Phase 3 trial of amivantamab (Rybrevant) plus carboplatin-pemetrexed vs chemotherapy alone as first-line treatment for EGFR exon 20 insertion advanced NSCLC. Presented at ESMO 2023, published in NEJM; basis for the March 2024 FDA full approval.
FDA Approved · Mar 2024EGFR Exon20ins NSCLC1st-LinePhase 3Amivantamab + Chemo · Johnson & Johnson
National Comprehensive
NCCN
Cancer Network®
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®)
Non-Small Cell Lung
Cancer
Version 1.2024 - December 21, 2023
NCCN.org
NCCN Guidelines for Patients® available at www.nccn.org/patients
Continue
Treatment with
RYBREVANT®
(amivantamab-vmjw)
Plus Chemotherapy
Resulted in
Statistically Significant
and Clinically
Meaningful
Improvement in
Progression-Free
Survival in Patients
with Newly Diagnosed
EGFR Exon 20
Insertion Mutation-
Positive Non-Small
Cell Lung Cancer
PRARMACENTICAL COMPANIES OF
janssen
Johnson-Johnson
[Slide 1]
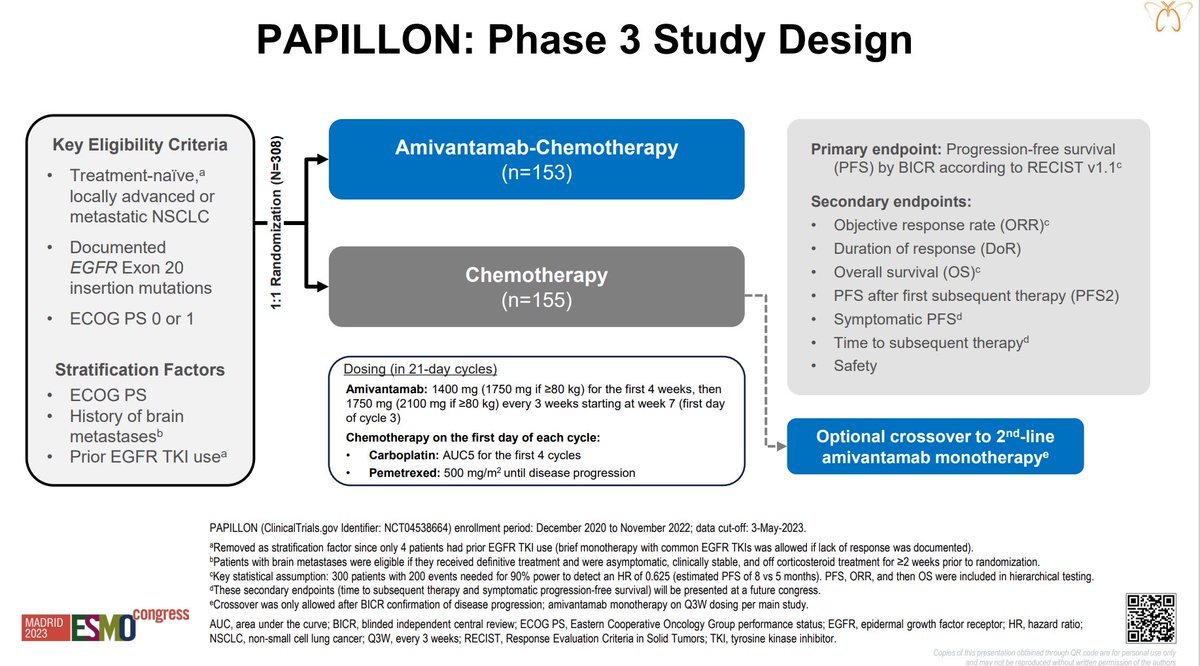
PAPILLON: Phase 3 Study Design
Key Eligibility Criteria
Amivantamab-Chemotherapy
Primary endpoint: Progression-free survival
Treatment-naîve a
(n=153)
(PFS) by BICR according to RECIST v1.1°
locally advanced or
Secondary endpoints:
metastatic NSCLC
Objective response rate (ORR)c
Documented
Duration of response (DoR)
EGFR Exon 20
Chemotherapy
Overall survival (OS)c
insertion mutations
(n=155)
PFS after first subsequent therapy (PFS2)
ECOG PS 0 or 1
Symptomatic PFS
Time to subsequent therapyd
Stratification Factors
Dosing (in 21-day cycles)
Safety
ECOG PS
Amivantamab: 1400 mg (1750 mg if >80 kg) for the first 4 weeks, then
1750 mg (2100 mg if >80 kg) every 3 weeks starting at week 7 (first day
History of brain
of cycle 3)
metastases
Chemotherapy on the first day of each cycle:
Optional crossover to 2nd-line
Prior EGFR TKI use
Carboplatin: AUC5 for the first 4 cycles
amivantamab monotherapy®
Pemetrexed: 500 mg/m2 until disease progression
PAPILLON (ClinicalTrials.gov Identifier: NCT04538664) enrollment period: December 2020 to November 2022; data cut-off: 3-May-2023.
Removed as stratification factor since only 4 patients had prior EGFR TKI use (brief monotherapy with common EGFR TKIs was allowed if lack of response was documented).
Patients with brain metastases were eligible if they received definitive treatment and were asymptomatic, clinically stable, and off corticosteroid treatment for >2 weeks prior to randomization.
Key statistical assumption: 300 patients with 200 events needed for 90% power to detect an HR of 0.625 (estimated PFS of 8 vs 5 months). PFS, ORR, and then os were included in hierarchical testing.
These secondary endpoints (time to subsequent therapy and symptomatic progression-free survival) will be presented at a future congress.
*Crossover was only allowed after BICR confirmation of disease progression; amivantamab monotherapy on Q3W dosing per main study.
