EGFR-mutant NSCLC after TKI failure -- Sichuan Kelun-Biotech (sacituzumab tirumotecan)
Discover KOL Sentiment on OptiTROP-Lung-03 →Design - Phase 2 sacituzumab tirumotecan (sac-TMT, TROP2 ADC) vs docetaxel, EGFR-mutant NSCLC after EGFR-TKI + platinum chemotherapy (NCT05631262); ELCC 2026 final OS.
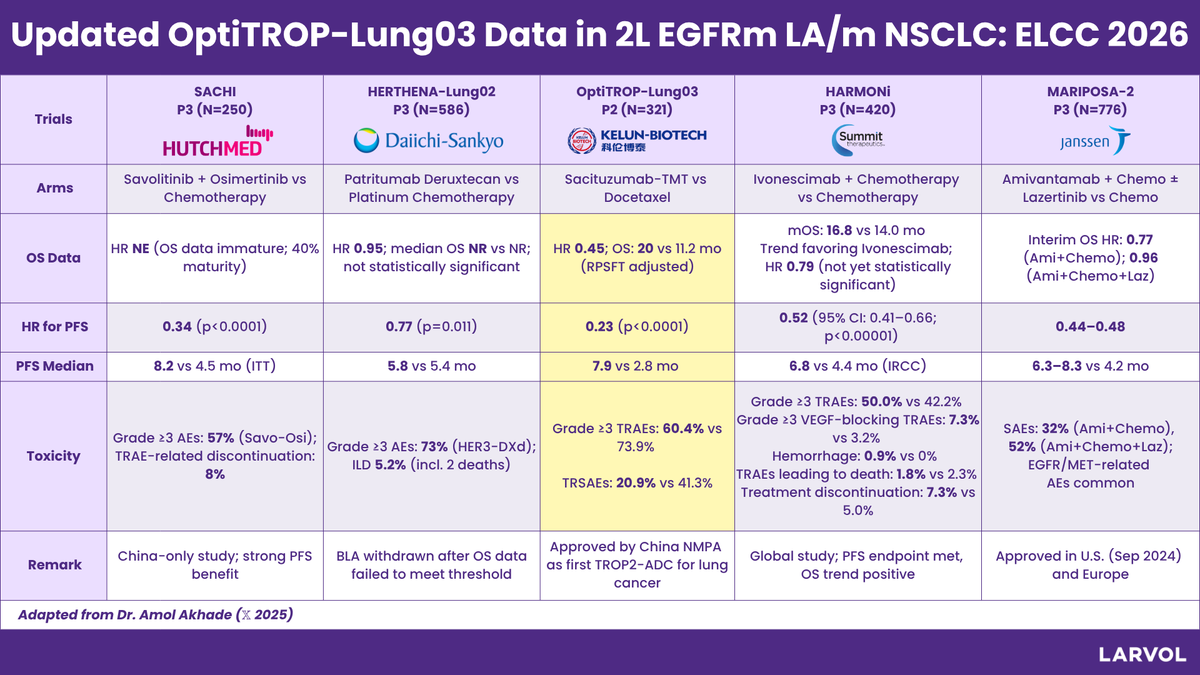
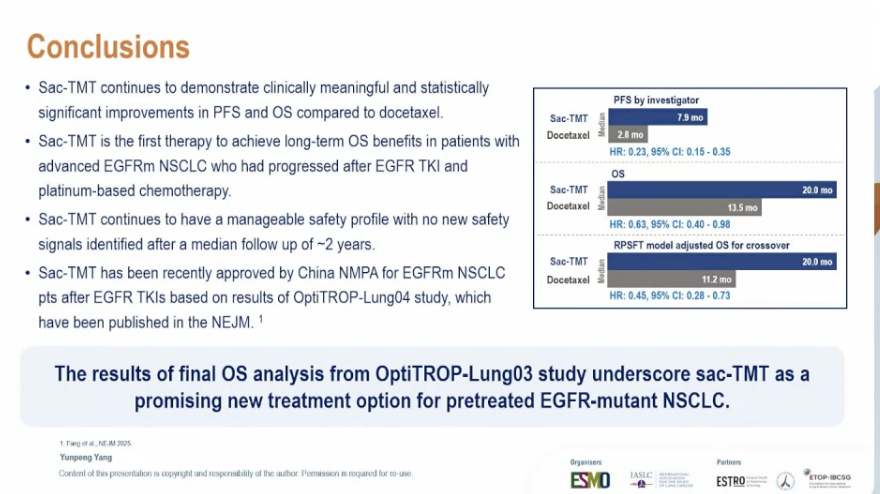
PFS - Median 7.9 vs 2.8 mo (investigator), HR 0.23 (95% CI 0.15-0.35) - significant.
