DLL3-expressing SCLC/NEC -- Obrixtamig (DLL3xCD3 bispecific) + Ezabenlimab (anti-PD-1) -- Boehringer Ingelheim
Visit Interactive Trial Page →






Top 4 by impressions -- click to view on X
Today presentation #ELCC26 phase 1 of Obrixtamig + ezabenlimab in SCLC, LCNEC or other NECs Overall: ORR 30%, DCR 58%, mPFS 4.4m Highest dose: ORR 58%, DCR 83%, mPFS 10m SCLC: ORR 33%, PFS 5.7 m. @OncoAlert @CHUdeToulouse @IUCTOncopole
NEW #ELCC26 @myESMO Proffered Paper session 1 Obrixtamig + ezabenlimab in SCLC or NECs Overall: ORR 30%, DCR 58%, mPFS 4.4m Highest dose: ORR 58%, DCR 83%, mPFS 10m @JulienMazieres Chair: @peters_solange NCT05879978
Congrats @JulienMazieres on the great presentation and the encouraging results for our lung NETs. Really impressive study testing the combination in all the different neuroendocrine tumor subtypes! #SCLC #ELCC2026
REVIEW #ELCC26 @myESMO Proffered Paper session 1 Obrixtamig + ezabenlimab in SCLC or NECs Overall: ORR 30%, DCR 58%, mPFS 4.4m Highest dose: ORR 58%, DCR 83%, mPFS 10m @JulienMazieres NCT05879978
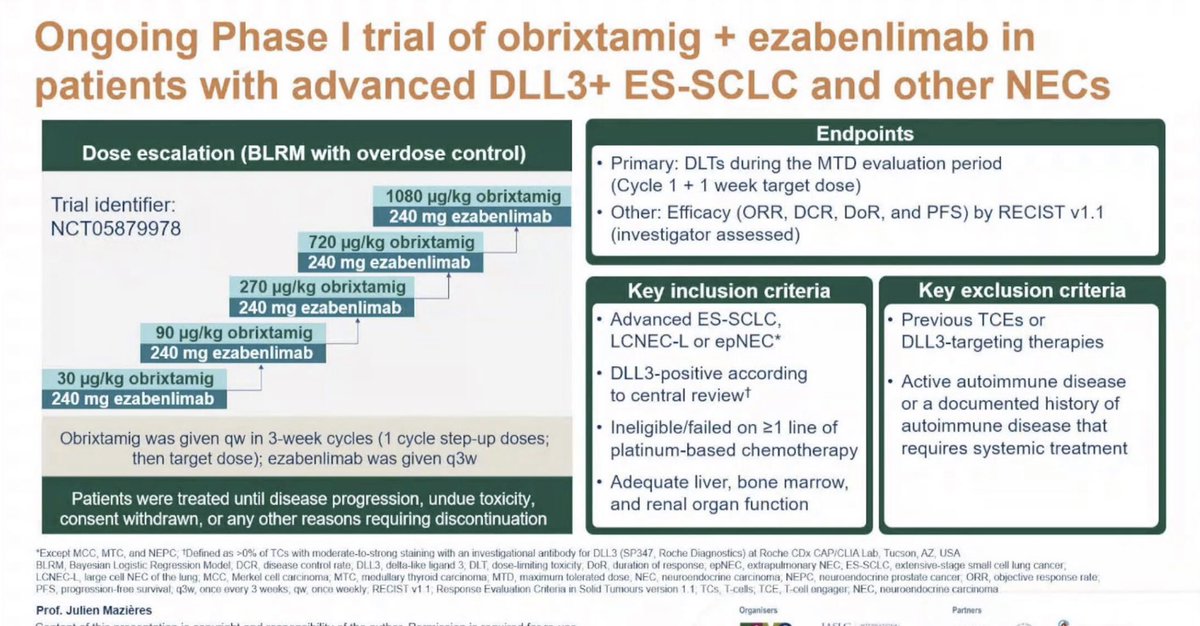
NCT05879978 is an ongoing phase I dose-escalation trial evaluating obrixtamig, a novel IgG-like DLL3-targeted T-cell engager (bispecific antibody), in combination with ezabenlimab (anti-PD-1) in patients with advanced DLL3-expressing extensive-stage small cell lung cancer (ES-SCLC), large cell neuroendocrine carcinoma of the lung (LCNEC-L), and extrapulmonary neuroendocrine carcinomas (epNEC). The study was presented by Prof. Julien Mazieres at ELCC 2026 as a Proffered Paper. Obrixtamig binds simultaneously to DLL3 on cancer cells and CD3 on T-cells, creating an MHC-independent cytolytic synapse. Preclinical data showed that obrixtamig upregulates PD-1 and PD-L1, providing the rationale for combining with the anti-PD-1 antibody ezabenlimab to potentially enhance antitumor activity.