MADRID
congress
ESMO
AUC. area under the curve; BICR, blinded independent central review: ECOG PS, Eastern Cooperative Oncology Group performance status; EGFR, epidermal growth factor receptor; HR, hazard ratio;
2023
NSCLC, non-small cell lung cancer; Q3W, every 3 weeks; RECIST, Response Evaluation Criteria in Solid Tumors; TKI, tyrosine kinase inhibitor.
Copies of this presentation obtained through OR
---
[Slide 2]
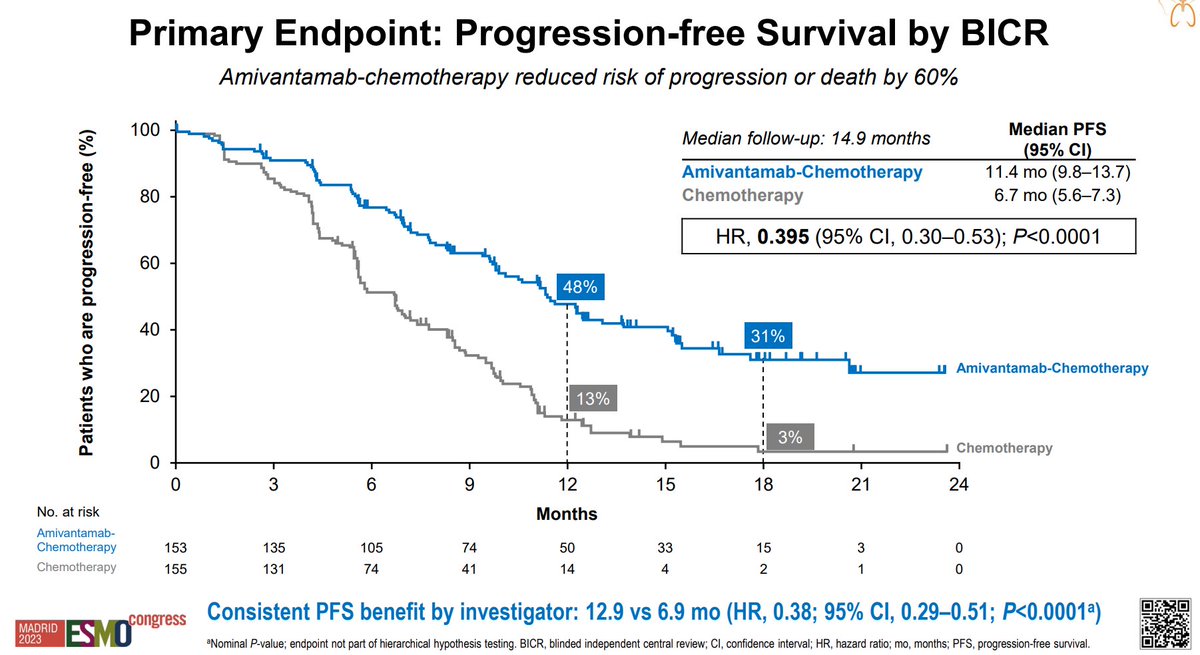
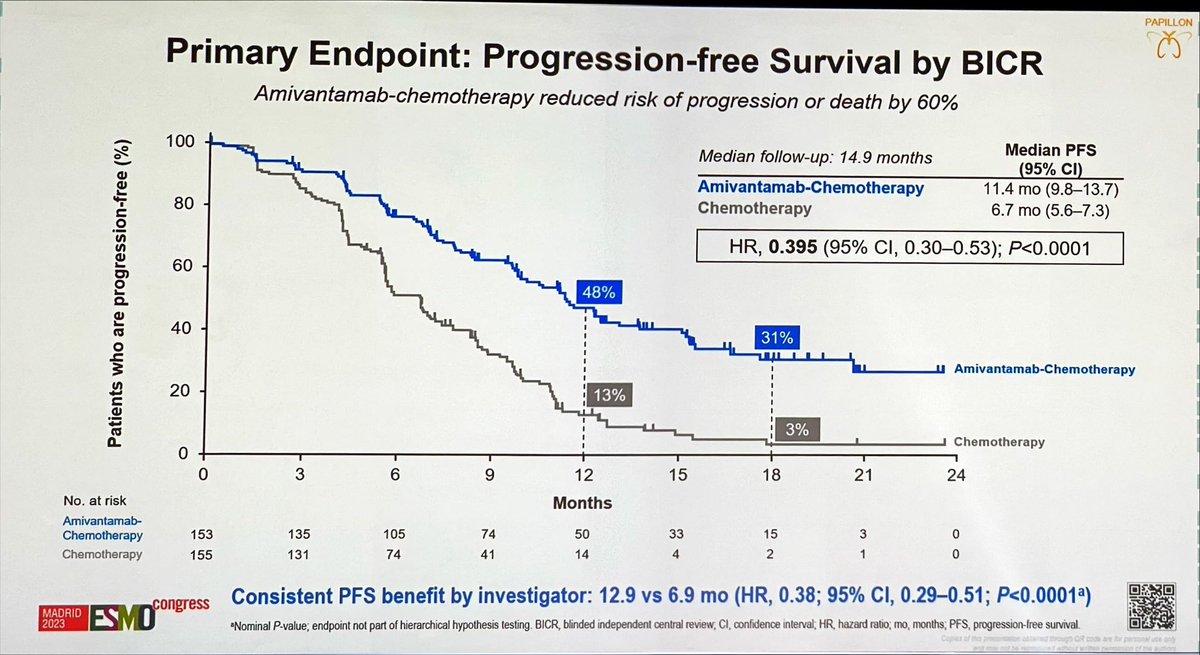
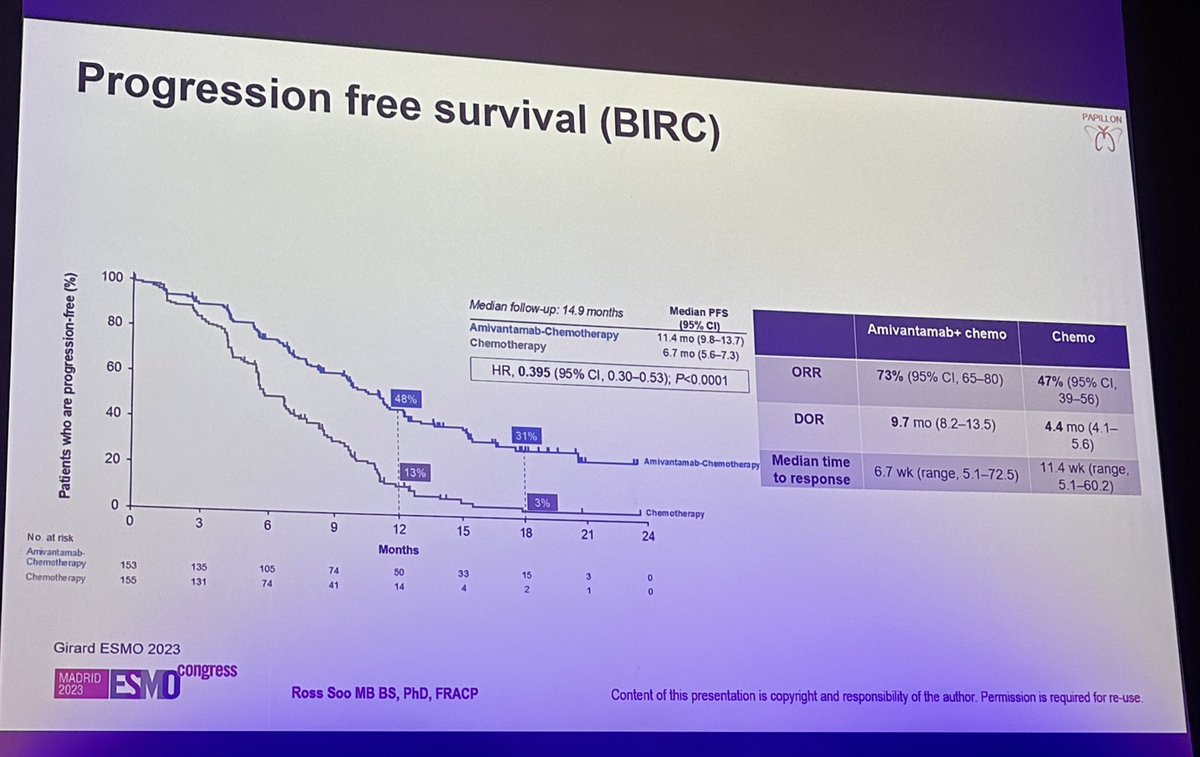
Primary Endpoint: Progression-free Survival by BICR
Amivantamab-chemotherapy reduced risk of progression or death by 60%
Median PFS
100
Median follow-up: 14.9 months
(95% CI)
Amivantamab-Chemotherapy
11.4 mo (9.8-13.7)
Chemotherapy
6.7 mo (5.6-7.3)
80
HR, 0.395 (95% CI, 0.30-0.53); P<0.0001
60
48%
LL
ALL
40
31%
LL
T
Amivantamab-Chemotherapy
20
13%
3%
Chemotherapy
0
9
12
15
18
21
24
0
3
6
Months
No. at risk
Amivantamab-
Chemotherapy
153
135
105
74
50
33
15
3
0
155
131
74
41
14
4
2
1
0
Chemotherapy
Consistent PFS benefit by investigator: 12.9 vs 6.9 mo (HR, 0.38; 95% CI, 0.29-0.51; P<0.0001a)
congress
MADRID
2023
ESMO
Nominal P-value: endpoint not part of hierarchical hypothesis testing. BICR. blinded independent central review; CI. confidence interval; HR, hazard ratio; mo, months: PFS, progression-free survival.
MADRID
ESMO
congress
2023
-
Amivantamab Plus Chemotherapy vs
Chemotherapy as First-line Treatment in
EGFR Exon 20 Insertion-mutated Advanced
Non-small Cell Lung Cancer (NSCLC)
Primary Results From PAPILLON, a Randomized
Phase 3 Global Study
Nicolas Girard Keunchil Park,2.* Ke-Jing Tang,3 Byoung Chul Cho,*
Luis Paz-Ares, Susanna Cheng, Satoru Kitazono, Muthukkumaran Thiagarajan,*
Jonathan W. Goldman, Joshua K. Sabari, 10 Rachel E. Sanborn, 11 Aaron S. Mansfield,12
Jen-Yu Hung,13 Sanjay Popat, 14 Josiane Mourão, 15 Archan Bhattacharya, 16
Trishala Agrawal,1 S. Martin Shreeve, Roland E. Knoblauch, Caicun Zhou
-
I
-
-
Theres
Versites,
France
Send
/
First
Unive
Division
Dolutes
Medical
I
-
New
-
Cellomia,
OR,
MN
Claic,
-
High
UK
PA,
USA
CA
School
===
Milation
MO
MADRID
MADRID
ESMocongress
---
PAPILLON
Primary Endpoint: Progression-free Survival by BICR
Amivantamab-chemotherapy reduced risk of progression or death by 60%
100
Median PFS
Median follow-up: 14.9 months
(95% CI)
Amivantamab-Chemotherapy
11.4 mo (9.8-13.7)
Patients who are progression-free (%)
80
Chemotherapy
6.7 mo (5.6-7.3)
HR, 0.395 (95% CI, 0.30-0.53); P<0.0001
60
48%
40
31%
u Amivantamab-Chemotherapy
20
13%
3%
Chemotherapy
0
0
3
6
9
12
15
18
21
24
No. at risk
Months
Amivantamab-