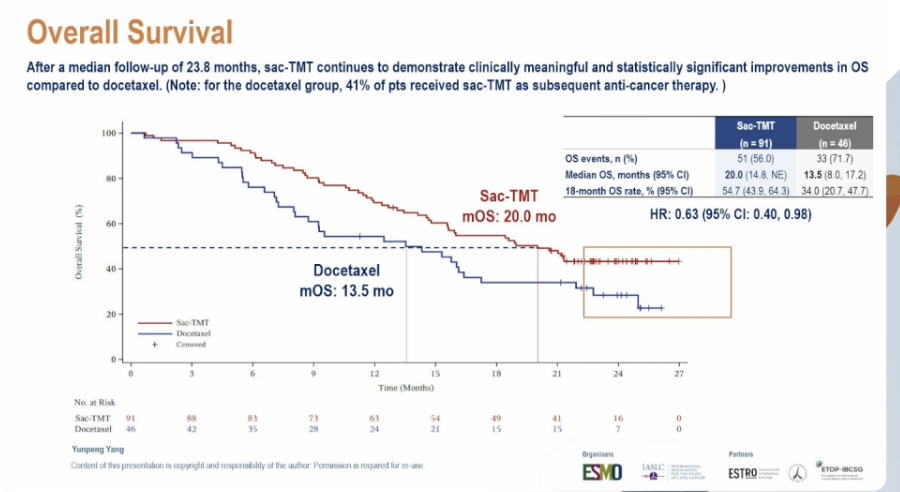
OS - Median 20.0 vs 13.5 mo, HR 0.63 (95% CI 0.40-0.98); 18-month OS 54.7% vs 34.0% - first therapy to show long-term OS benefit in this population.
Safety - Manageable, no new safety signals at ~2-year median follow-up; better safety profile than docetaxel at the earlier analysis.
Regulatory - Investigational in the US (NOT FDA approved); NMPA-approved in China for EGFR-mutant NSCLC after TKI + chemotherapy.
Sponsor / drug - Sichuan Kelun-Biotech (partner Merck); sacituzumab tirumotecan (sac-TMT / SKB264 / MK-2870).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.









Top 10 by impressions -- click to view on X
🚨 Day 3 #ELCC26 – Trials to Watch 🫁 Early-stage NSCLC – perioperative IO maturity 🔹 KEYNOTE-671 (222MO, 223MO) 5-year outcomes by pCR vs non-pCR 👉 Long-term validation of...
Updated OptiTROP-Lung03 data from ELCC 2026 in 2L EGFRm LA/m NSCLC landscape from Dr. Amol Akhade (@SuyogCancer)👉 Updated Landscape ⬇️: Explore more insights and conference data from...
