Immunotherapy Timing in Advanced NSCLC - Does time of day of ICI infusion affect overall survival? ETOP-Roche propensity-score matched meta-analysis of 8 international RCTs.
Visit Interactive Trial Page →









Top 10 by impressions - click to view on X
Does time of immunotherapy infusion matters ? No . Opposite results from asco 2025 presentation. Looking forward to full presentation. LBA2 iTIMES @myESMO #ELCC2026...
✨THE proffered paper session 2 at #ELCC26: i-TIMES study in 🫁 cancer! Does the time of day of ICI infusion really matter? 🎯 Primary endpoint met: late ICI was non-inferior to early...
Plot twist: Turns out timing might NOT be everything (even for ICI). At #ELCC26, i-TIMES asks: does when you give ICI matter? ▫️HR late v early: 1.04 (0.93–1.17) ▫️OS: 17.3 mo...
🔜 #ELCC26 @myESMO 🇩🇰 🔥Proffered Paper session 2 ☑️CT screening in non-risk-based population ☑️LATIFY: ceralasertib + durvalumab ☑️ETOP-Roche i-TIMES: immunotherapy...
It’s over…
🔥 Does timing of immunotherapy during the day matter? #ELCC26 LBA2 - i-TIMES study explores early vs late ICI dosing in advanced lung cancer 👇 🧬 Study...
🆙 #ELCC26 @myESMO 🇩🇰 🔥Proffered Paper session 2 ☑️ETOP-Roche i-TIMES: Immunotherapy Timing 🎯No difference observed by timing 🎯mOS Early/Late 17.3m vs. 16.0m, HR 1.039 (95%CI...
🔥💉 Immunotherapy timing does NOT impact survival - morning 🌅 vs afternoon 🌙 makes no difference #ELCC26 LBA2 - i-TIMES answers a long-standing chronotherapy question in lung cancer...

#ELCC26 📢The “morning vs afternoon” debate in immunotherapy may be over. i-TIMES shows: 📊 No meaningful OS difference Earlier signals… didn’t hold up @OncoAlert...

The debate continues regarding the benefits and timing of immunotherapy infusions. Non -inferiority of late vs early administration (i-TIMES study). Reassuring for our current clinical...
The i-TIMES study (Immunotherapy Timing) is a propensity-score matched meta-analysis investigating whether the time of day of immune checkpoint inhibitor (ICI) infusion affects overall survival in patients with advanced or metastatic lung cancer. The study pooled data from 8 international Roche-sponsored randomized clinical trials, classifying ICI administration as Early (before 12:00 PM) or Late (after 12:00 PM) based on the starting time of the first 2 cycles. This ETOP-Roche collaboration, presented by Solange Peters at ELCC 2026, was designed as a non-inferiority analysis to determine whether later-in-the-day ICI dosing compromises outcomes.
Propensity-score matched meta-analysis of 8 international Roche-sponsored phase II/III RCTs with at least one ICI arm and OS as a primary endpoint. Non-inferiority design with pre-specified 95% CI upper limit of 1.18, tested at one-sided alpha 2.5% with 80% power.