Chemotherapy
153
135
105
74
50
33
15
3
0
Chemotherapy
155
131
74
41
14
4
2
1
0
MADRID
congress
Consistent PFS benefit by investigator: 12.9 vs 6.9 mo (HR, 0.38; 95% CI, 0.29-0.51; P<0.0001ᵃ)
2023
ESMD
*Nominal P-value; endpoint not part of hierarchical hypothesis testing. BICR, blinded independent central review, CI, confidence interval; HR, hazard ratio, mo, months; PFS, progression-free survival
I I
MADRID
2023
ESMD
congress
congress
SMO
---
PAPILLON
MADRID
congress
2023
ESMO
Amivantamab Plus Chemotherapy vs
Chemotherapy as First-line Treatment in
EGFR Exon 20 Insertion-mutated Advanced
Non-small Cell Lung Cancer (NSCLC)
Primary Results From PAPILLON, a Randomized
Phase 3 Global Study
⑉
⑉
Nicolas Girard,1 Keunchil Park,2.* Ke-Jing Tang,³ Byoung Chul Cho,4
Luis Paz-Ares,⁵ Susanna Cheng,6 Satoru Kitazono,⁷ Muthukkumaran Thiagarajan,⁸
Jonathan W. Goldman,9 Joshua K. Sabari,¹ 10 Rachel E. Sanborn,11 Aaron S. Mansfield,12
Jen-Yu Hung,¹³ Sanjay Popat,14 Josiane Mourão, 15 Archan Bhattacharya,16
Trishala Agrawal,17 S. Martin Shreeve,¹⁸ Roland E. Knoblauch,17 Caicun Zhou19
Institut Curie, Institut du Thorax Curie-Montsouris Paris, France and Paris Saclay University UVSQ Versailles France Samsung Medical Center
Sungkyunkwan University School of Medicine Seoul Republic of Korea The First Affiliated Hospital of Sun Yat-sen University Guangzhou China "Division
of Medical Oncology Yonsei Cancer Center. Yonsei University College of Medicine Seoul Republic of Korea Hospital Universitario 12 de Octubre Madrid
Spain, *Sunnybrook Odette Cancer Centre. Toronto. ON. Canada Cancer Institute Hospital Japanese Foundation for Cancer Research Tokyo. Japan
General Hospital Kuala Lumpur, Kuala Lumpur, Malaysia David Geffen School of Medicine University of California Los Angeles, Los Angeles, California
USA *NYU Langone Health New York NY. USA "Earle A Chiles Research Institute Providence Cancer Institute Portland OR USA Mayo Clinic
Rochester MN, USA; Department of Internal Medicine Kaohsking Medical University Hospital Kaohsiung Medical University Kaohslung Talwan "Royal
Marsden Hospital NHS Foundation Trust London UK and The Institute of Cancer Research London UK; "Barretos Cancer Hospital Barretos Brazil
"Janssen R&D. High Wycombe UK: Janssen R&D Spring House, PA USA: "Janssen R&D San Diego, CA USA; "Shanghai Pulmonary Hospital Tong
⑉
University School of Medicine, Shanghai, China
"Current Affiliation MD Anderson Cancer Center Houston, TX, USA
Copies or the resentation cotained through OR code
or personal - and may not be restruced
without the
---
PAPILLON
EGFR Exon 20 Insertion Mutations (Ex20ins) Advanced NSCLC
