KRAS G12D-mutant advanced solid tumors (primarily NSCLC) — Astellas Pharma (Setidegrasib)
Discover KOL Sentiment on 3082-CL-0101 →Design - Phase 1 first-in-human dose-escalation/expansion study of setidegrasib (ASP3082), a first-in-class KRAS G12D-selective degrader, in KRAS G12D-mutant advanced solid tumors, primarily NSCLC (NCT05382559; Astellas).
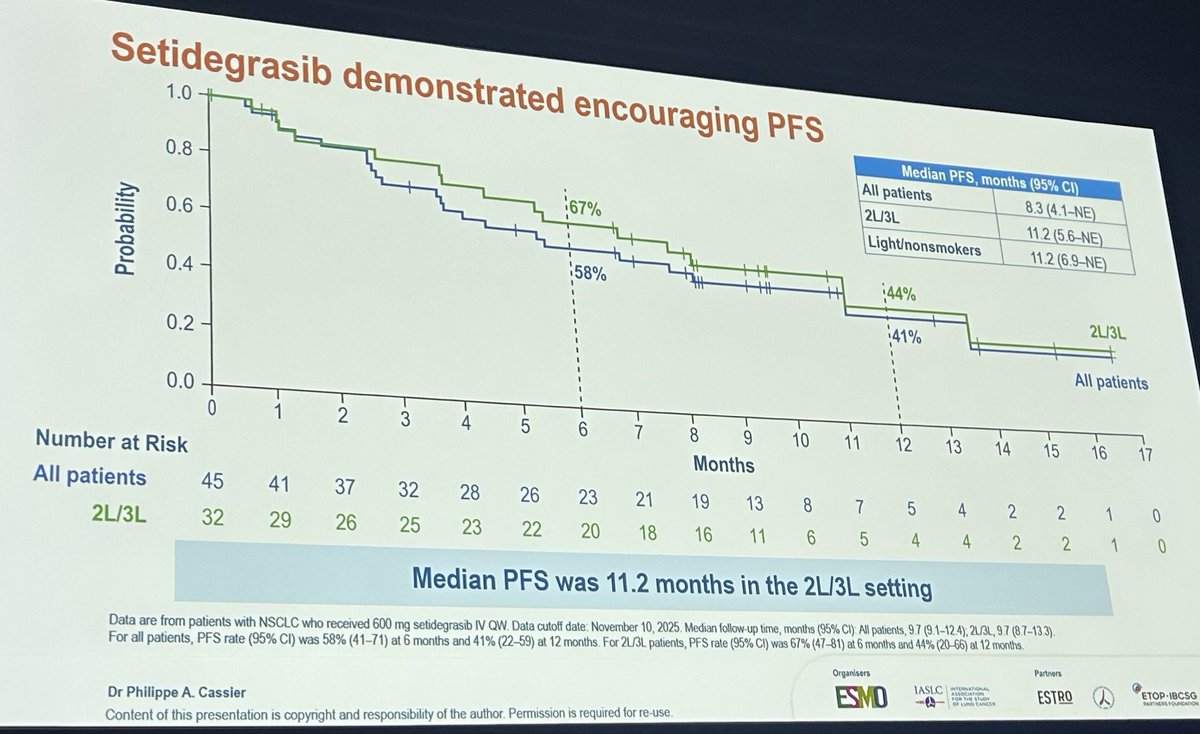
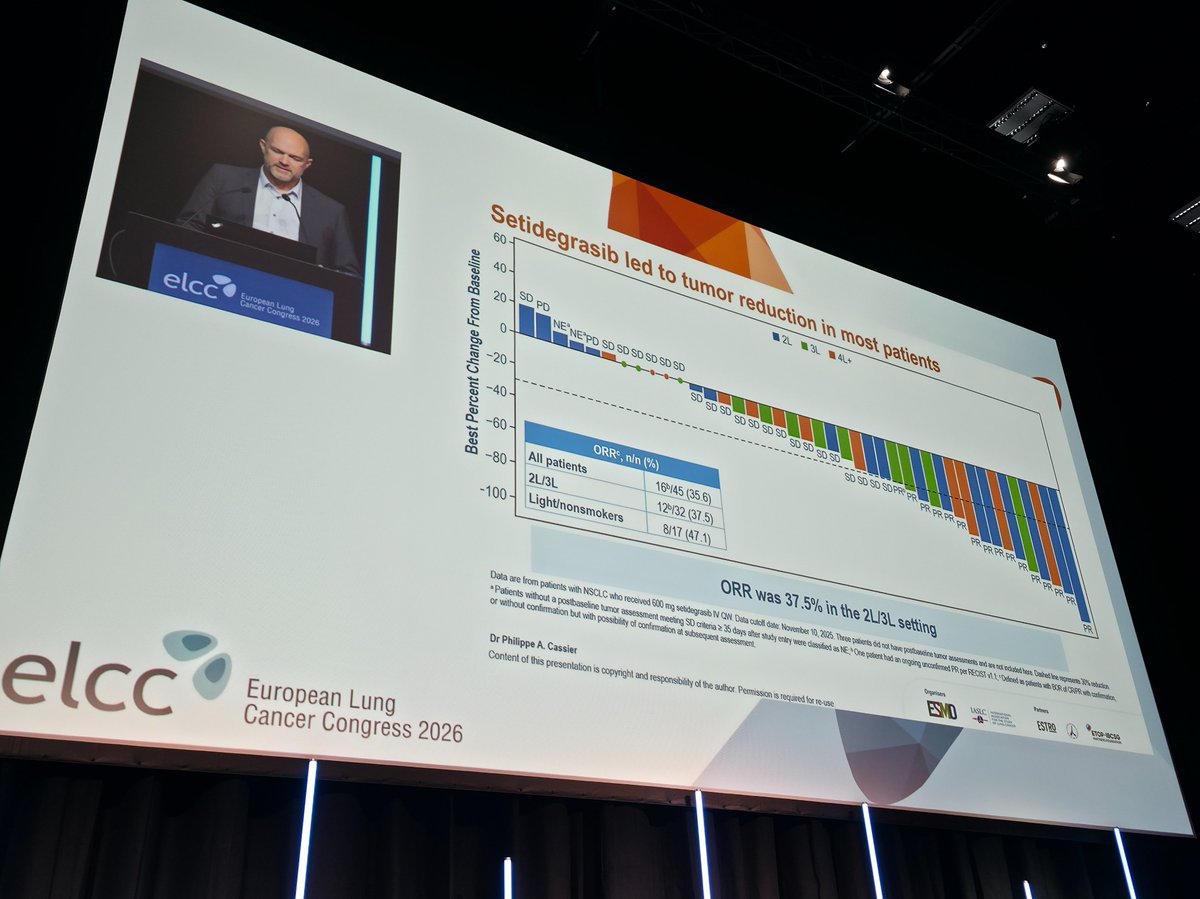
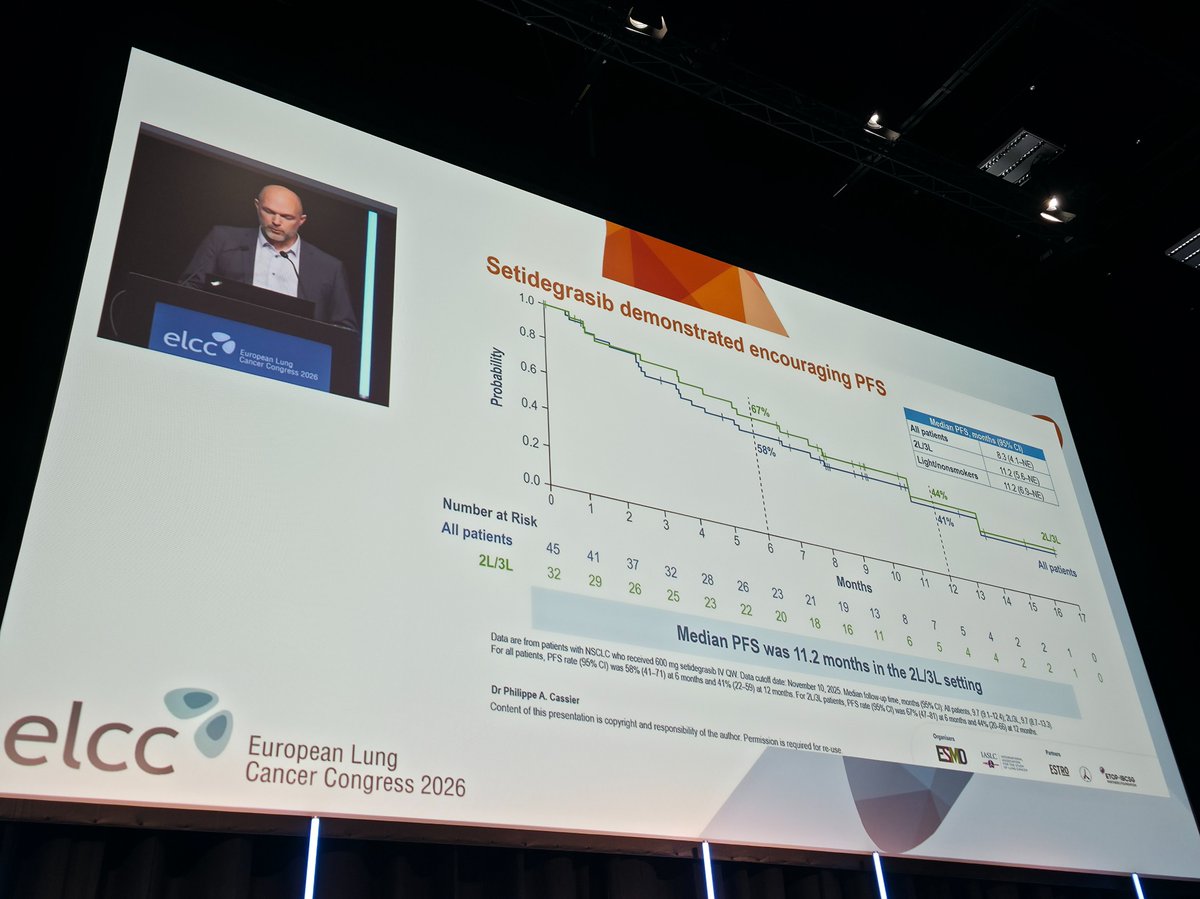
Efficacy / PFS (NSCLC, N=45) - Median PFS 8.3 months overall; approximately 11.2 months in the 2L/3L subgroup; objective response rate 35.6%, disease-control rate 84.4%.
Overall survival - Not mature at the October 9, 2025 data cutoff; OS is an exploratory endpoint in this Phase 1 study.