Updated Overall Survival of Sacituzumab-Tirumotecan in pretreated EGFR mut+ NSCLC OptiTROP Lung03 presented at #ELCC2026 @OncoAlert
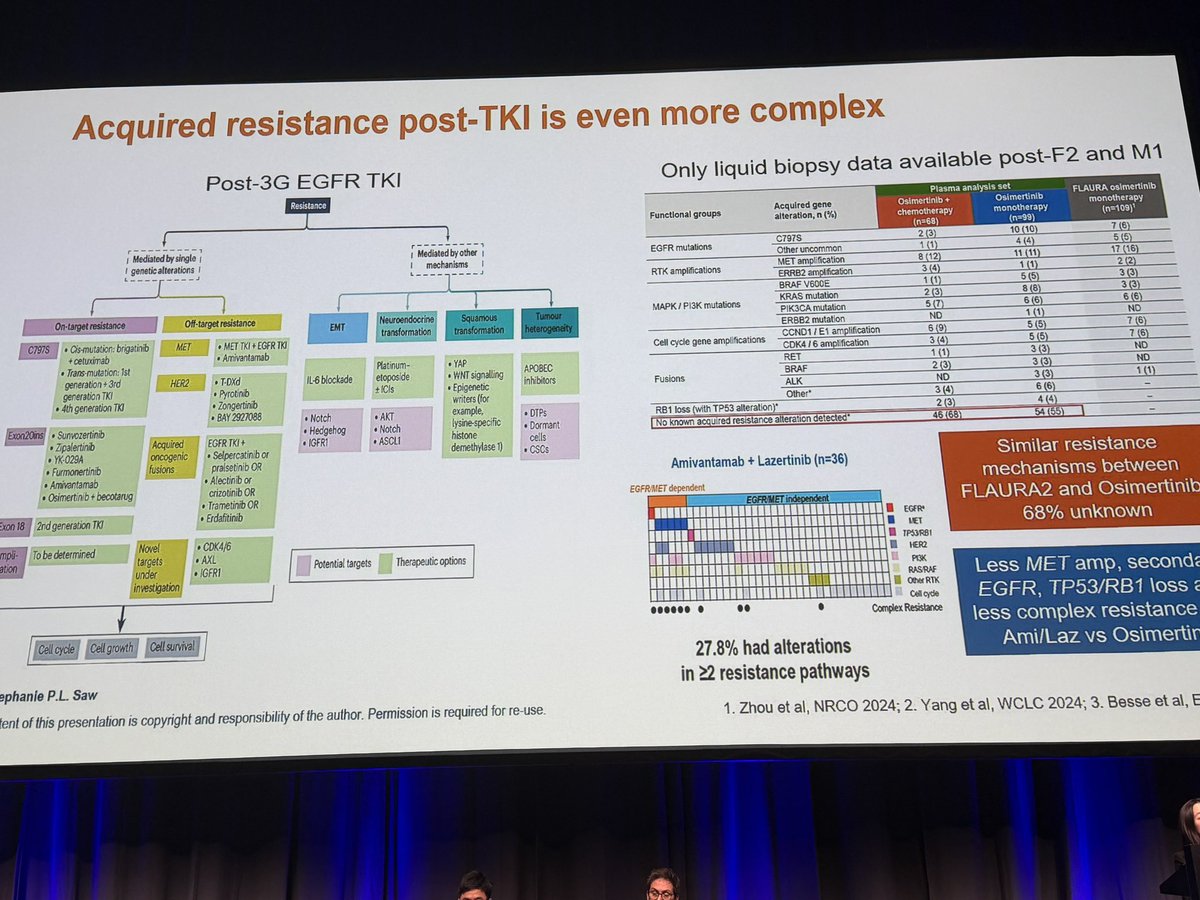
#ELCC26 A comprehensive presentation by @stephanieplsaw on selection of optimal treatment for #ΕGFRmut. #NSCLC based on defining...
🆙 #ELCC26 @myESMO 🇩🇰 🔥Mini Oral session 2 ☑️OptiTROP-Lung03 🎯mPFS 7.9 vs. 2.8m (HR 0.23, 95%CI 0.15-0.35) 🎯mOS 20.0 vs. 13.5 m (HR 0.63, 95%CI 0.40-0.98) 🎙️Dr. Yunpeng...