Outcomes in newly diagnosed EGFR Ex20ins advanced NSCLC are historically poor¹-³
Reported median OS has ranged from 16 to 24 months, with a 5-year OS rate of 8%¹
Ex20ins are largely insensitive to common EGFR TKIs due to steric hindrance at the TKI-binding site⁴,⁵
Checkpoint inhibitors have failed to show benefit in this setting⁶⁷⁷
Platinum-based chemotherapy is the standard of care, but has limited efficacy
Amivantamab received first approval for EGFR Ex20ins advanced NSCLC after progression on platinum-based
chemotherapy
80
Best Response on Amivantamab in Post-platinum EGFR Ex20ins NSCLC8
n=81ᵃ; ORR=40%; DoR=11.1 months
60
Helical region (762-766)
Near loop region (767-772)
Far loop region (773-775)
Not detected by ctDNA
40
Best change from baseline in
SoD of target lesions (%)
20
0
-20
-40
-60
-80
-100
*One patient discontinued before any disease assessment and is not shown on the waterfall plot.
ctDNA circulating-tumor DNA DoR, duration of response; EGFR epidermal growth factor receptor, NSCLC, non-small cell lung cancer, ORR, objective response rate (by blinded independent central review);
OS, overall survival; SoD, sum of diameters; TKI, tyrosine kinase inhibitor
MADRID
congress
1. Bazhenova L, et al. Lung Cancer 2021;162:154-161 2. Ou S-H, et al. JTO Clin Res. 2023;4(10): 100558 3. Chouaid C, et al. Target Oncol 2021;16(6):801-811. 4. Vyse S, et al. Signal Transduct Target
Ther. 2019;4:5 5. Robichaux JP, et al. Nat Med. 2018,24(5):638-646. 6. Hou J. et al. Biomark Res. 2022;10(1):21. 7. Girard N, et al. Clin Lung Cancer. 2022,23(h):571-577. 8. Park K, et al. J Clin Oncol.
2023
2021;39(30):3391-3402
Copies
peserition
through
code
:
for
on
without
the
---
PAPILLON
Rationale for Combining Amivantamab and Chemotherapy
Amivantamab is an EGFR and MET
Trogocytosis and Antibody-dependent Cellular Cytotoxicity²
bispecific antibody with immune
Amivantamab-labeled
cell-directing activity1-3
NSCLC tumor cell
Macrophage
Combining amivantamab's ability to
Macrophage
engage immune cells with
Y
chemotherapy-mediated cell death
Tumor Cell
could lead to deeper and more durable
responses
Natural
Killer Cell
Phase 1 data (n=20) demonstrated
Video available in Mol Cancer Ther 2020.
safety, tolerability, and antitumor
activity of amivantamab-
Chemotherapy-mediated Cell Death5,6
chemotherapy⁴
Carboplatin
Pemetrexed
COM
Among 5 patients with treatment-
CO2H
naïve, EGFR Ex20ins NSCLC,
Tumor Cell
Tumor Cell Death
4 achieved a best response of PR
EGFR, epidermal growth factor receptor, Ex20ins, Exon 20 insertion mutations; NSCLC, non-small cell lung cancer, PR, partial response.
