[Slide 1]
ADEPPT: Single-arm Multicenter Phase Il trial
Screening, eligibility & enrolment
Trial treatment
PD
Follow-up
Primary endpoint:
Key eligibility criteria
Cohort A
Objective response rate by 12
Histologicalycyloloialy-confimed
Elderly (age 2 70 years)
weeks (12-week ORR)
stage IV NSCLC
(ECOG PS 0-1)
(RECIST v1.1)
KRAS
Adagrasib, 600 mg orally, twice daily, until
Prior systemic therapy for NSCLC
Secondary endpoints:
(e.g., platinum-based doublet
progression or unacceptable toxicity
Durable clinical benefit (DCB)
Cohort B
Time-to-progression (TTP)
chemotherapy and/or immune-
ECOG PS 2
Progression-free survival (PFS)
checkpoint inhibition or both)
(> 18 years)
Overall survival (0$)
Safety (CTCAE V5.0) and QoL
6 12 18 24 weeks Followed by every 9 weeks
Assumptions:
CT-scan + brain MRI
CT-scans
12-week ORR $ 15% vs 35%
1-sided alpha=2.5% power=80%
Patient-reported
Patient-reported outcome questionnaires
outcome questionnaire
every 6 weeks (+3 days, while on treatment)
Planned sample size:
48 patients (34 per cohort)
FFPE & blood
Blood
FFPE & blood
Organizers
Patients
ESMO
ASLC
Content of his presentation is copyright and responsibility of the author Permission is required for to ase
h
ETCP
ESTRO
Jarushka Naidoo
---
[Slide 2]
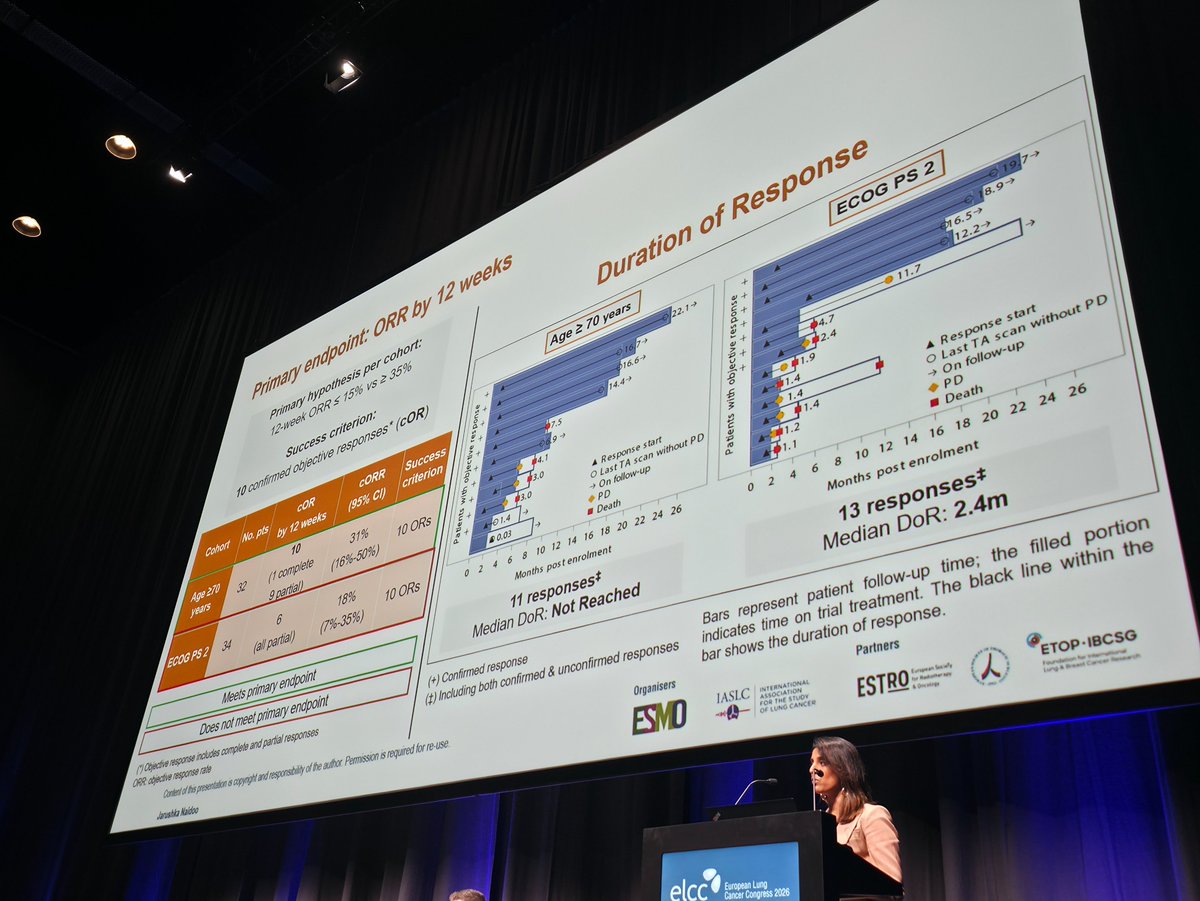
Primary endpoint: ORR by 12 weeks
Primary hypothesis per cohort:
12-week ORR $ 15% vs 2 35%
Success criterion:
Duration of Response
10 confirmed objective responses* (cOR)
Age 2 70 years
ECOG PS 2
2114
Cohort
No. pts
COR
CORR
Success
by 12 weeks
(16%-50%)
I I I I
PAST
(95% CI)
criterion
32
$4.1
years
10 ORs
9 partial)
I I 1
32%
FILE
Age 270
10
(1 complete
31%
Empose Hell
Last TA - what PO
Expense -
.