🚨 OptiTROP-Lung03 @ASCO Sac-TMT shows superior efficacy vs docetaxel in pretreated EGFRm NSCLC: ✅ ORR 45.1% vs 15.6% (p=0.0004) ✅ PFS: 6.9 vs 2.8 mo (HR 0.30) ✅ OS: HR 0.49 (adjusted HR...

Great EGFR-mutant NSCLC session. Impressed by the Sac-TMT results (anti-TROP2 ADC), which show the most positive outcomes across two Chinese studies. Other ADCs are also in the pipeline, things are...
🔥 #ELCC26 Sac-TMT strengthens the case in pretreated EGFR-mutant NSCLC Final OS analysis from OptiTROP-Lung03 shows sacituzumab tirumotecan outperforming docetaxel after EGFR TKI +...

#ASCO25 @ASCO #NSCLC #LCSM OptiTROP-Lung03 (Abstract 8507): Sacituzumab tirumotecan (sac-TMT) vs docetaxel in previously treated...

OPTI-Trop rand ph2 study of anti-Trop2 ADC, saci-terumotecan vs docetaxel in pts w EGFR+ NSCLC after progression on TKI W much better ORR/PFS w sac-TMT - lets just say that doce has been...
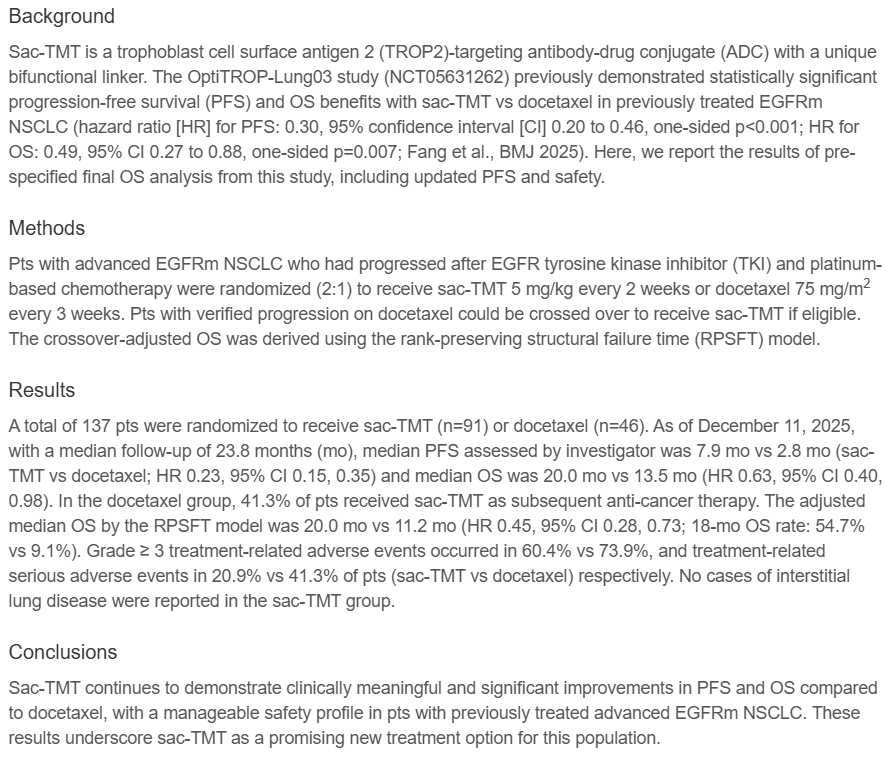
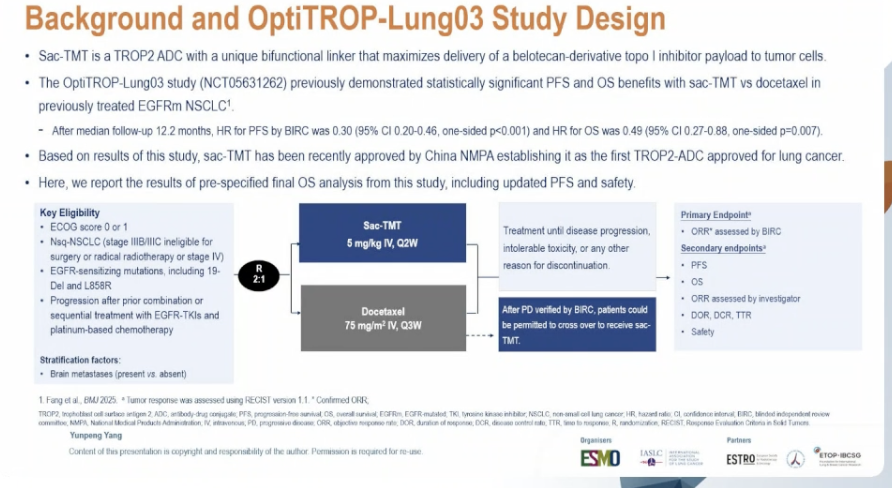
OptiTROP-Lung03 (NCT05631262) is a randomized phase 2 trial evaluating sacituzumab tirumotecan (sac-TMT), a TROP2-directed antibody-drug conjugate with a unique bifunctional linker delivering a belotecan-derivative topoisomerase I inhibitor payload. The study compares sac-TMT (5 mg/kg IV, Q2W) versus docetaxel (75 mg/m2 IV, Q3W) in patients with previously treated EGFR-mutant advanced NSCLC who progressed after EGFR TKI and platinum-based chemotherapy. Patients were randomized 2:1 with stratification by brain metastasis status. Crossover from docetaxel to sac-TMT was permitted after verified progressive disease.