MADRID
congress
2023
ESMO
1. Moores S, et al. Cancer Res. 2016,76(13):3942-3953.2. Vijayaraghavan S, et al. Mol Cancer Ther 2020;19(10):2044-2056. 3. Yun J. et al. Cancer Discov. 2020;10(8):1194-1209.
4. Nagasaka M. et al. Poster presented at WCLC; September 8-14, 2021; Virtual 5 Schaer et al. Clin Cancer Res 2019,25(23):7175-7188 6. Schoch S. et al. Int J Mol Sci 2020;21(18) 6928
Capies the obtained through OR CODE are to
and may not be reproduced amount entim permission of the authors
Resources for Information | Approved Drugs
FDA approves amivantamab-
vmjw for EGFR exon 20
insertion-mutated non-small
cell lung cancer indications
f
Share
X Post
Email
On March 1, 2024, the Food and Drug
Administration approved amivantamab-
vmjw (Rybrevant, Janssen Biotech, Inc.)
with carboplatin and pemetrexed for the
first-line treatment of locally advanced
or metastatic non-small cell lung cancer
(NSCLC) with epidermal growth factor
receptor (EGFR) exon 20 insertion
mutations, as detected by an FDA-
approved test.
---
METHODS
The NEW ENGLAND JOURNAL of MEDICINE
RESEARCH SUMMARY
Amivantamab plus Chemotherapy in NSCLC
with EGFR Exon 20 Insertions
Zhou C et al. DOI: 10.1056/NEJMoa2306441
CLINICAL PROBLEM
In patients with non-small-cell lung cancer (NSCLC)
with exon 20 insertions in the gene encoding epidermal
growth factor receptor (EGFR), amivantamab — an EGFR
mesenchymal-epithelial transition factor (MET) bispecific
antibody with immune cell-directing activity — is ap-
proved for use after progression occurs during or after
Amivantamab
EGFR
receipt of first-line platinum-based chemotherapy. A pivotal
phase 1 trial also showed safety and antitumor activity of
amivantamab plus carboplatin-pemetrexed chemotherapy
Chemotherapy
(amivantamab-chemotherapy). More data on this combi-
Exon 20 insertions
c-MET
nation therapy are needed.
CLINICAL TRIAL
Progression-free Survival
Design: A phase 3, international, randomized trial
100
HR for disease progression or death, 0.40
(95% CI,0.30-0.53): P<0.001
assessed the efficacy and safety of amivantamab-
90
chemotherapy as compared with chemotherapy alone
80
as first-line therapy in patients with advanced NSCLC
with EGFR exon 20 insertions.
Percentage of Patients
70
60
Amivantamab + chemotherapy
50
11.4 mo (95% CI, 9.8-13.7)
Intervention: 308 adults were assigned to receive intrave-
40
Chemotherapy
nous amivantamab (1400 mg weekly for the first 4 weeks;
6.7 mo
30
(95% CI, 5.6-7.3)
1750 mg every 3 weeks starting at week 7 until progres-
20
sion occurred) plus carboplatin-pemetrexed chemotherapy
10
or chemotherapy alone, in 21-day cycles. Patients assigned
0
to chemotherapy alone could receive amivantamab mono-
0
3
6
9
12
15
18
21
24
Months since Randomization
therapy after disease progression was documented. The
primary outcome was progression-free survival.
Most Common Adverse Events in Each Group
100
RESULTS
Amivantamab . Chemotherapy
Chemotherapy
Efficacy: Progression-free survival was significantly
80
longer in the amivantamab-chemotherapy group than
in the chemotherapy group.
Safety: No new safety signal emerged for any agent.
Percentage of Patients
59
60
56
54
55
45
42
40
Discontinuation of amivantamab because of adverse
reactions was reported in 7% of patients.
20
0
LIMITATIONS AND REMAINING QUESTIONS
Neutropenia
Paronychia
Rash
Anemia
Neutropenia
Nausea
Blinding of treatment assignments was not possible
because of differences in drug administration, pre-
medication requirements, and safety profiles.
CONCLUSIONS
The number of deaths in the trial was too few to provide
In patients with previously untreated, advanced NSCLC
robust conclusions regarding overall survival; an analysis
with EGFR exon 20 insertions, progression-free survival
is planned at approximately 4 years of follow-up.
was significantly longer with combination amivantamab-
chemotherapy than with chemotherapy alone.
Links: Full Article
NEJM Quick Take
---
October 2, 2023
OSAKA, Japan and CAMBRIDGE,
Massachusetts, October 2, 2023 -
Takeda (TSE:4502/NYSE:TAK) today
announced that, following discussions
with the U.S. Food and Drug
Administration (FDA), it will be
working with the FDA towards a
voluntary withdrawal of EXKIVITY®
(mobocertinib) in the U.S. for adult
patients with epidermal growth factor
receptor (EGFR) Exon20 insertion
mutation-positive (insertion+) locally
advanced or metastatic non-small cell
lung cancer (NSCLC) whose disease
has progressed on or after platinum-
based chemotherapy. Takeda intends
to similarly initiate voluntary
withdrawal globally where EXKIVITY is
approved and is working with
regulators in other countries where it
is currently available on next steps.
