-controlled trial in patients with unresectable stage III EGFR-mutant (exon 19 deletion or L858R) NSCLC who completed definitive platinum-based concurrent or sequential chemoradiation therapy without disease progression. EGFR mutations identified by central or local certified testing. Randomization stratified by CRT type (concurrent vs sequential), tumor staging (IIIA vs IIIB/IIIC), and China cohort.
Adults (18+ years, 20+ in Japan) with locally advanced, unresectable stage III NSCLC harboring EGFR exon 19 deletions or L858R mutations, WHO performance status 0-1, who completed at least 2 cycles or 5 weekly doses of platinum-based chemotherapy with radiation (54-66 Gy) within 6 weeks prior to randomization. Excluded patients with history of ILD, symptomatic pneumonitis following CRT, or prior EGFR TKI therapy.
Osimertinib 80 mg orally once daily versus placebo, continued until disease progression by BICR (RECIST 1.1), unacceptable toxicity, or other discontinuation criteria. Open-label osimertinib crossover offered to placebo patients upon progression.
Primary endpoint: progression-free survival (PFS) assessed by blinded independent central review (BICR) per RECIST 1.1. Key secondary endpoints: overall survival (OS) and CNS progression-free survival by BICR. Additional secondary endpoints: objective response rate (ORR), duration of response (DoR), time to first subsequent treatment (TFST), second PFS (PFS2), time to second subsequent treatment (TSST), safety, and tolerability.
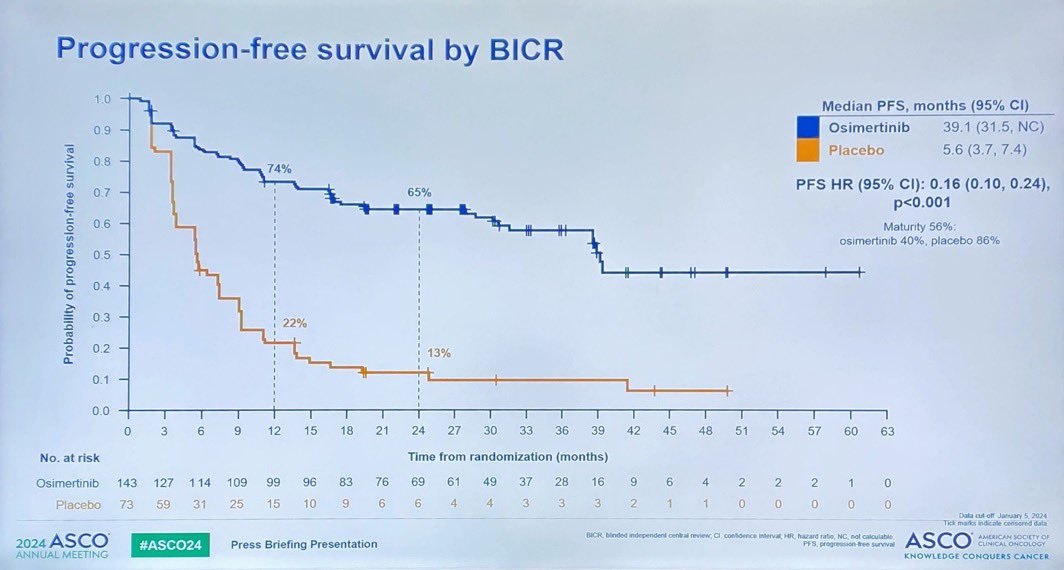
Osimertinib demonstrated a profound PFS benefit versus placebo. Median PFS was 39.1 months (95% CI: 31.5-NE) with osimertinib versus 5.6 months (95% CI: 3.7-7.4) with placebo, with a hazard ratio of 0.16 (95% CI: 0.10-0.24; p<0.001), representing an 84% reduction in risk of disease progression or death. PFS rates at 12 and 24 months were 74% and 65% with osimertinib versus 22% and 13% with placebo. Investigator-assessed PFS was consistent (HR 0.19; 95% CI: 0.12-0.29). Benefit was observed across all prespecified subgroups.
Interim OS data at 20% maturity showed a non-significant trend favoring osimertinib: 36-month OS rates of 84% vs 74% (HR 0.81; 95% CI: 0.42-1.56; p=0.53). Updated OS analysis at 31% maturity (ELCC 2025) showed median OS of 58.8 months vs 54.1 months (HR 0.67; 95% CI: 0.40-1.14; p=0.140), with 48-month OS rates of 70% vs 52%. Notably, 78-80% of placebo patients crossed over to receive osimertinib upon progression, confounding OS interpretation. Final OS analysis planned at 60% maturity.
Grade 3+ adverse events occurred in 35% of osimertinib patients vs 12% with placebo. ILD/pneumonitis (including radiation pneumonitis) occurred in 56% of osimertinib patients vs 38% placebo; majority were Grade 1-2, with Grade 3 in 3.5% and one fatal case (0.7%). Radiation pneumonitis specifically occurred in 48.3% vs 38.4%. ILD or ILD-like reactions reported in 7.7% vs 1.4%. Permanent discontinuation due to AEs was 8.4%; dose interruptions in 42.0%; dose reductions in 4.9%. Most common AEs: radiation pneumonitis (48.3%), diarrhea (35.7%), rash (35.7%), paronychia (23.1%).
LAURA established osimertinib as the new standard of care (NCCN Category 1) for unresectable stage III EGFR-mutant NSCLC after CRT, replacing durvalumab consolidation for this molecular subgroup. Key clinical debates include: (1) the unusually low 5.6-month placebo PFS suggesting possible occult metastatic disease due to inadequate baseline staging; (2) immature OS data with high crossover rates (78-80%) complicating survival interpretation; (3) overtreatment concerns since 20-30% of stage III patients may be cured by CRT alone, raising questions about exposing all patients to indefinite osimertinib with its associated physical (35% Grade 3+ AEs) and financial toxicity (ICER $322,308/QALY in US); (4) alternative close-surveillance strategy advocated by some oncologists to spare cured patients from unnecessary treatment while catching recurrence early.

















































