Randomized, open-label, phase 2 study comparing sac-TMT vs docetaxel in a 2:1 ratio. Stratification by brain metastases (present vs absent). No companion diagnostic required.
Patients with non-squamous NSCLC (stage IIIB/IIIC ineligible for surgery or radical radiotherapy, or stage IV) harboring EGFR-sensitizing mutations (19del and L858R), who progressed after combination or sequential treatment with EGFR TKIs and platinum-based chemotherapy. ECOG PS 0-1.
Sac-TMT 5 mg/kg IV every 2 weeks versus docetaxel 75 mg/m2 IV every 3 weeks. Treatment continued until disease progression, intolerable toxicity, or other discontinuation criteria. Crossover to sac-TMT was permitted after BIRC-verified progressive disease on docetaxel.
Primary endpoint: confirmed objective response rate (ORR) assessed by BIRC per RECIST v1.1. Secondary endpoints: PFS, OS, investigator-assessed ORR, duration of response (DOR), disease control rate (DCR), time to response (TTR), and safety.
At the pre-specified final OS analysis (median follow-up 23.8 months), sac-TMT demonstrated a significant PFS benefit. Median PFS by investigator was 7.9 months with sac-TMT versus 2.8 months with docetaxel (HR 0.23, 95% CI 0.15-0.35). The BIRC-assessed PFS at the earlier analysis showed HR 0.30 (95% CI 0.20-0.46, one-sided p<0.001).