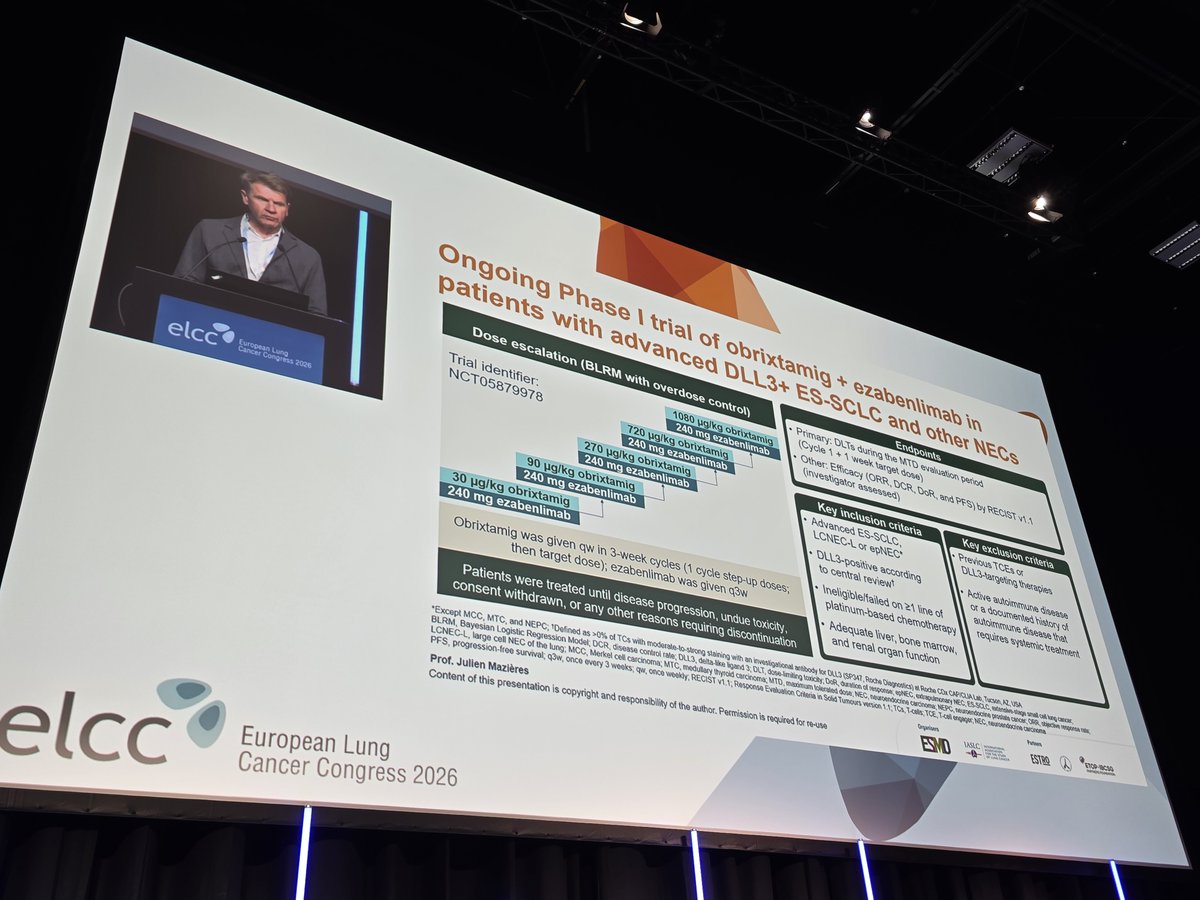
Phase I dose escalation using a Bayesian Logistic Regression Model (BLRM) with overdose control. Obrixtamig administered weekly in 3-week cycles (1 cycle step-up doses, then target dose); ezabenlimab given every 3 weeks (q3w). Five dose cohorts: 30, 90, 270, 720, and 1080 mcg/kg obrixtamig with 240 mg ezabenlimab.