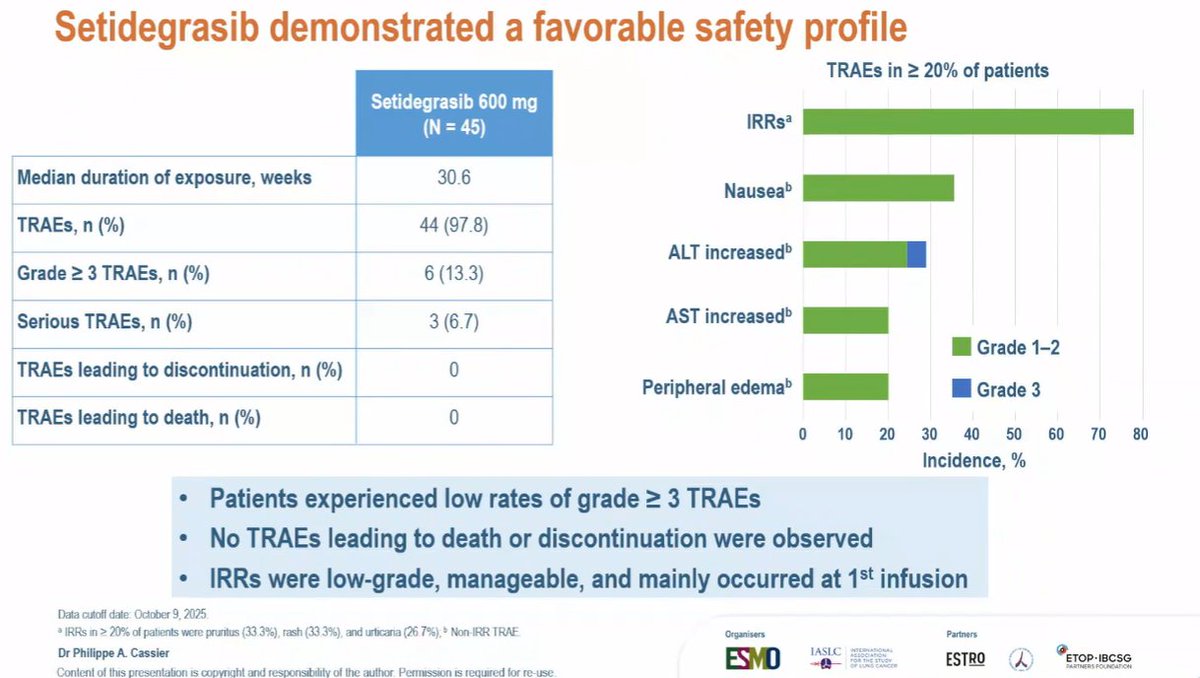
Safety - Median duration of exposure 30.6 weeks; treatment-related adverse events in 97.8% of patients, but grade 3 or higher in only 13.3% (6/45) - a favorable early tolerability profile.
Regulatory / sponsor - Investigational (Phase 1); setidegrasib is not FDA approved. Sponsor Astellas Pharma. Presented at ELCC 2026.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.














Top 10 by impressions — click to view on X
🔥 KRAS G12D finally druggable? First-in-human data for setidegrasib in advanced NSCLC #ELCC26 🧬 Study: Phase I (NCT05382559) 👥 Heavily pretreated KRAS G12D NSCLC (N=45) 💊...
Setidegrasib, novel KRAS G12D protein degrader reporting clinical meaningful outcomes with PFS of 11.2 m in 2/3L However there are KRAS G12D ON or ON/OFF inhibitors with activity. How to decide best...
🆙 #ELCC26 @myESMO 🇩🇰 🔥Proffered Paper session 1 ☑️Setidegrasib in KRAS G12D 🎯ORR 35.6%, mPFS 8.3m 🎙️Dr. Philippe CASSIER 🎙️Chair:...
Post-#ELCC26 clarity in one place 😉 🔗 From KRAS G12D degraders to ADC final OS, plus negative trials that matter (LATIFY) and practice-changing questions (i-TIMES, NorthStar)...
Cross tiral comparison for Kras G12d inhibitors. Nice slide 👌@esmo #elcc2026
🔁REVIEW #ELCC26 @myESMO 🇩🇰 🔥Proffered Paper session 1 ☑️Setidegrasib in KRAS G12D 🎯ORR 35.6%, mPFS 8.3m 🎙️Dr. Philippe CASSIER 📍NCT05382559 🆙 @OncoAlert...

📌Breakthrough in KRAS G12D NSCLC The undruggable era is over. Ph I data for Setidegrasib in pretreated NSCLC ☑️ORR 36.5% | mPFS 8.3–11.2 mo 🔁6-mo DoR ~76% 🧬 Early ctDNA drop → correlates with PFS...