On Mary
Last LA - when PO
6
PO
ECOG PS 2
34
18%
Da blows
I
FO
(all partial)
10 ORs
(7%-35%)
I
.
1
1
1
10
12
14
.
-
.
24
26
.
I
'
.
I I I
-
12
14
.
:
I 1 I
Meets primary endpoint
11 responses
Median DoR: Not Reached
13 responses
Does not meet primary endpoint
Median DoR: 2.4m
(*) Objective response includes complete and partial responses
(+) Confirmed response
CRR: objective response rate
(1) Including both confirmed & unconfirmed responses
Bars represent patient blow-up time, the Net portion
Content of his presentation . copyright and responsibily If be author Permission 5 required for . inc
bar shows the duration If response
indicates time on the restitent, The black in when the
I
Jarishka Naidoo
I
ESMO
ARC
ESTRO
&
FROM -
---
[Slide 3]
Secondary endpoints: Quality of Life
Age 2 70 years
ECOG PS 2
16
a
#
Change from baseline in NFLSI-17 Total score
1
-
Better
17
.
23
04.10.81
1
16
1.5.
1
STAR
27
MO
АНД
41
0.05
12.60
4
-$1,
0.8
PRIORA
T
I
12
1.8
I
4548
.
0
.
12
.
-
16
Number of patients with Only -
- toban
1
(9*23)
23
"
15
1).
.
12
1
"
,
- of release - as -
0
- -
18
a
-
I
#
-
:
.
1
.
1
F
.
Weeks since treatment initiation
"
.
-
-
it.
- since revenued initiation
MO importance afference
Change minimal of then A 11 that number of - vin I OF date
Jurushka Maldoo
Content / his presentation . copyright and imporsibily if be author - 1 required for , - -
I
ESMD
ARC
ESTRO
b
non -
I
---
[Slide 4]
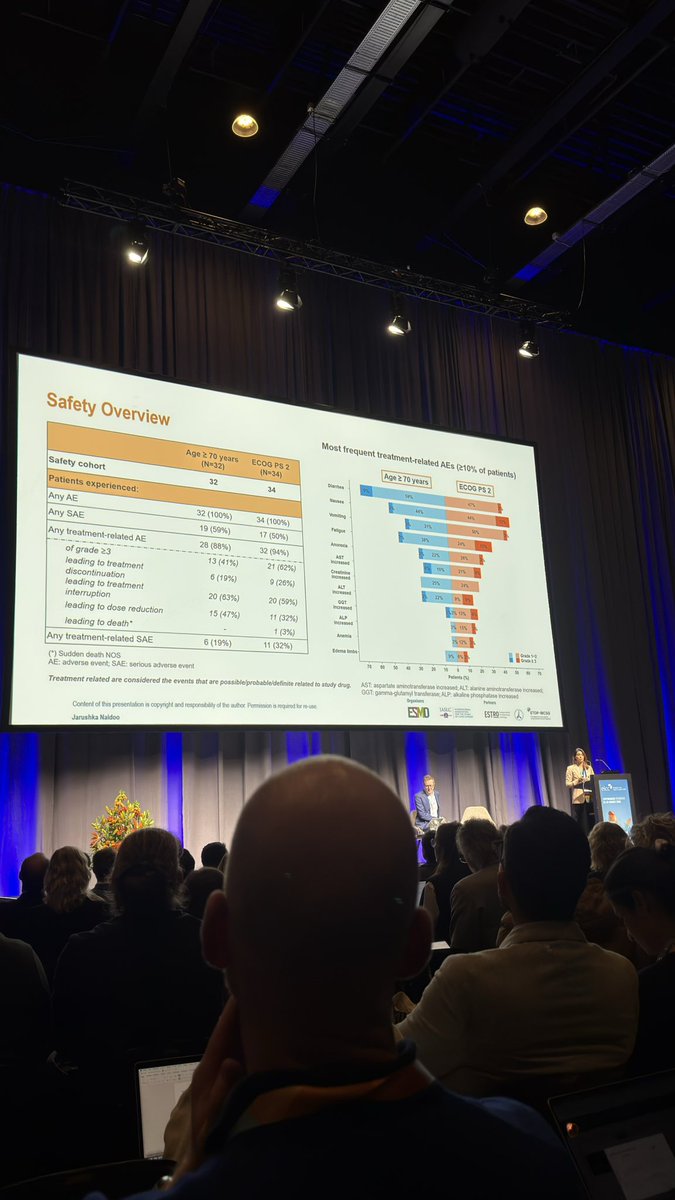
Safety Overview
Most frequent treatment-related AEs (>10% of patients)
Age 2 70 years
ECOG PS 2
Age 2 70 years
ECOG PS 2
(N=32)
(N=34)
I
Safety cohort
%
$
2
32
34
Names
Patients experienced:
5
$
I
Any AE
21%
is
32 (100%)
34 (100%)
I
Any SAE
as
in
7
19
(59%)
17 (50%)
-
2%
Any treatment-related AE
in
28 (88%)
32 (94%)
AST
increase
3
É
of grade 23
13 (41%)