---
EXCLAIM-2 (NCT04129502) Phase 3 Trial Schema
Mobocertinib 160 mg daily
-Treatment naive
-Locally advanced or
metastatic
-Nonsquamous
NSCLC
R
-EGFR ex20ins
1:1
10 endpoint: PFS by IRC
N=318
2° endpoints: ORR, OS, PFS by IA, DoR, TTR, DCR, PRO, safety
Subgroup analysis
1. Brain mets (yes vs
no)
2. Race (Asian vs non-
Asian)
Platinum/Pemetrexed X 4
Crossover to
mobocertinib
Pemetrexed maintenance
allowed
168 clinical sites
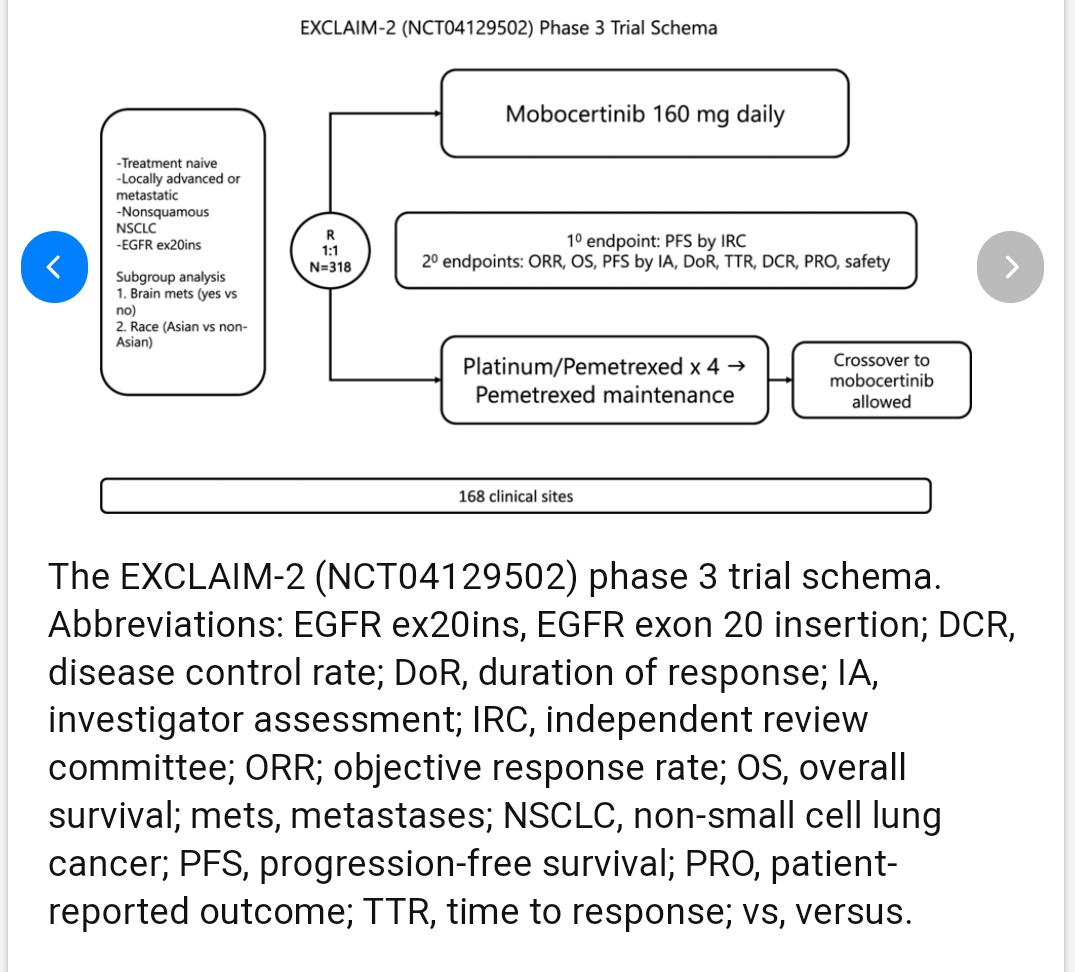
The EXCLAIM-2 (NCT04129502) phase 3 trial schema.
Abbreviations: EGFR ex20ins, EGFR exon 20 insertion; DCR,
disease control rate; DoR, duration of response; IA,
investigator assessment; IRC, independent review
committee; ORR; objective response rate; OS, overall
survival; mets, metastases; NSCLC, non-small cell lung
cancer; PFS, progression-free survival; PRO, patient-
reported outcome; TTR, time to response; VS, versus.