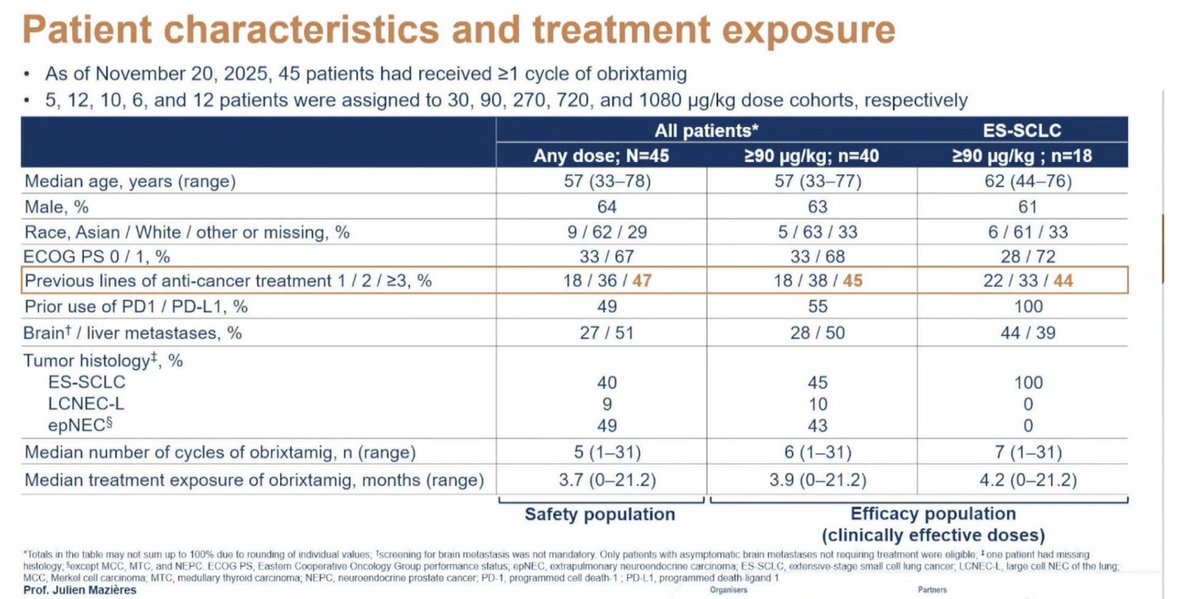
45 patients with advanced DLL3-positive ES-SCLC, LCNEC-L, or epNEC who had failed at least one line of platinum-based chemotherapy. DLL3 positivity defined as >0% of tumor cells with moderate-to-strong staining (SP347, Roche Diagnostics). Median age 57 years, 64% male, 49% with prior PD-1/PD-L1 therapy.
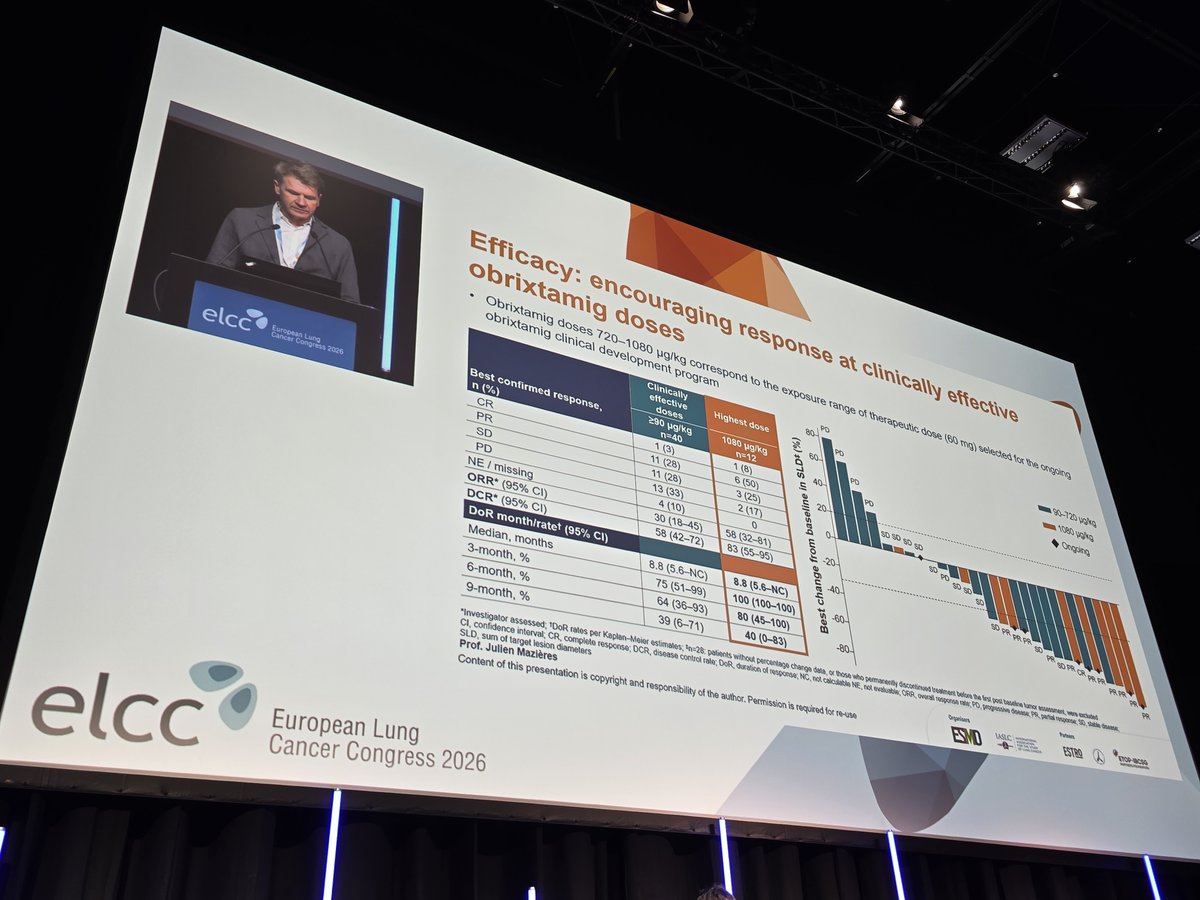
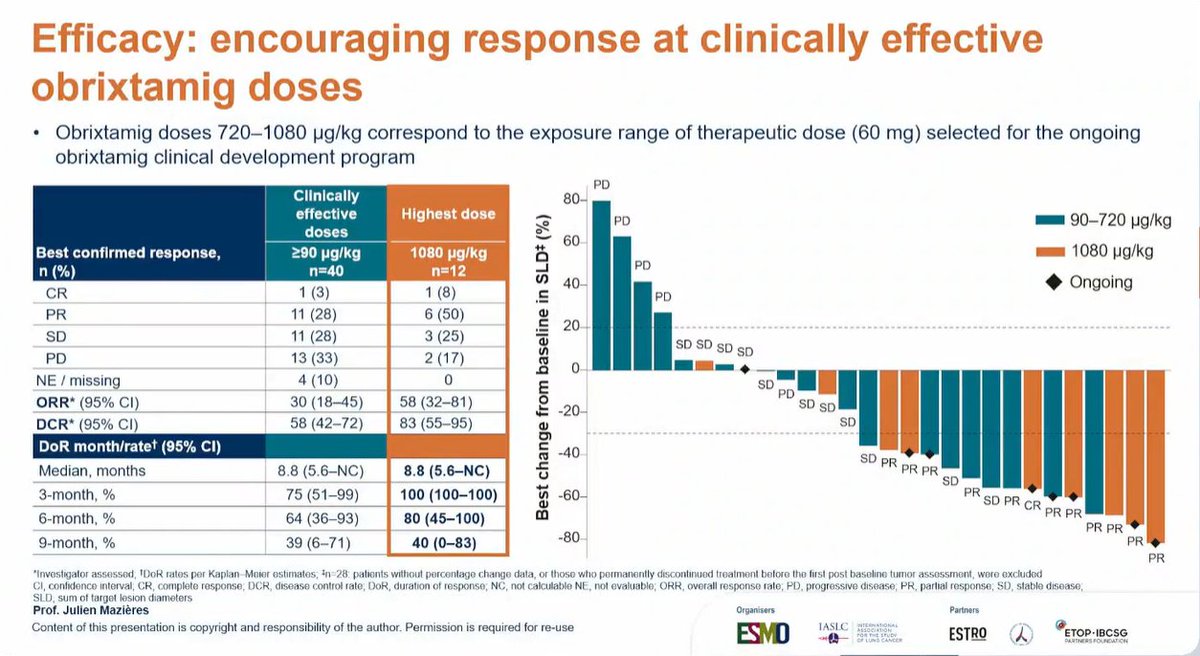
Obrixtamig (DLL3xCD3 T-cell engager) + ezabenlimab (anti-PD-1 humanized IgG4 mAb). Treatment continued until disease progression, undue toxicity, or consent withdrawal. Clinically effective doses identified as 720-1080 mcg/kg (corresponding to therapeutic dose of 60 mg).
Primary: Dose-limiting toxicities (DLTs) during the MTD evaluation period (Cycle 1 + 1 week at target dose). Secondary: Efficacy endpoints including ORR, DCR, DoR, and PFS by RECIST v1.1 (investigator assessed).
