













Top 10 by impressions - click to view on X
“More than half of patients (60%) with advanced lung cancer who took lorlatinib were still alive five years later with no progression of disease, data presented at the world’s largest cancer...
@StephenVLiu @bensolomon1 No matter what @VPrasadMDMPH may say, these results are outstanding and never seen before in lung cancer, ever!
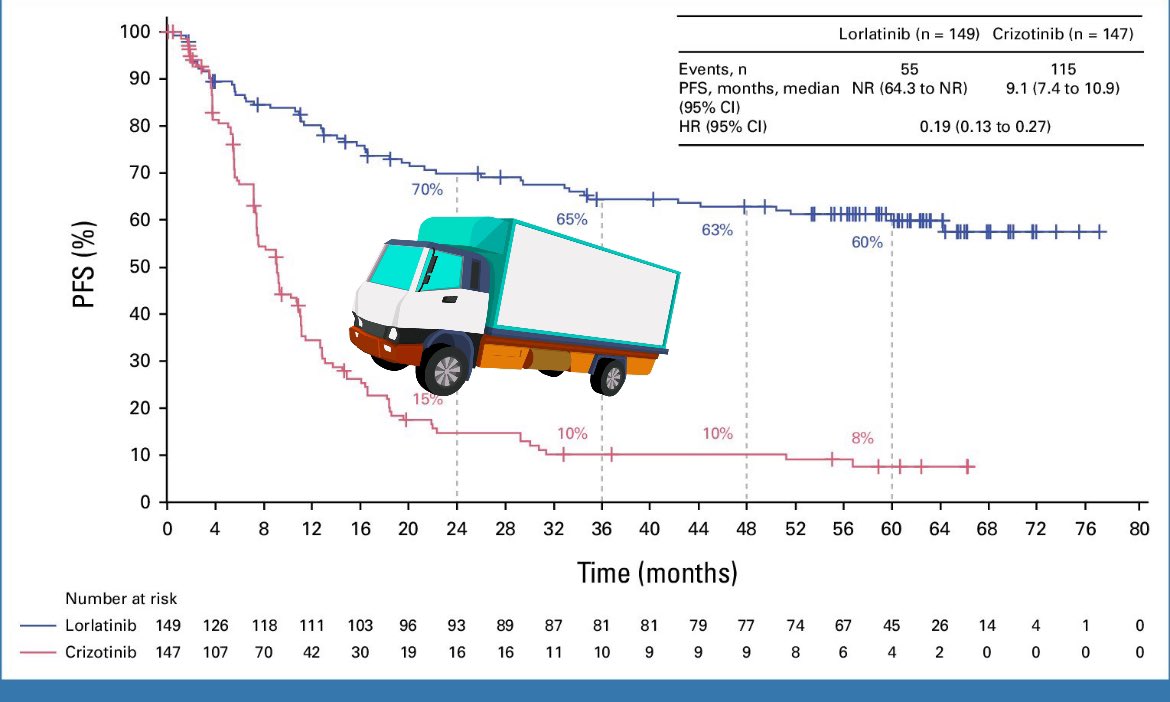
Truck test ✅ #CROWN #lcsm
So, 5y PFS is out. CROWN shows that only 3% of patients had disease progression from year 4 to year 5. Toxic, Lorlatinib is indeed, but this in totally unprecedented in thoracic oncology. ALK fusion...
Let’s take a minute. Have we seen anything like this in NSCLC before? mPFS NR at 5 years? 👏🏽👏🏽👏🏽👏🏽 These curves are very impressive, and should urge us to think about management of AEs and optimize...

Not to steal the thunder from the oral session today, but this is the CROWN PFS curve, more or less flat between 2-5 years and still 60% progression free at 5 years! #ASCO24...