[Slide 1]
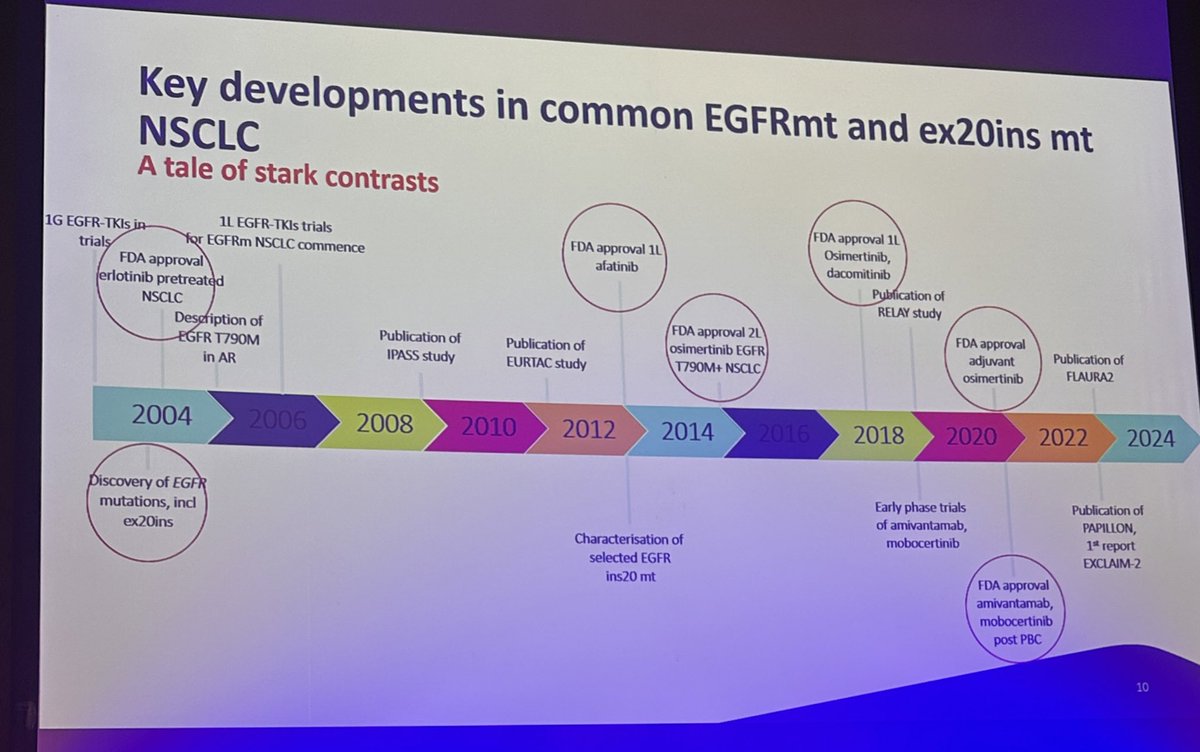
Key developments in common EGFRmt and ex20ins mt
NSCLC
A tale of stark contrasts
1L EGFR-TKIs trials
FDA approval 1L
1G EGFR-TKIs in
for EGFRm NSCLC commence
FDA approval 1l
Osimertinib,
trials
afatinib
dacomitinib
FDA approval
Publication of
erlotinib pretreated
RELAY study
NSCLC
Description of
FDA approval 21
FDA approval
Publication of
EGFR T790M
Publication of
osimertinib EGFR
adjuvant
Publication of
in AR
IPASS study
EURTAC study
1790M+ NSCLC
osimertinib
FLAURA2
2004
2006
2008
2010
2012
2014
2016
2018
2020
2022
2024
Discovery of EGFR
Early phase trials
Publication of
mutations, ind
of amivantamab,
PAPILLON,
ex20ins
Characterisation of
mobocertinib
1st report
selected EGFR
EXCLAIM-2
ins20 mt
FDA approval
amivantamab,
mobocertinib
post PBC
10
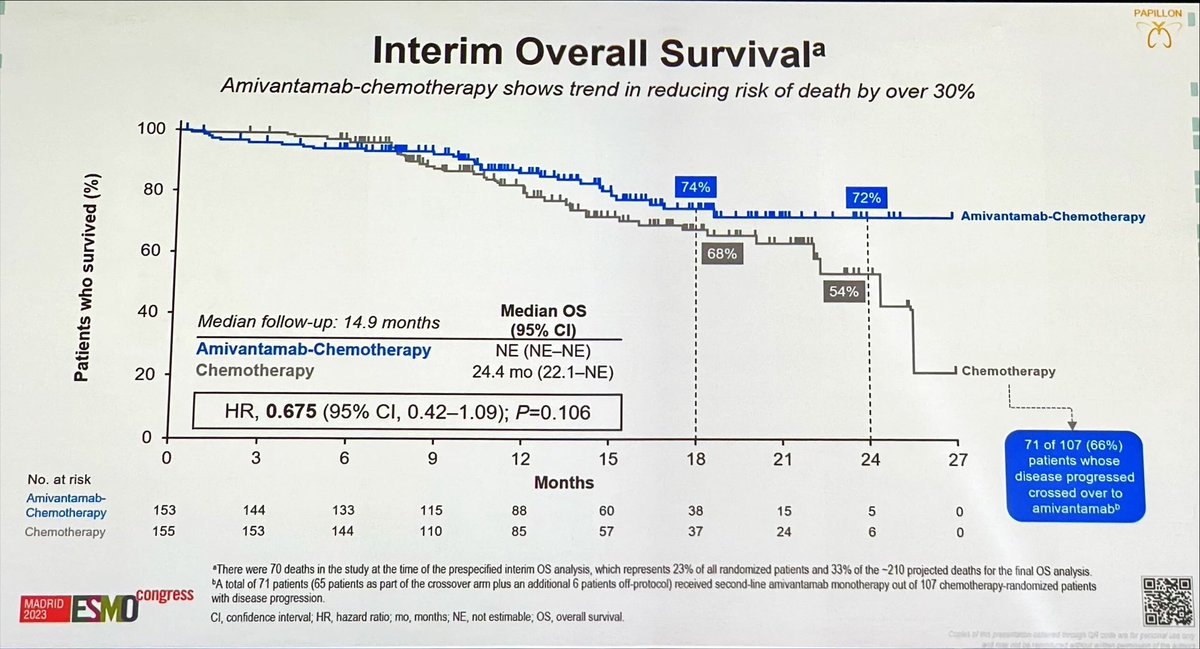
PAPILLON (NCT04538664) is the pivotal Phase 3 global trial that established amivantamab plus carboplatin-pemetrexed as a first-line standard of care for advanced NSCLC harboring EGFR exon 20 insertion mutations. Presented at the 2023 ESMO Congress and published simultaneously in the New England Journal of Medicine, the trial met its primary endpoint of progression-free survival. On March 1, 2024, the FDA granted full approval to amivantamab (Rybrevant) with carboplatin and pemetrexed for this indication — the first FDA-approved frontline regimen for EGFR exon 20 insertion NSCLC. PAPILLON is the established comparator against which newer first-line options such as sunvozertinib (WU-KONG28) are now being benchmarked.
Population
Treatment-naïve locally advanced/metastatic NSCLC with EGFR exon 20 insertion mutations.