Setidegrasib (NEJM 2026, Phase 1) degrades KRAS G12D. NSCLC: ORR 36%, PFS 8.3 mo Pancreas: ORR 24% A big step toward drugging KRAS G12D. #MVOnco #ELCC2026
Setidegrasib (KRAS G12D degrader) in pretreated NSCLC: ORR 35.6% | DCR 84.4% | mPFS 8.3 mo Weekly IV; manageable safety (IRRs common, no discontinuations). A new option for ~5%...

From the reality check on cronoimmunotherapy to the breakthrough of next-gen KRAS G12D degraders.🧬 Not everything at #ELCC2026 changes clinical practice, but these 5 clinical...
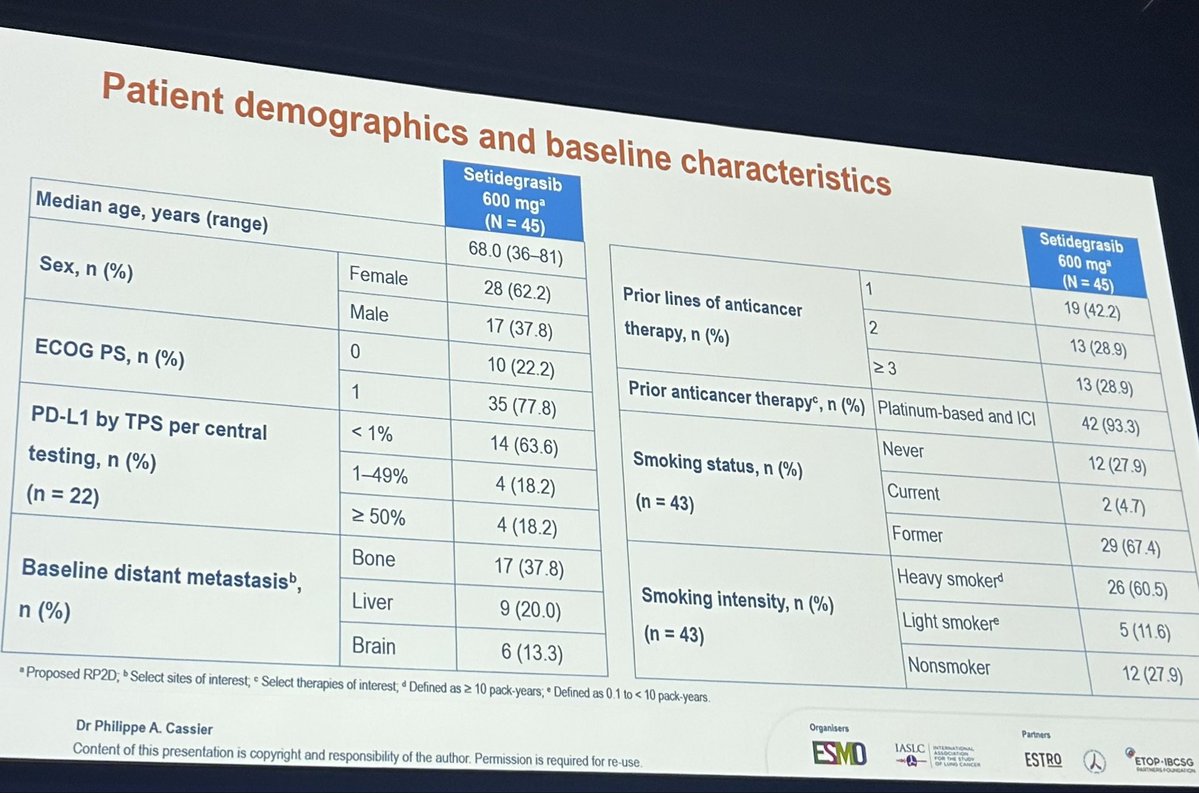
3082-CL-0101 (NCT05382559) is a Phase 1 dose-escalation and dose-expansion study evaluating setidegrasib, a novel KRAS G12D-targeted protein degrader, in patients with advanced solid tumors harboring KRAS G12D mutations. Unlike conventional KRAS inhibitors, setidegrasib degrades the KRAS G12D protein through a proteasome-mediated mechanism. The study enrolled 45 patients with heavily pretreated KRAS G12D-mutant NSCLC receiving setidegrasib 600 mg IV weekly.
