Inoperable T1-2N0M0 NSCLC -- Durvalumab + SBRT vs SBRT alone (AstraZeneca)
Discover KOL Sentiment on ASTEROID →Design - Phase 2 academic randomized trial of durvalumab (Imfinzi) + SBRT vs SBRT alone in inoperable early-stage T1-2N0M0 NSCLC (NCT03446547; Vastra Gotaland Region / Sahlgrenska; durvalumab supplied by AstraZeneca).
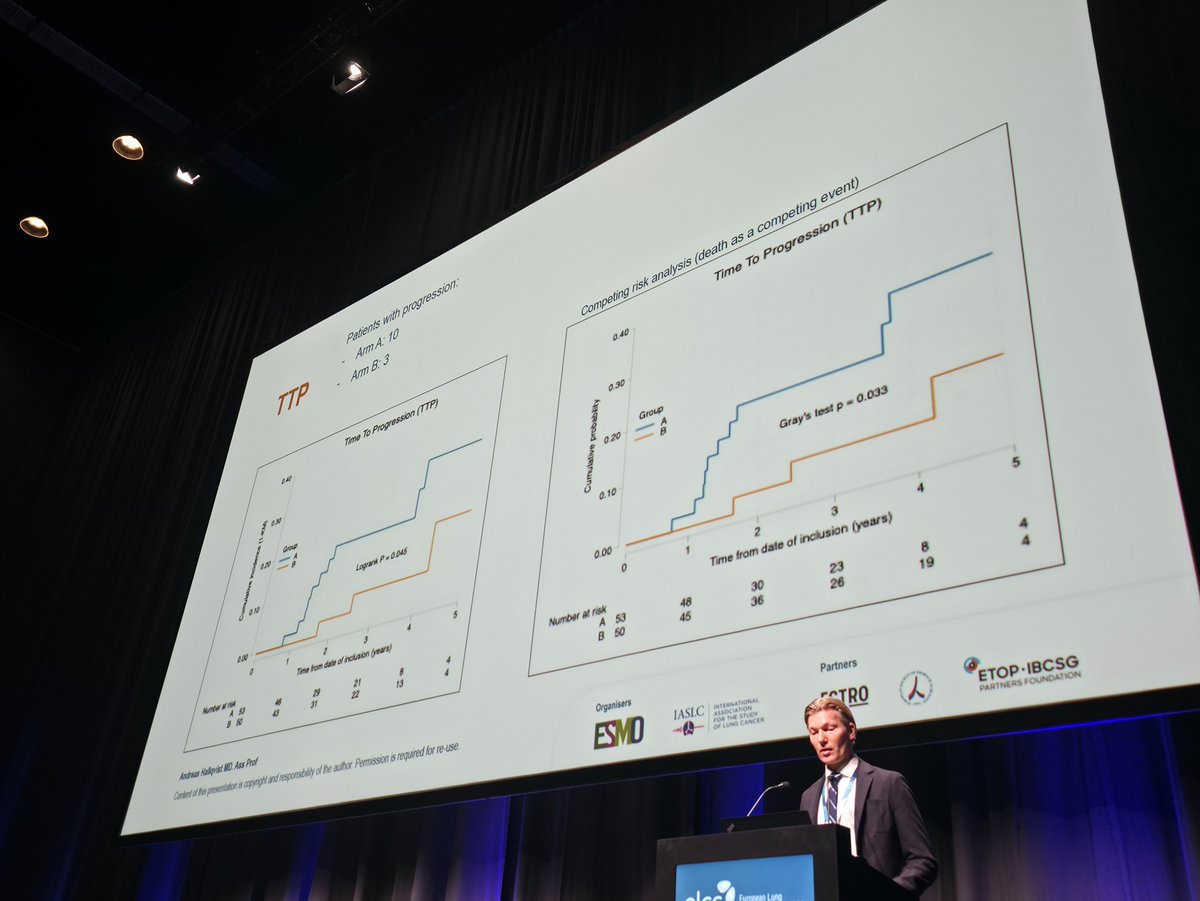
Time to progression (primary) - Signal toward improved TTP: fewer progression events with durvalumab (3) vs SBRT alone (10); p=0.054 - approaching but not reaching conventional statistical significance.
DFS / OS - No disease-free or overall-survival benefit observed; small sample size and Phase 2 design limit the ability to detect survival differences.
Safety - Manageable safety profile; the majority of adverse events were grade 1-2, consistent with the known profiles of durvalumab and SBRT, with no unexpected signals.
Interpretation - Preliminary evidence that durvalumab plus SBRT may improve local control, but the primary endpoint was not met at conventional significance; longer follow-up needed.
Regulatory / sponsor - Investigational; not FDA approved in this early-stage SBRT setting. Sponsor Vastra Gotaland Region; durvalumab (Imfinzi, AstraZeneca).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.