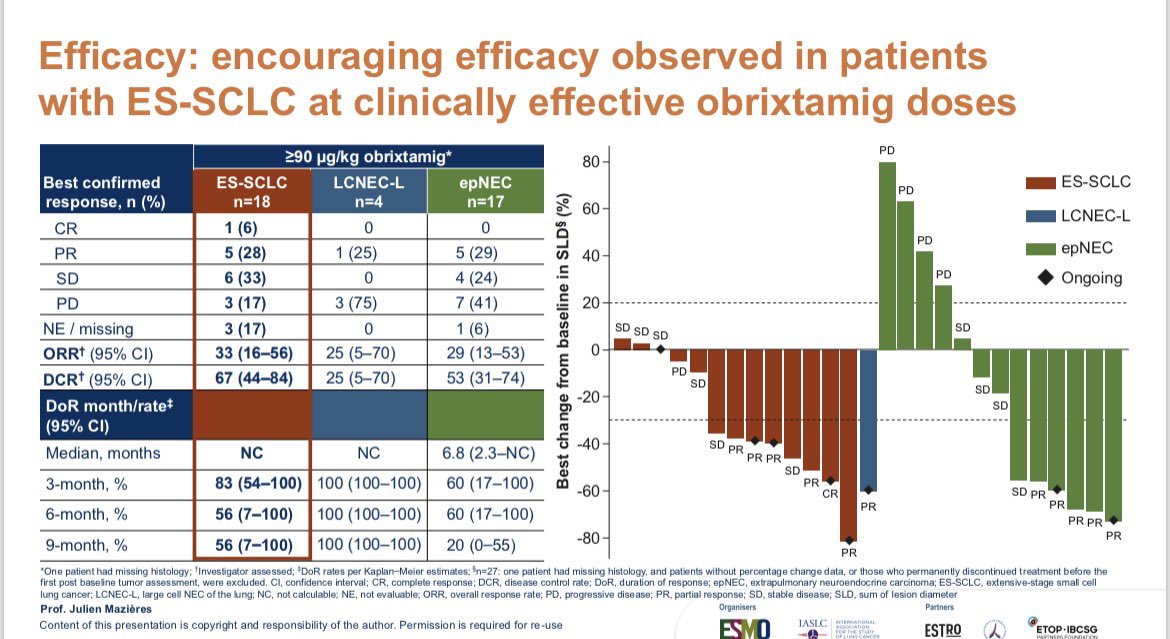
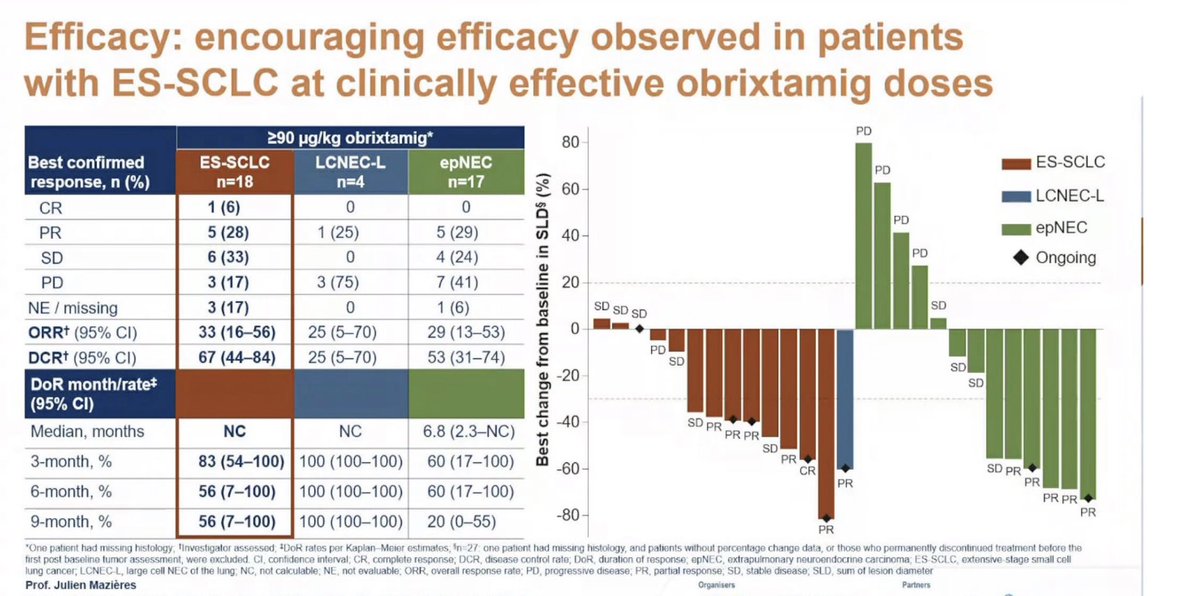
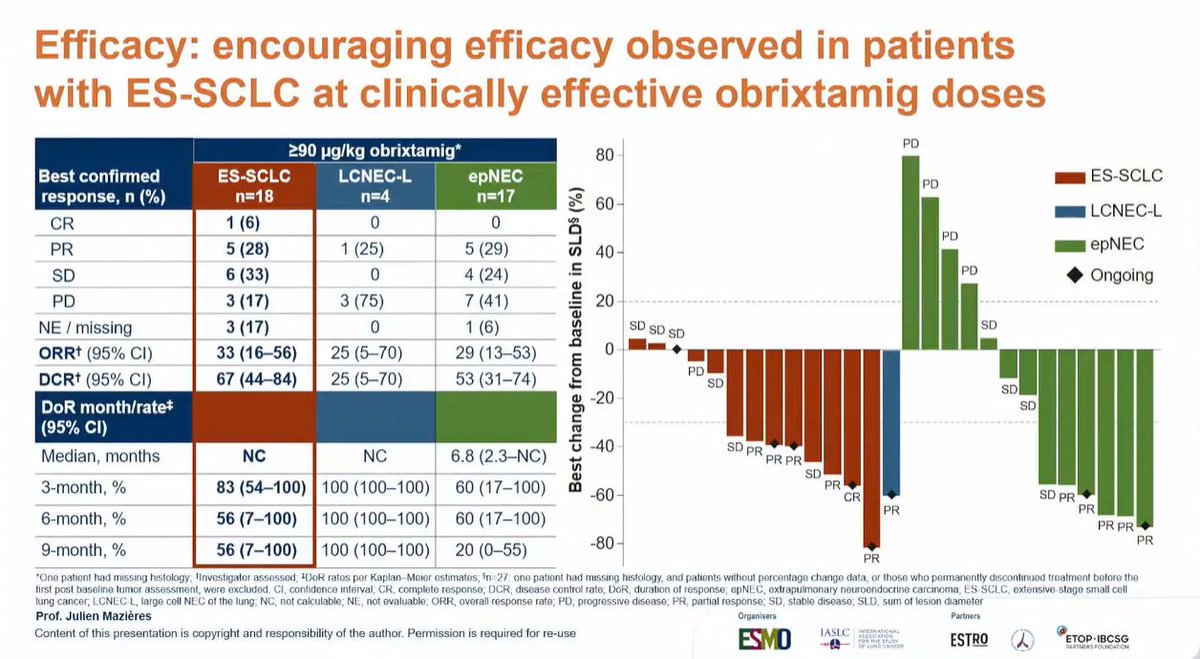
At clinically effective obrixtamig doses (>=90 mcg/kg, n=40), the overall response rate (ORR) was 30% (95% CI: 18-45) with a disease control rate (DCR) of 58% (95% CI: 42-72). At the highest dose (1080 mcg/kg, n=12), ORR improved to 58% (95% CI: 32-81) with DCR of 83% (95% CI: 55-95). Median duration of response was 8.8 months (95% CI: 5.6-NC) with a 6-month DoR rate of 64% at clinically effective doses.