21 (62%)
Creatine
leading to treatment
-
3
in
discontinuation
5(19%)
9(26%)
ALT
I
as
leading to treatment
n
interruption
20(63%)
20 (59%)
99T
notesed
7% 0%
leading to dose reduction
15 (47%)
11(32%)
->
incleased
% is
leading to death*
.
(3%)
I
e E S
Any treatment-related SAE
6 (19%)
11 (32%)
- timbe
a PS
Prade FE
(") Sudden death NOS
AE: adverse event, SAE: serious adverse event
N " 10 0 * a - I - n . 45 - " 70
Patients N
Treatment related are considered the events that are possible/probable/definie related to study drug.
AST aspartate aminotiransferate increased, ALT: alanize amindranslerase
GGT: transferate ALP: alkatine phosphatase increased
Department
Content of his presentation a copyright and responsibility il the author Permission , required or . HM
ESMO
ARE
Janushka Naldoo
ESTRO
Y
FOR 9C39
I
[Slide 1]
Most frequent treatment-related AEs (≥10% of patients
Safety Overview
ECOG PS 2
Age ≥ 70 years
ECOG PS 2
47%
Age ≥ 70 years
59%
(N=32)
(N=34)
Diarrhea
9%
44%
12%
44%
32
34
Nausea
Safety cohort
50%
3%
3%
31%
Vomiting
Patients experienced:
24%
15%
38%
32(100%)
34 (100%)
Fatigue
Any AE
3%
19(59%)
17(50%)
22%
26%
Any SAE
Anorexia
Any treatment-related AE
28 (88%)
32 (94%)
AST
6%
16%
21%
6%
increased
of grade 23
13(41%)
21 (62%)
Creatinine
25%
24%
increased
leading to treatment
discontinuation
6(19%)
9 (26%)
ALT
increased
%
22%
9%
9%
leading to treatment
20(63%)
20(59%)
GGT
interruption
increased
%3%
15%
6%
leading to dose reduction
15(47%)
11(32%)
ALP
increased
3%
15%
3%
leading to death*
.
1 (3%)
Anemia
Any treatment-related SAE
3% 12%
6(19%)
11(32%)
Edema limbs
(*) Sudden death NOS
9%
6%
3%
Grade 1-2
AE: adverse event SAE: serious adverse event
Grade 2 3
70
60
50
40
30
20
10
0
Treatment related are considered the events that are possible/probable/definit related to study drug.