Phase 1 dose-escalation and dose-expansion study (NCT05382559) of setidegrasib, a KRAS G12D protein degrader, administered as 600 mg IV weekly in patients with ECOG PS 0-2.
Patients with locally advanced unresectable or metastatic NSCLC harboring KRAS G12D mutations who had progressed on prior standard-of-care therapy (N=45). No prior pan-RAS or KRAS G12D inhibitors/degraders.
Setidegrasib 600 mg administered intravenously once weekly (IV QW). Dose escalation ranged from 140 mg to 800 mg, with 600 mg selected as the recommended Phase 2 dose (RP2D).
Primary endpoint: safety. Secondary endpoints: objective response rate (ORR), disease control rate (DCR), and duration of response (DOR) per RECIST v1.1. Exploratory endpoints: PFS, OS, pharmacodynamics.
Setidegrasib demonstrated a median PFS of 8.3 months in the overall NSCLC population (N=45). In the 2L/3L subgroup, median PFS was approximately 11.2 months. Early ctDNA molecular response (greater than or equal to 50% decrease in KRAS G12D VAF at Day 21) was strongly associated with PFS benefit (HR 0.12; 95% CI 0.03-0.46; p=0.0004), with median PFS of 9.6 months vs 2.6 months.
Overall survival data were not yet mature at the data cutoff (October 9, 2025). OS remains an exploratory endpoint in this Phase 1 study.
Setidegrasib demonstrated a favorable safety profile with median duration of exposure of 30.6 weeks. Treatment-related adverse events (TRAEs) occurred in 97.8% of patients, but grade 3 or higher TRAEs were observed in only 13.3% (6/45). Serious TRAEs occurred in 6.7%. Importantly, no TRAEs led to treatment discontinuation or death. The most common TRAEs (greater than 20%) were infusion-related reactions (IRRs), nausea, ALT increase, AST increase, and peripheral edema. IRRs were low-grade, manageable, and mainly occurred at the first infusion.
Setidegrasib represents a promising first-in-class KRAS G12D degrader with clinically meaningful activity in heavily pretreated NSCLC. The ORR of 35.6% and DCR of 84.4% in this difficult-to-treat population compare favorably with other emerging KRAS G12D-targeting agents. The strong ctDNA-PFS correlation (HR 0.12) may enable early response monitoring. This agent is investigational and not FDA-approved; further development in randomized trials is warranted.
3082-CL-0101 (NCT05382559) is a Phase 1, Astellas-sponsored first-in-human study of setidegrasib (development code ASP3082), a first-in-class KRAS G12D-selective degrader, in adults with KRAS G12D-mutant advanced solid tumors, with a focus on non-small cell lung cancer. It evaluates safety, tolerability, pharmacokinetics and preliminary anti-tumor activity.
In the NSCLC population (N=45), setidegrasib produced a median progression-free survival of 8.3 months overall and approximately 11.2 months in the second/third-line subgroup, with an objective response rate of 35.6% and a disease-control rate of 84.4%. Overall survival was not mature at the October 9, 2025 data cutoff.
No. Setidegrasib is an investigational KRAS G12D-selective degrader in Phase 1 development; it is not FDA approved for any indication. Its use in 3082-CL-0101 is investigational.
In 3082-CL-0101 the median duration of exposure was 30.6 weeks. Treatment-related adverse events occurred in 97.8% of patients, but grade 3 or higher treatment-related events were limited to 13.3% (6 of 45), indicating a manageable early safety profile for a first-in-class degrader.
KRAS G12D is one of the most common and historically undruggable KRAS mutations, particularly in pancreatic and lung cancers. Setidegrasib is a first-in-class G12D-selective degrader, and the clinically meaningful response and disease-control rates in heavily pretreated NSCLC make 3082-CL-0101 an early proof-of-concept for directly targeting KRAS G12D.