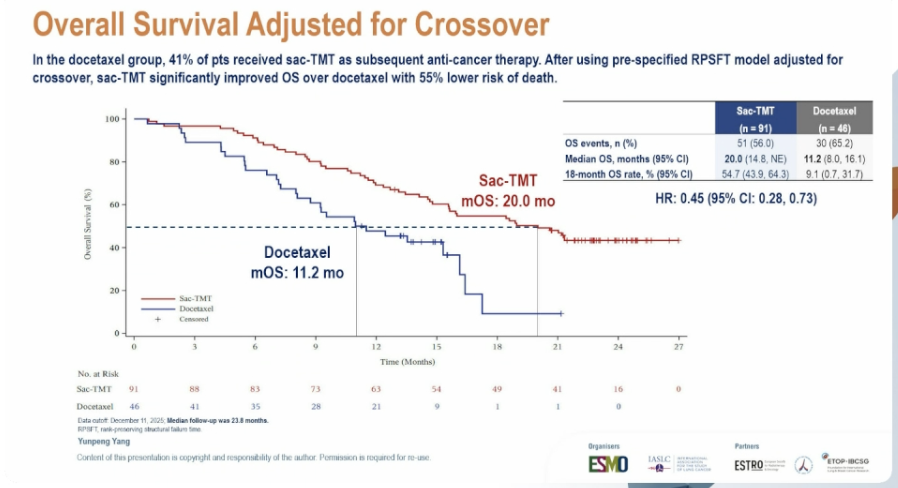
After a median follow-up of 23.8 months, sac-TMT demonstrated a statistically significant improvement in OS: median OS 20.0 months (95% CI 14.8, NE) vs 13.5 months (95% CI 8.0, 17.2) with docetaxel (HR 0.63, 95% CI 0.40-0.98). The 18-month OS rate was 54.7% vs 34.0%. After adjusting for crossover (41% of docetaxel patients received sac-TMT) using the pre-specified RPSFT model, HR was 0.45 (95% CI 0.28-0.73) with median OS 20.0 vs 11.2 months.
Sac-TMT continues to have a manageable safety profile with no new safety signals identified after a median follow-up of approximately 2 years. The safety profile was consistent with earlier reports. At the earlier ASCO analysis, sac-TMT demonstrated a better safety profile compared to docetaxel.
Sac-TMT is the first therapy to achieve long-term OS benefits in patients with advanced EGFR-mutant NSCLC who progressed after EGFR TKI and platinum-based chemotherapy. The final OS analysis underscores sac-TMT as a promising new treatment option for this population. Sac-TMT has been approved by China NMPA for EGFR-mutant NSCLC based on the related OptiTROP-Lung04 study (published in NEJM), establishing it as the first TROP2-ADC approved for lung cancer. Sac-TMT remains investigational outside China and is not FDA-approved.
OptiTROP-Lung-03 is a registrational Phase 2 randomized trial (NCT05631262) comparing sacituzumab tirumotecan (sac-TMT, also called SKB264 or MK-2870, a TROP2-directed antibody-drug conjugate) with docetaxel in patients with locally advanced or metastatic EGFR-mutant non-small cell lung cancer who progressed after an EGFR-TKI and platinum-based chemotherapy. It was run by Sichuan Kelun-Biotech.
Sac-TMT significantly outperformed docetaxel. Median progression-free survival was 7.9 versus 2.8 months (HR 0.23; 95% CI 0.15-0.35), and at the final analysis median overall survival was 20.0 versus 13.5 months (HR 0.63; 95% CI 0.40-0.98), with an 18-month overall survival rate of 54.7% versus 34.0%. Sac-TMT is the first therapy to achieve a long-term overall-survival benefit in this previously treated EGFR-mutant NSCLC population.
No. Sacituzumab tirumotecan (sac-TMT) is investigational in the United States and is not FDA approved. Based on OptiTROP-Lung-03, it was approved by China's National Medical Products Administration (NMPA) for previously treated EGFR-mutant NSCLC, and a Merck-partnered global development program is ongoing under the name sacituzumab tirumotecan.
Sac-TMT (SKB264/MK-2870) is a TROP2-directed antibody-drug conjugate carrying a topoisomerase-I payload. It belongs to the same broad class as other TROP2 ADCs such as datopotamab deruxtecan and sacituzumab govitecan, but is a distinct molecule with its own linker-payload and clinical program.
Sac-TMT had a manageable safety profile with no new safety signals after approximately 2 years of median follow-up, consistent with earlier reports. At the earlier analysis, sac-TMT demonstrated a better safety profile than docetaxel in this previously treated population.