10
20
30
40
50
Patients (%)
60
70
Jarushka Naidoo
Content of his presentation 5 copyright and responsibility of the author Permission is required for use
GGT: AST: aspartate gamma-glutamyl aminotransferase Organisers transferase; increased; ALP: alkaline ALT: phosphatase alanine aminotransferase increased increased;
Partners
ESMO
IASLC
INTERNATIONAL
FOR ASSOCIATION THE TUDY
or LUNG CANCER
ESTRO
I
L
ETOPIBCSG 1 I
longs -
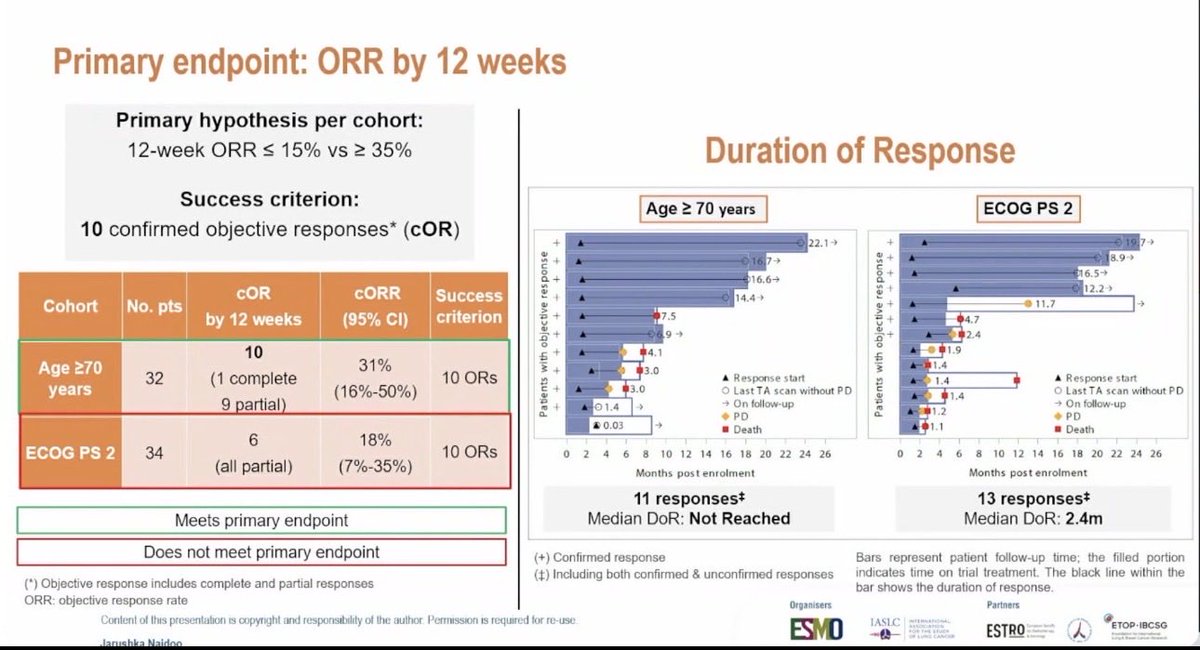
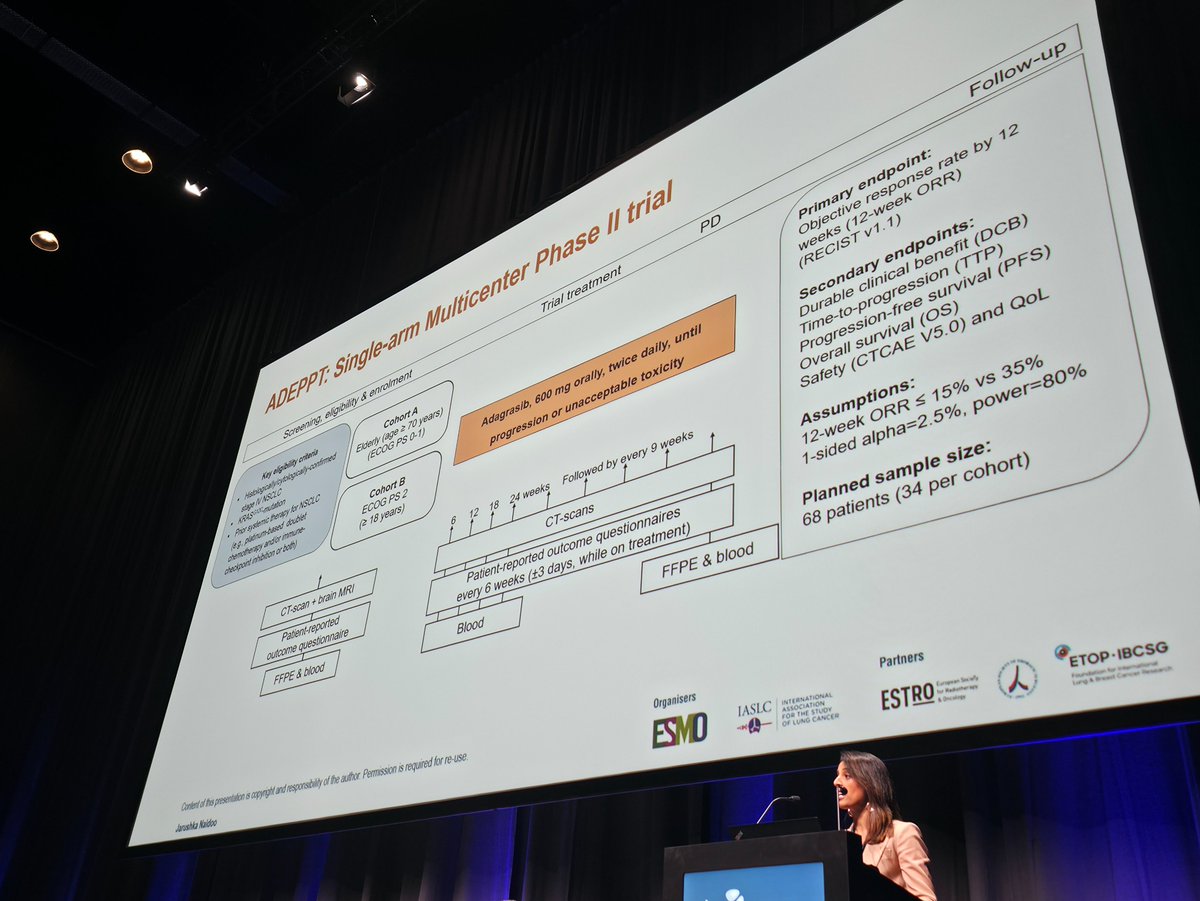
The ETOP ADEPPT trial is a single-arm, multicenter phase II study evaluating adagrasib (600 mg BID) in patients with KRAS G12C-mutant stage IV NSCLC who are elderly (aged 70 years or older with ECOG PS 0-1) or have poor performance status (ECOG PS 2). These patient populations are typically underrepresented in clinical trials. The primary endpoint was objective response rate (ORR) at 12 weeks by RECIST v1.1. The trial