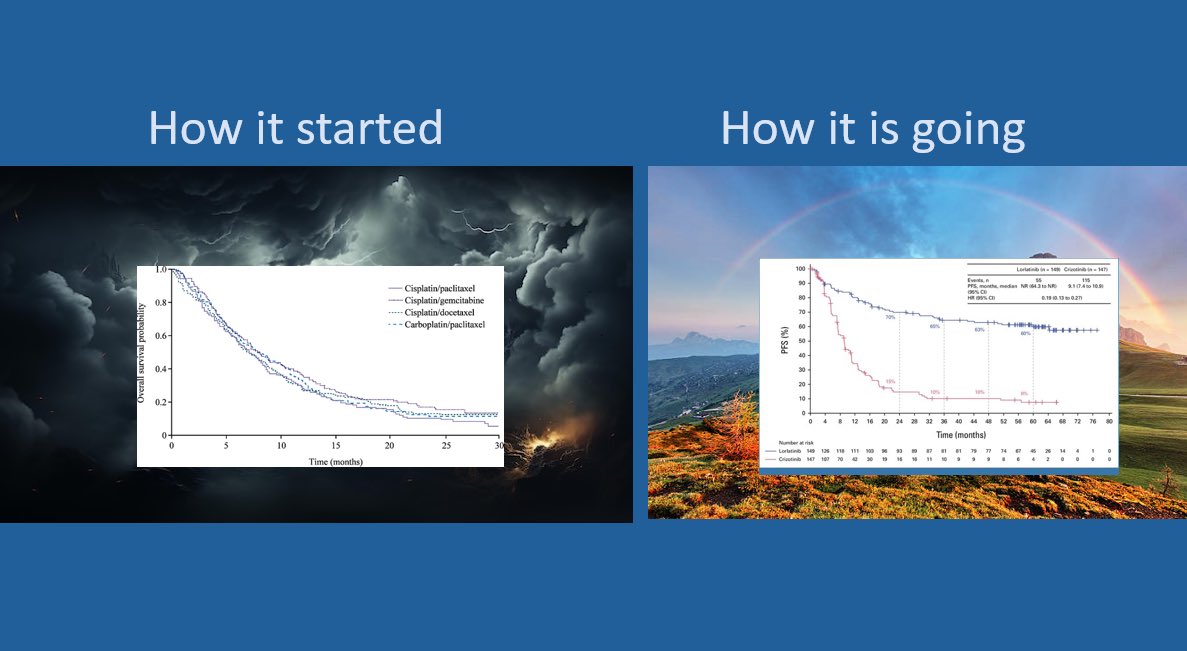
#ASCOLung How it started How it is going
Its great to see #asco24 changing language. In the future, I would love to see @asco make sure All randomized studies use appropriate control arms (sorry CROWN) All RCTs...
The curve again! 👑 #ASCO24 @ASCO

#ASCO24 CROWN study: lorlatinib vs crizotinib Lorlatinib..... no need to comment, look at the curves👇 Presented by Dr. @bensolomon1 👏👏 @OncoAlert
CROWN is a landmark Phase III, randomized, open-label trial that established lorlatinib (Lorbrena) as the standard of care for first-line treatment of ALK-positive metastatic NSCLC. The trial randomized 296 treatment-naive patients 1:1 to lorlatinib 100 mg once daily or crizotinib 250 mg twice daily, demonstrating unprecedented progression-free survival exceeding 5 years. CROWN represents the longest PFS ever reported with any single-agent molecular targeted treatment across all metastatic solid tumors.
Phase III, global, multicenter, randomized, open-label, parallel 2-arm trial in treatment-naive patients with ALK-positive advanced or metastatic NSCLC. ALK rearrangements were identified by the Ventana ALK (D5F3) CDx immunohistochemical assay.
Adults with previously untreated ALK-positive advanced or metastatic NSCLC, ECOG performance status 0-2. Patients were randomized 1:1 (149 lorlatinib, 147 crizotinib). Both patients with and without baseline brain metastases were enrolled (35 lorlatinib, 38 crizotinib had brain metastases at baseline).