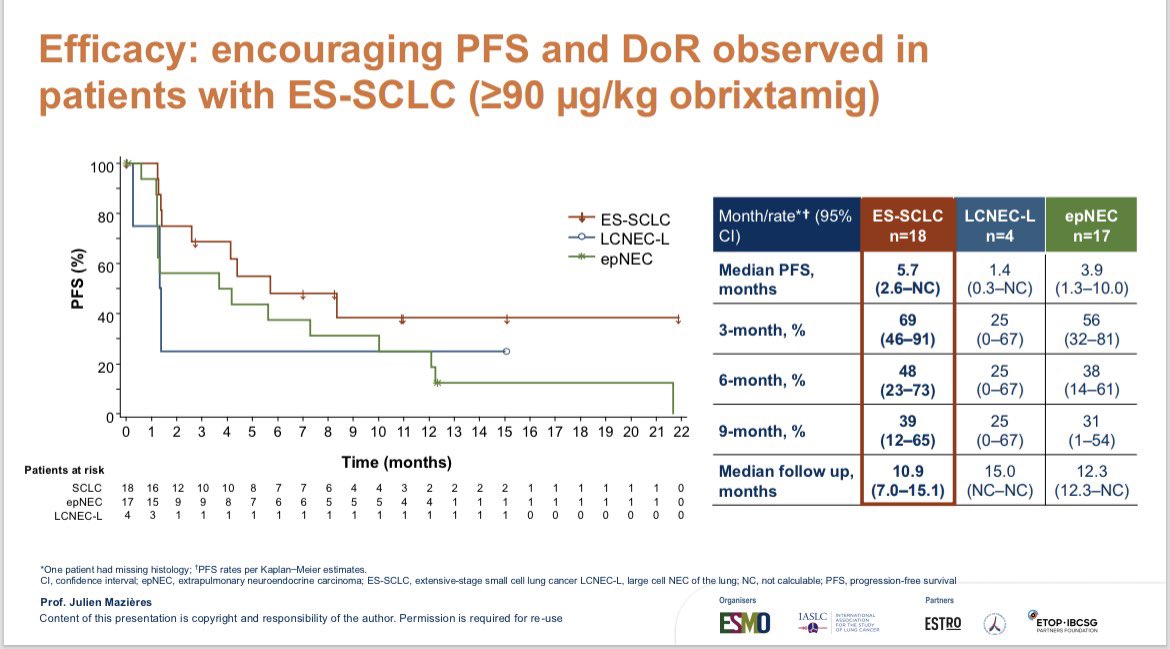
Overall median PFS was 4.4 months. By histology at clinically effective doses (>=90 mcg/kg): ES-SCLC (n=18) showed median PFS of 5.7 months (95% CI: 2.6-NC) with a 6-month PFS rate of 48% (23-73); epNEC (n=17) had median PFS of 3.9 months (95% CI: 1.3-10.0); LCNEC-L (n=4) had median PFS of 1.4 months (95% CI: 0.3-NC). At the highest dose, median PFS reached 10 months.
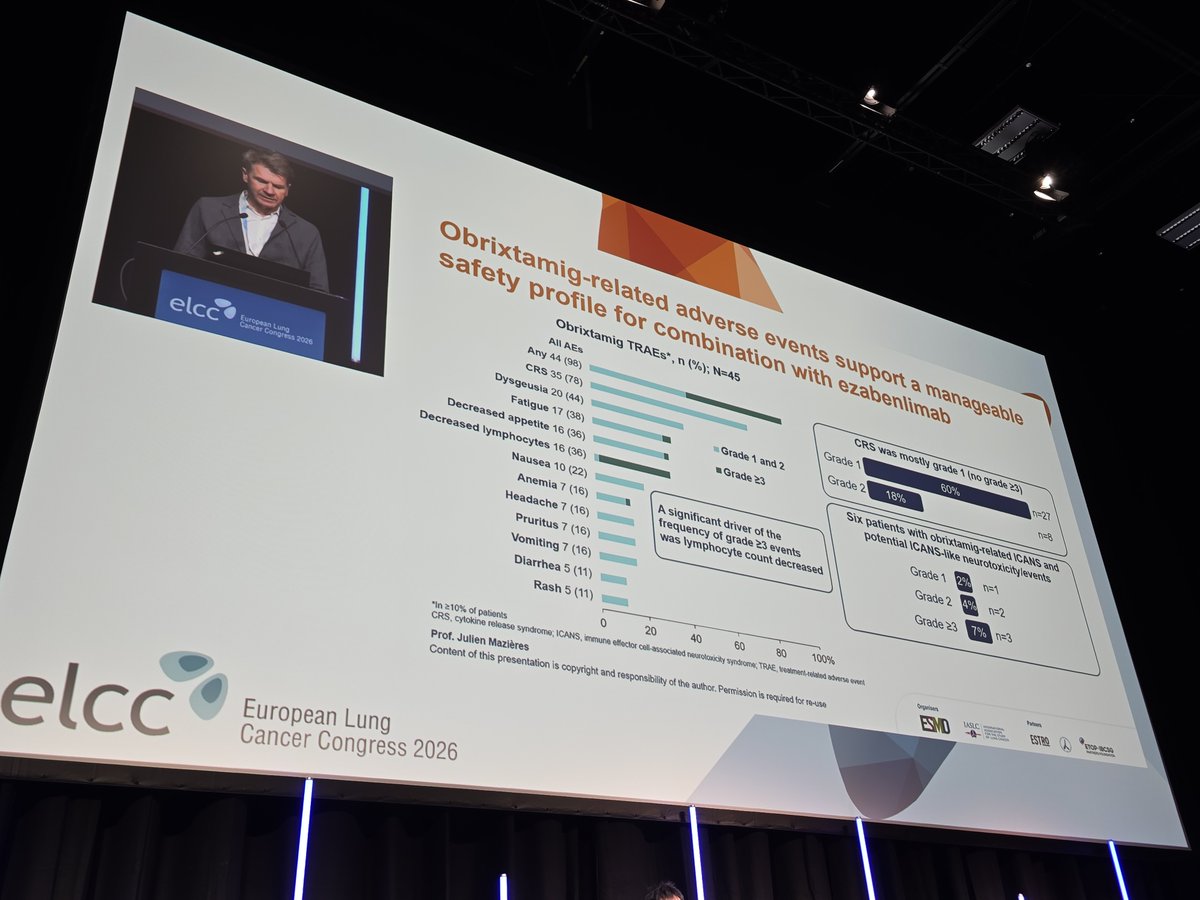
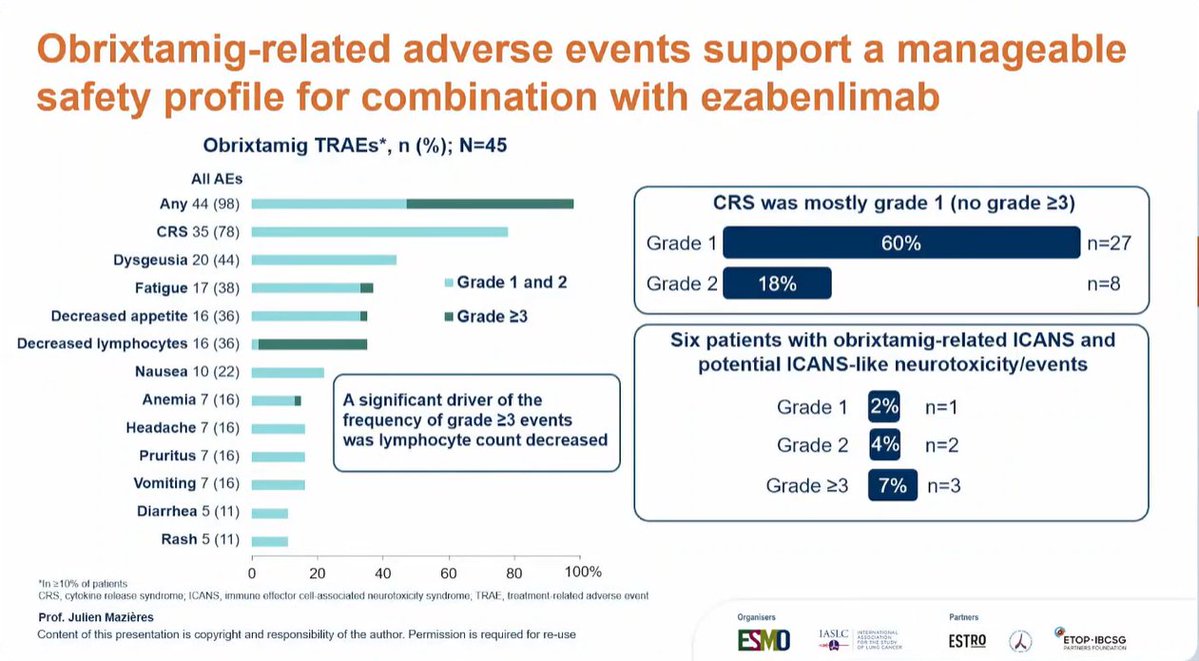
Treatment-related adverse events (TRAEs) occurred in 98% of patients (44/45). The most common TRAE was cytokine release syndrome (CRS) in 78% of patients, which was mostly grade 1 (60%, n=27) with no grade 3 or higher CRS events. Other common TRAEs included dysgeusia (44%), fatigue (38%), decreased appetite (36%), and decreased lymphocytes (36%). Six patients experienced ICANS or potential ICANS-like neurotoxicity events (grade 1: 2%, grade 2: 4%, grade >=3: 7%). Lymphocyte count decrease was identified as a significant driver of grade >=3 events.
The combination of obrixtamig and ezabenlimab demonstrates encouraging antitumor activity across DLL3-expressing neuroendocrine carcinomas, with particularly notable responses at the highest dose level. The manageable safety profile, characterized by predominantly low-grade CRS and limited ICANS events, supports continued clinical development. This trial represents one of the first evaluations of a DLL3-targeted T-cell engager combined with PD-1 blockade, and the dose-response relationship observed at 1080 mcg/kg (ORR 58%, mPFS 10 months) is especially encouraging for patients who have progressed on prior platinum-based chemotherapy and immunotherapy. Obrixtamig + ezabenlimab remains investigational and is not approved for any indication.