enrolled 66 patients across 21 centers (32 elderly, 34 PS2) and was conducted by ETOP-IBCSG in partnership with GECP. This is an investigational study; adagrasib is not FDA-approved in the perioperative or elderly/PS2 setting specifically studied in ADEPPT.
Single-arm, multicenter phase II trial with two cohorts (elderly and poor PS). Adagrasib 600 mg orally twice daily until progression or unacceptable toxicity. Primary hypothesis: 12-week ORR of 15% or less vs 35% or more, with one-sided alpha of 2.5% and 80% power.
Population
KRAS G12C-mutant stage IV NSCLC, pretreated (prior platinum-based chemotherapy and/or immune checkpoint inhibition). Cohort A: age 70 years or older, ECOG PS 0-1 (n=32). Cohort B: ECOG PS 2 (n=34). Median follow-up: 16.8 months (elderly) and 18.5 months (PS2).
Interventions
Adagrasib 600 mg orally, twice daily, continuous dosing until disease progression or unacceptable toxicity. CT scans plus brain MRI at screening, then CT scans every 6-9 weeks. Patient-reported outcome questionnaires every 6 weeks.
Primary Endpoints
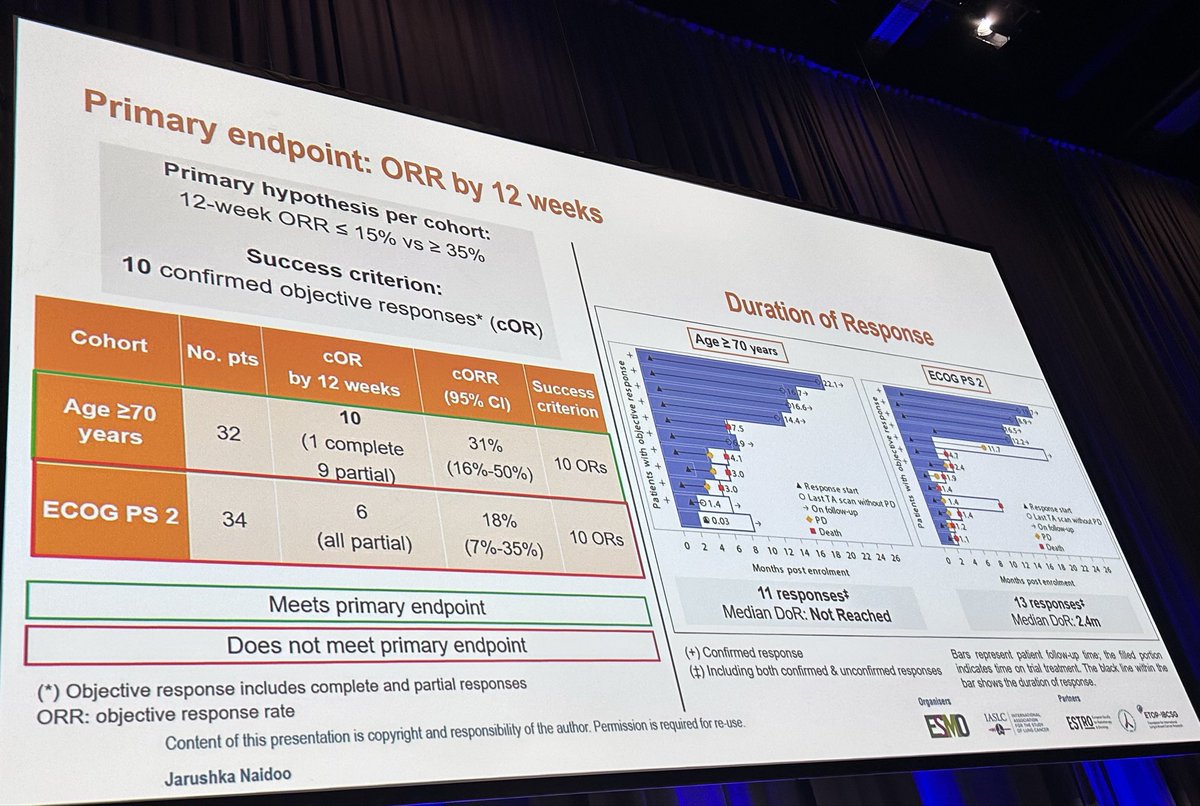
Objective response rate (ORR) at 12 weeks per RECIST v1.1. Success criterion: 10 or more confirmed objective responses per cohort. Secondary endpoints: durable clinical benefit (DCB), time-to-progression, PFS, OS, safety (CTCAE v5.0), and quality of life.
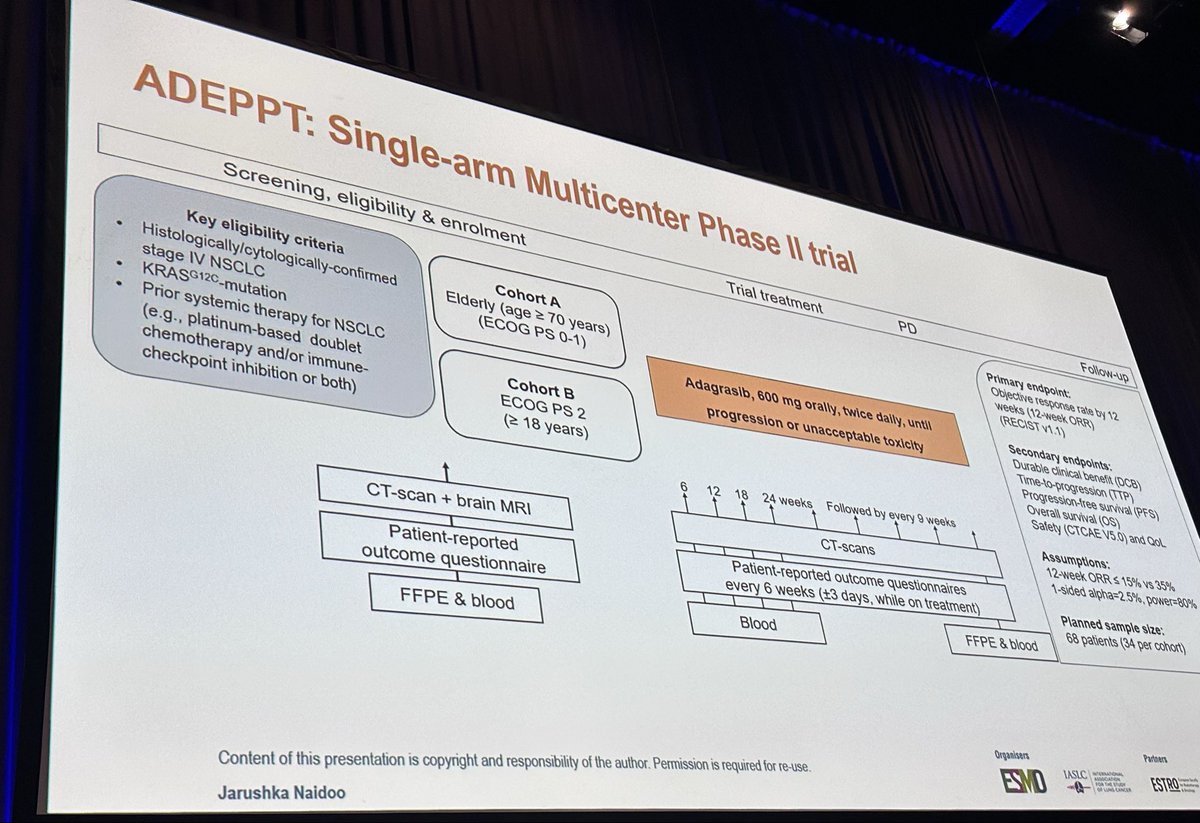
Efficacy - ORR at 12 Weeks (Primary Endpoint)
In the elderly cohort (age 70 or older), confirmed ORR at 12 weeks was 31% (95% CI: 16%-50%) with 10 objective responses (1 complete, 9 partial), meeting the primary endpoint success criterion. Median duration of response was not reached. In the ECOG PS 2 cohort, ORR was 18% (95% CI: 7%-35%) with 6 partial responses, which did not meet the primary endpoint. Median duration of response in the PS2 group was 2.4 months.