Lorlatinib 100 mg orally once daily versus crizotinib 250 mg orally twice daily in 28-day cycles. Median treatment duration with lorlatinib was 57.0 months.
Primary endpoint: progression-free survival (PFS) based on Blinded Independent Central Review (BICR). Secondary endpoints: investigator-assessed PFS, overall survival (OS), objective response rate (ORR), intracranial objective response (IOR), and safety.
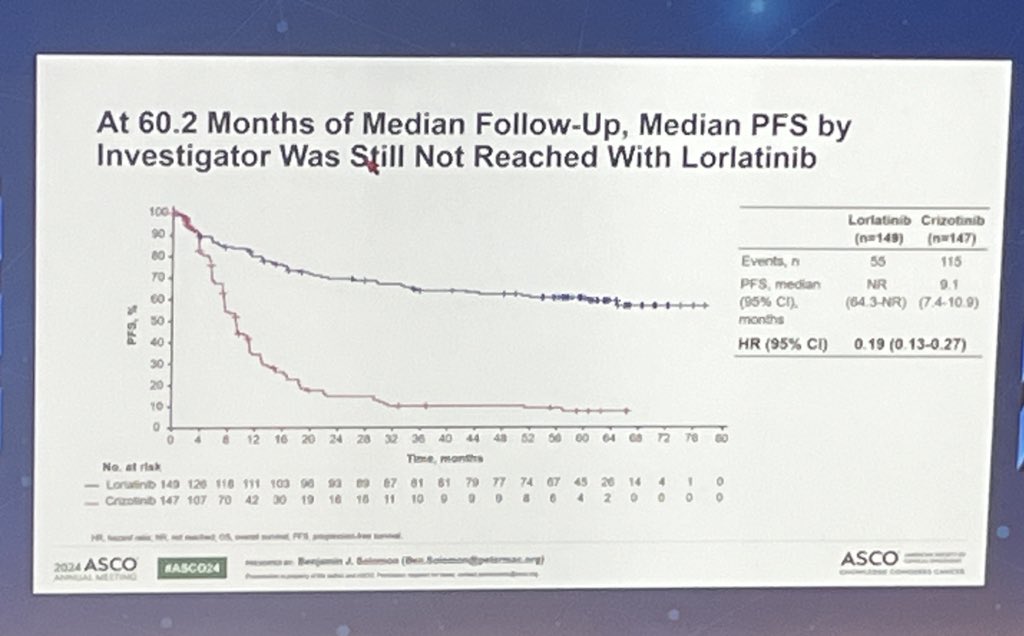
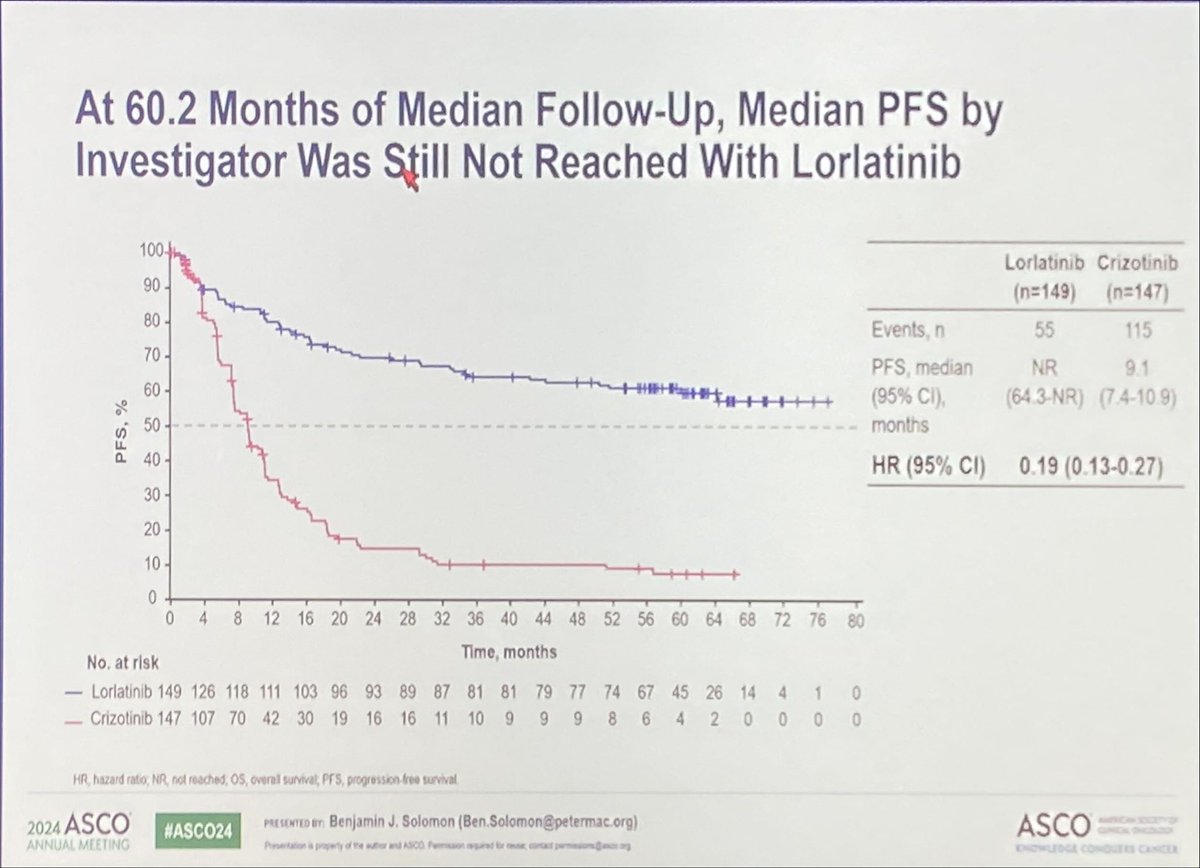
After a median follow-up of 60.2 months, PFS HR was 0.19 (95% CI: 0.13-0.27), representing an 81% reduction in the risk of disease progression or death. Median PFS was not reached with lorlatinib (95% CI: 64.3-NR) versus 9.1 months (95% CI: 7.4-10.9) with crizotinib. The 5-year PFS rate was 60% with lorlatinib versus 8% with crizotinib. ORR was 81% (95% CI: 73-87) with lorlatinib versus 63% (95% CI: 54-70) with crizotinib.
Overall survival data were not yet mature at the 5-year analysis. In the pivotal phase I/II study, with a median OS follow-up of 72.7 months, median OS was not reached with lorlatinib, and 5-year OS was 76% (95% CI: 57-88) in treatment-naive ALK-positive NSCLC patients (n=30).
Grade 3/4 AEs occurred in 77% of lorlatinib patients versus 57% with crizotinib, primarily driven by laboratory abnormalities. Hypercholesterolemia occurred in 72% (20% Grade 3), hypertriglyceridemia in 66% (17% Grade 3, 8% Grade 4), requiring lipid-lowering medication initiation in 83% of patients. CNS effects occurred in 52% (cognitive 28%, mood 21%, psychotic 7%), mostly Grade 1-2. Weight gain occurred in 44% (23% Grade 3). Treatment-related permanent discontinuation was only 5%.
CROWN established lorlatinib as the preferred first-line treatment for ALK-positive metastatic NSCLC, with 5-year PFS of 60% representing a transformative outcome that approaches chronic disease management. The intracranial efficacy is particularly noteworthy, with 92% freedom from brain progression at 5 years, addressing a critical unmet need in ALK-positive NSCLC. Key clinical debates include the unique toxicity profile (hyperlipidemia, CNS effects, weight gain) versus second-generation ALK TKIs, optimal TKI sequencing strategies, and long-term cardiovascular implications of sustained hyperlipidemia management.














