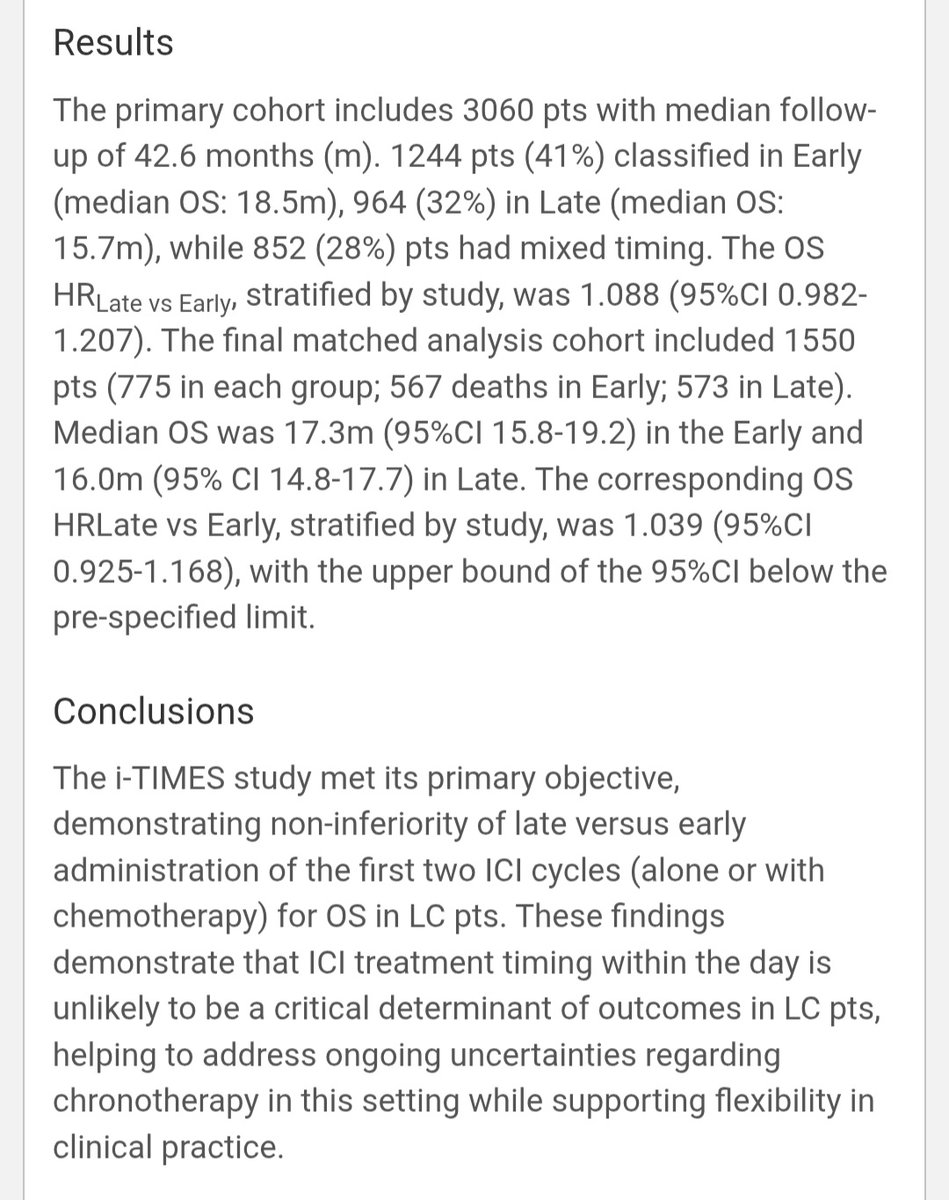
3,060 patients with advanced/metastatic lung cancer who received at least 2 cycles of ICI with available timing data. 1,244 patients (41%) classified as Early, 964 (32%) as Late, and 852 (28%) had mixed timing. Final matched cohort: 1,550 patients (775 per group).
ICI administered alone or in combination with chemotherapy. Early group: ICI infusion started before 12:00 PM. Late group: ICI infusion started after 12:00 PM. Classification based on first 2 cycle start times.