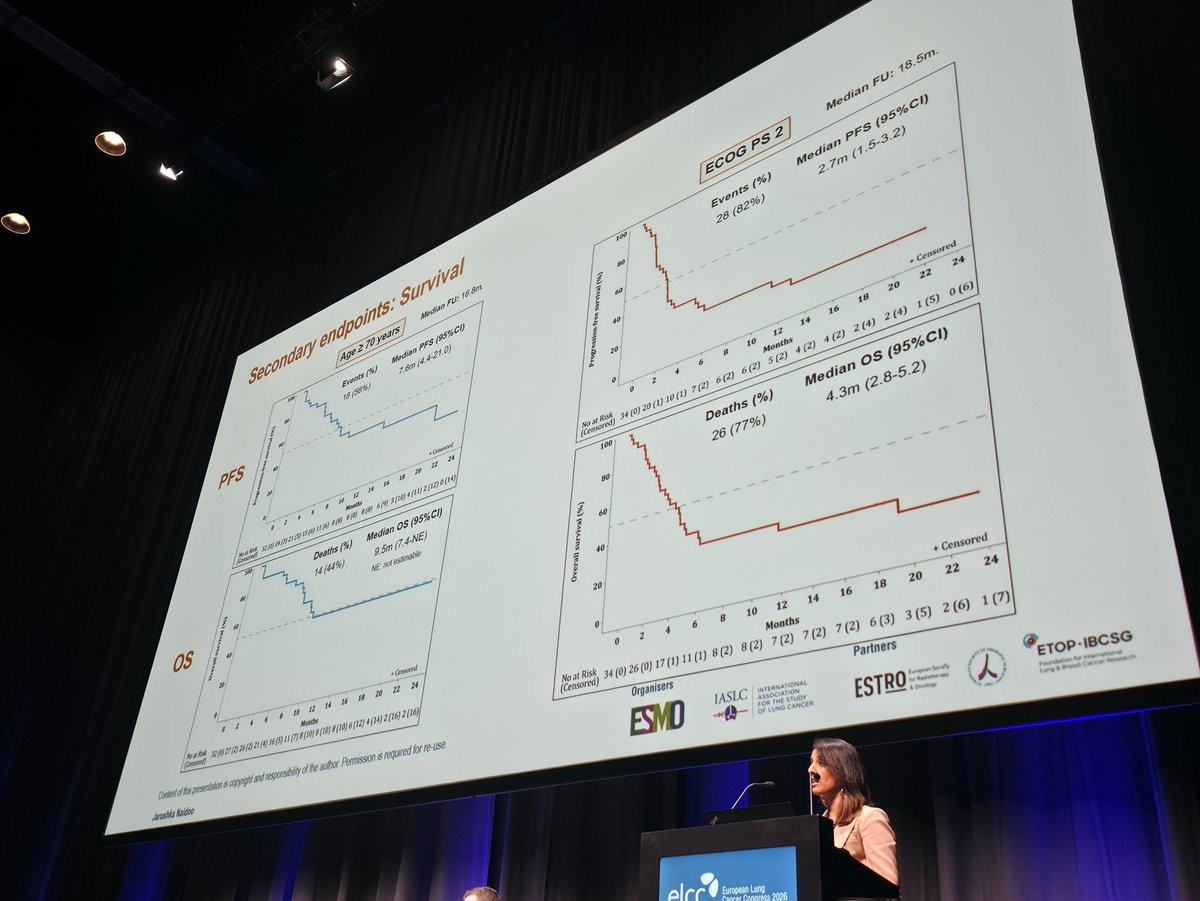
In the elderly cohort, median PFS was 7.6 months (95% CI: 4.4-21.0) with 56% events. Median OS was 9.5 months (95% CI: 7.4-NE). In the PS2 cohort, median PFS was 2.7 months (95% CI: 1.5-3.2) with 82% events. Median OS was 4.3 months (95% CI: 2.8-5.2) with 77% deaths. Survival outcomes were markedly worse in PS2 patients compared to the elderly cohort.