Top 5 by impressions -- click to view on X
#ELCC26 @myESMO @IASLC Mini Oral session 1 ASTEROID: SBRT +/- Durvalumab Time to progression was significantly improved by durvalumab Dr. Andreas Hallqvist Chair: @DocSacher Dr. Andreas Rimner NCT03446547
ELCC26 Day 2 Recap - Practice Signals Getting Sharper #ELCC26 ASTEROID Trial SBRT +/- Durvalumab (early-stage inoperable NSCLC) TTP signal (p=0.054) No DFS / OS benefit Mostly G1-2 toxicity Not practice-changing yet
Top Trials to Follow on Day 2 @myESMO #ELCC26 KANDLELIT-001 | ADEPPT | NORTHSTAR | ASTEROID | BeamionLung-1 | BECOME #ELCC #ELCC2026 #LungCancer #NSCLC
@myESMO #ELCC26: Top Trials from Day 2 ADEPPT | BeamionLung-1 | ASTEROID | NORTHSTAR | BECOME | KANDLELIT-001 | NCT02941458 #ELCC #ELCC2026 #LungCancer
SBRT + Durvalumab Improves Tumor Control in Early-Stage NSCLC At #ELCC2026, the #ASTEROIDtrial explores a key question: can immunotherapy enhance outcomes after SBRT? Fewer progression events: 3 vs 10
The ASTEROID trial (NCT03446547) is a randomized, open-label, phase II study evaluating the addition of durvalumab (anti-PD-L1) to stereotactic body radiation therapy (SBRT) in patients with inoperable, early-stage (T1-2N0M0) non-small cell lung cancer. The trial was presented at ELCC 2026 by Dr. Andreas Hallqvist and addresses a critical unmet need in patients who cannot undergo surgery but may benefit from immunotherapy combined with SBRT.
The study randomized patients to receive SBRT followed by durvalumab versus SBRT alone. The primary endpoint was time to progression (TTP). While durvalumab showed a signal toward improved TTP (p=0.054) with fewer progression events (3 vs 10), no statistically significant benefit was observed for disease-free survival (DFS) or overall survival (OS). The safety profile was manageable, with mostly grade 1-2 toxicities reported. Durvalumab is investigational in this early-stage SBRT setting and is not FDA-approved for this indication.
Randomized, open-label, phase II trial of SBRT followed by durvalumab versus SBRT alone in inoperable early-stage NSCLC (NCT03446547).
Patients with inoperable T1-2N0M0 non-small cell lung cancer eligible for SBRT. No biomarker selection or companion diagnostic required.
Experimental arm: SBRT followed by durvalumab (anti-PD-L1). Control arm: SBRT alone. AstraZeneca-sponsored.
Time to progression (TTP). Secondary endpoints included disease-free survival (DFS), overall survival (OS), and safety/tolerability.
The addition of durvalumab to SBRT showed a signal toward improved time to progression compared to SBRT alone. There were fewer progression events in the durvalumab arm (3 events) compared to the SBRT-alone arm (10 events). The p-value was 0.054, approaching but not reaching conventional statistical significance at the 0.05 threshold.
No benefit was observed for disease-free survival (DFS) or overall survival (OS) with the addition of durvalumab to SBRT. Data maturity and the small sample size of this phase II trial may limit the ability to detect OS differences. Longer follow-up will be needed to determine if the TTP signal translates into meaningful survival benefit.
The combination of durvalumab with SBRT showed a manageable safety profile. The majority of adverse events were grade 1-2 in severity. No unexpected safety signals were reported. The toxicity profile is consistent with what is known for both durvalumab monotherapy and SBRT in early-stage lung cancer.
The ASTEROID trial provides preliminary evidence that adding durvalumab to SBRT may improve local tumor control in inoperable early-stage NSCLC. However, the study did not meet its primary endpoint at conventional significance (p=0.054), and no DFS or OS benefit was demonstrated. KOL consensus at ELCC 2026 was that these results are not yet practice-changing. Durvalumab remains investigational in this early-stage SBRT setting and is not FDA-approved for this indication. Larger, randomized phase III trials will be needed to confirm whether immunotherapy has a role alongside SBRT in medically inoperable early-stage NSCLC.
ASTEROID (NCT03446547) is a Phase 2 academic randomized trial (sponsored by Sweden's Vastra Gotaland Region / Sahlgrenska, with durvalumab supplied by AstraZeneca) that tested whether adding durvalumab (Imfinzi) to stereotactic body radiotherapy (SBRT) improves outcomes versus SBRT alone in patients with inoperable early-stage (T1-2N0M0) non-small cell lung cancer.
ASTEROID showed a signal toward improved time to progression with durvalumab plus SBRT - fewer progression events (3 versus 10 with SBRT alone) - but the p-value of 0.054 did not reach conventional statistical significance. No benefit was seen for disease-free survival or overall survival, and the investigators noted that the small Phase 2 sample size limits the ability to detect survival differences.
No. Durvalumab combined with SBRT for inoperable early-stage NSCLC is investigational and not FDA-approved for this indication. Durvalumab (Imfinzi) is approved in other lung-cancer settings, but its early-stage SBRT use as tested in ASTEROID has not met the bar for approval.
The combination of durvalumab with SBRT showed a manageable safety profile, with the majority of adverse events being grade 1-2. No unexpected safety signals were reported, and the toxicity profile was consistent with what is known for both durvalumab monotherapy and SBRT in early-stage lung cancer.
ASTEROID provides preliminary evidence that adding durvalumab to SBRT may improve local tumor control in inoperable early-stage NSCLC, but because the primary time-to-progression endpoint was not met at conventional significance (p=0.054) and no survival benefit was shown, KOL consensus at ELCC 2026 was that the approach requires larger, confirmatory studies before it could change practice.