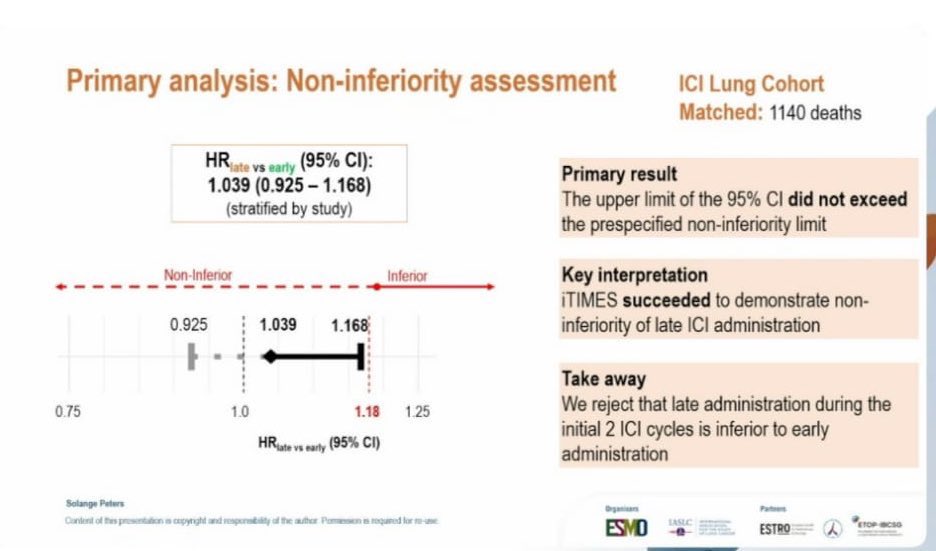
Primary endpoint: overall survival (OS), assessed as non-inferiority of Late vs. Early ICI administration. Required 1,147 events. Non-inferiority margin set at HR upper bound of 1.18.
The i-TIMES study focused on overall survival as the primary endpoint. No separate PFS analysis was presented in the primary results. The study design centered on whether late ICI administration was non-inferior to early administration for OS.
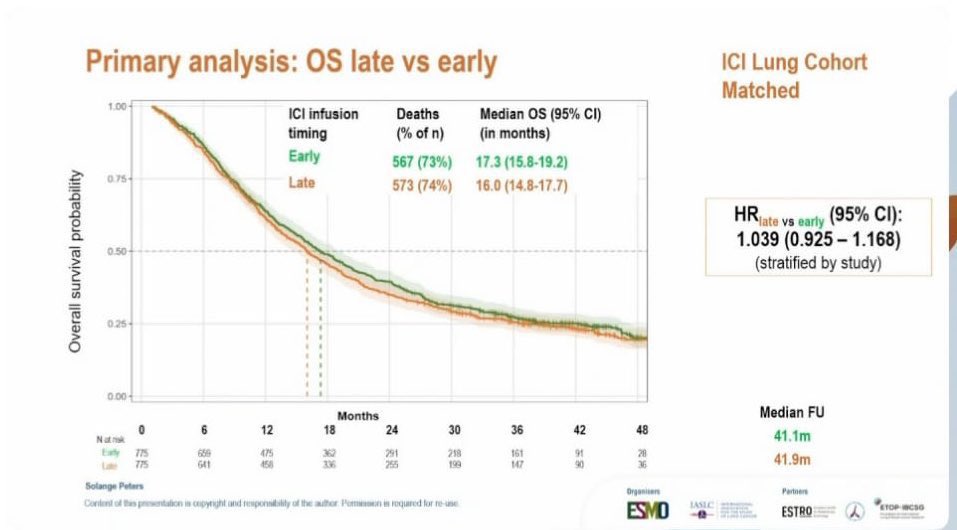
The study met its primary objective. In the matched cohort (n=1,550), median OS was 17.3 months (95% CI 15.8-19.2) in the Early group vs. 16.0 months (95% CI 14.8-17.7) in the Late group. The OS HR Late vs. Early, stratified by study, was 1.039 (95% CI 0.925-1.168), with the upper bound below the pre-specified non-inferiority margin of 1.18.
The i-TIMES study was a meta-analysis of ICI timing and did not report separate safety or tolerability data. The focus was exclusively on OS outcomes by time of infusion. No differential adverse event profiles by timing were presented.
The i-TIMES results support a flexible and pragmatic approach to ICI scheduling without compromising clinical outcomes. ICI treatment timing within the day is unlikely to represent an independent determinant of efficacy in lung cancer patients. The investigators noted that any potential chronotherapy effect appears limited in magnitude and of uncertain clinical relevance. This study directly addresses — and largely resolves — prior conflicting signals from retrospective analyses suggesting morning immunotherapy superiority.