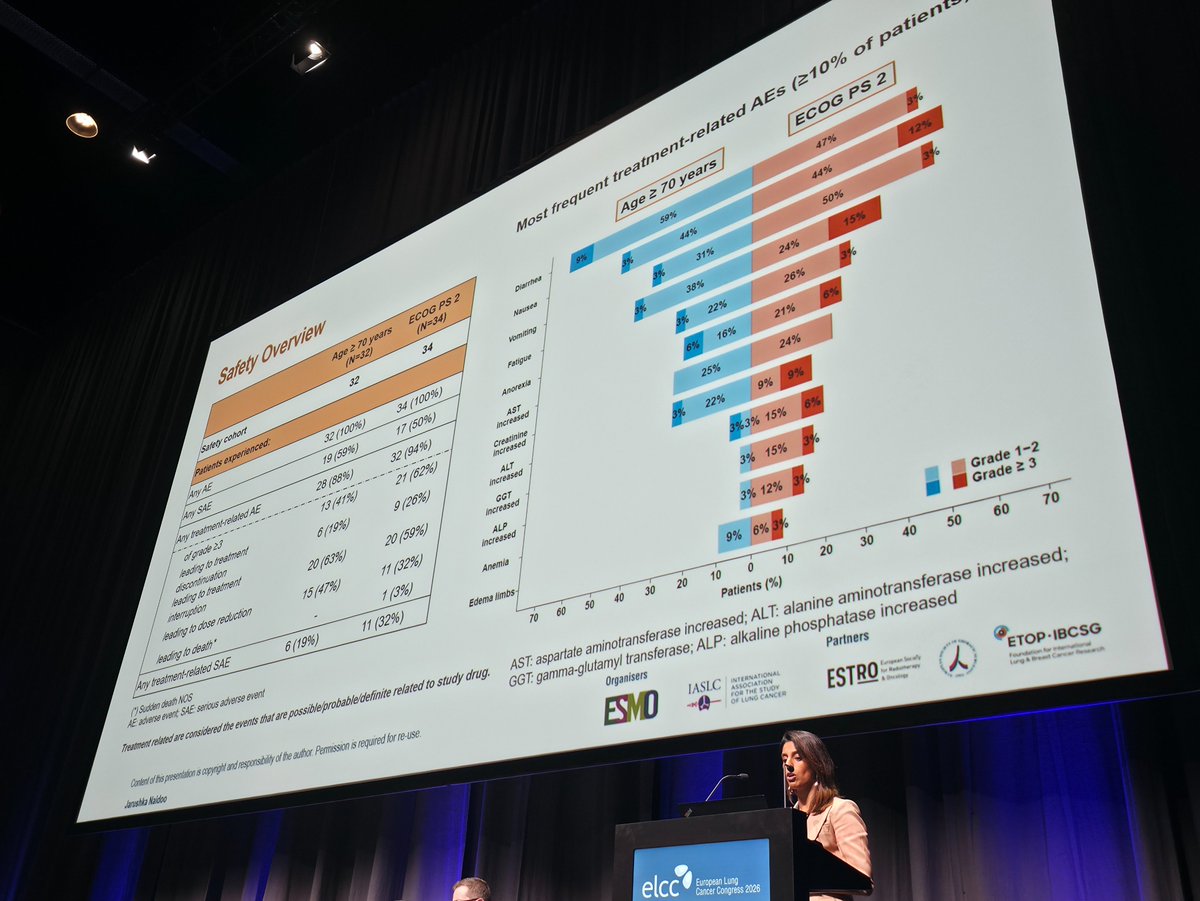
All patients in both cohorts experienced at least one adverse event. Treatment-related AEs occurred in 88% (elderly) and 94% (PS2) of patients. Grade 3 or higher TRAEs were reported in 41% (elderly) vs 62% (PS2). The most common TRAEs were diarrhea (44% in both), nausea (50% elderly, 31% PS2), and vomiting (24% elderly, 15% PS2). Treatment discontinuation due to toxicity occurred in 19% (elderly) vs 26% (PS2). One death (sudden death NOS) was reported in the PS2 cohort.
The ADEPPT trial provides the first prospective evidence for KRAS G12C inhibition in elderly and poor-performance-status NSCLC patients. Adagrasib at 600 mg BID appears feasible for elderly patients (age 70 or older) with ECOG PS 0-1, achieving a meaningful 31% ORR. However, the data raise caution for ECOG PS 2 patients, where the primary endpoint was missed (18% ORR), PFS/OS were short, and toxicity was substantial (62% grade 3+ TRAEs). KOLs have noted the need for dose optimization (potentially 400 mg BID) in PS2 patients and more detailed comprehensive geriatric assessment in elderly cohorts. This remains an investigational setting; adagrasib does not have specific FDA approval for these subgroups.