Intervention
IV amivantamab + carboplatin-pemetrexed vs carboplatin-pemetrexed alone.
Primary Endpoint
Progression-free survival by blinded independent central review (RECIST 1.1).
Key Secondary
Objective response rate, duration of response, and overall survival.
Efficacy & Safety
Reported Results
Progression-Free Survival (Primary Endpoint)
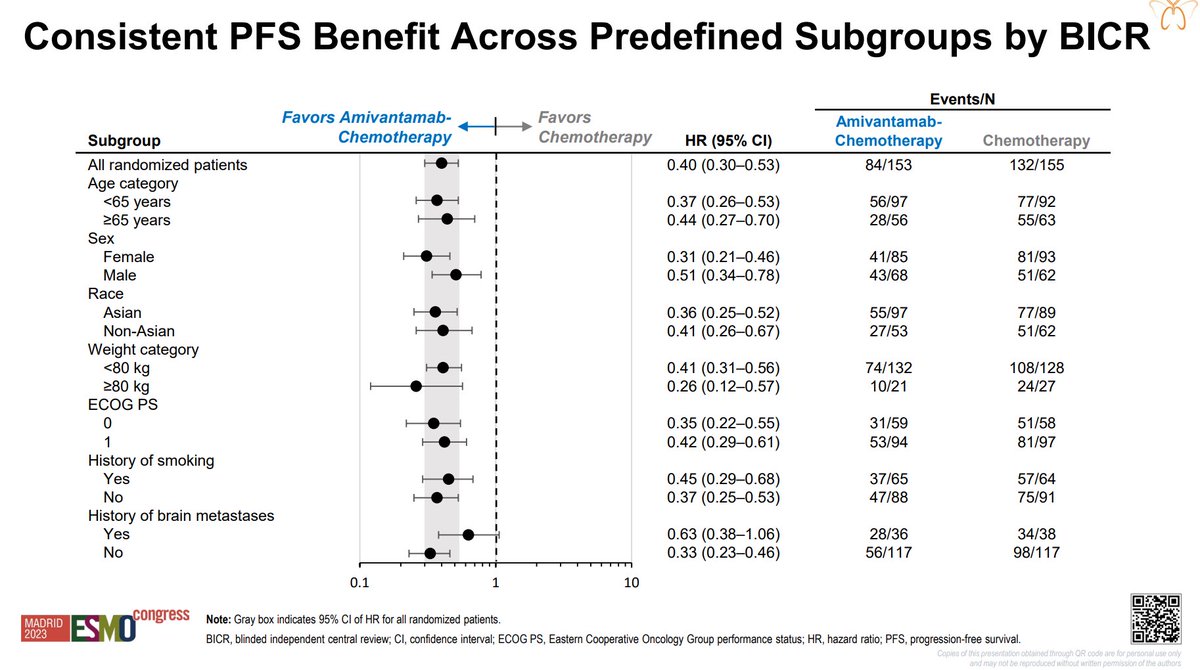
Amivantamab plus chemotherapy significantly improved median PFS to 11.4 months vs 6.7 months with chemotherapy alone (HR 0.40; 95% CI, 0.30–0.53; p<0.0001) at a median follow-up of 14.9 months.
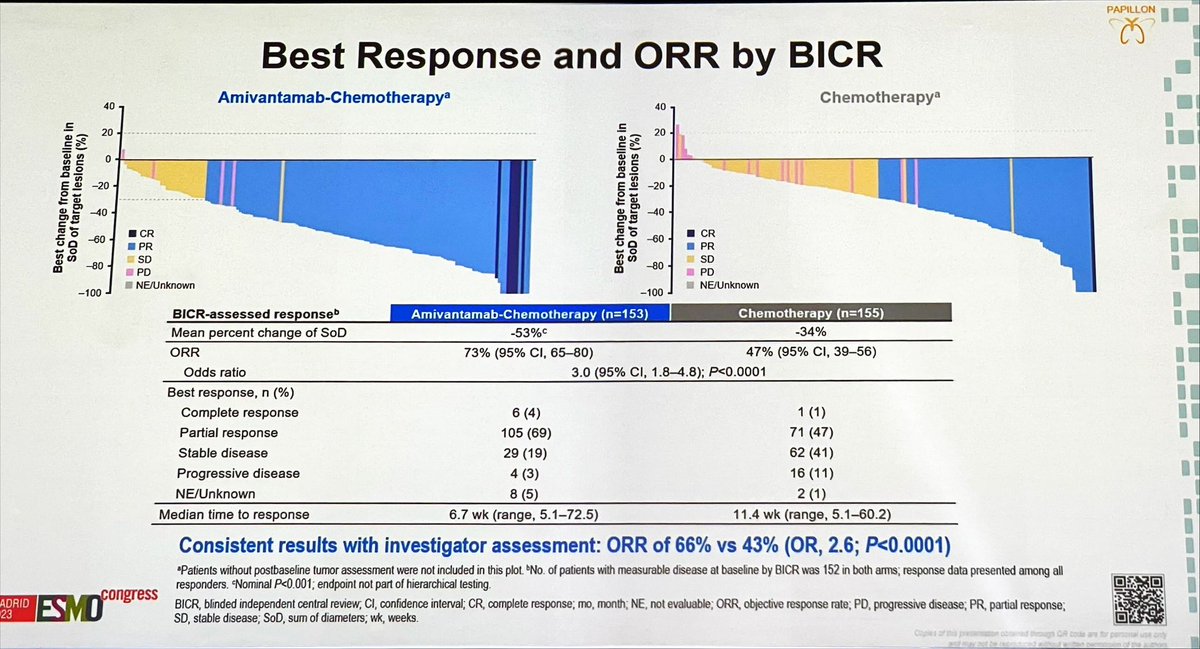
Amivantamab plus chemotherapy improved objective response rate and duration of response versus chemotherapy alone; full response figures are reported in the NEJM primary publication.
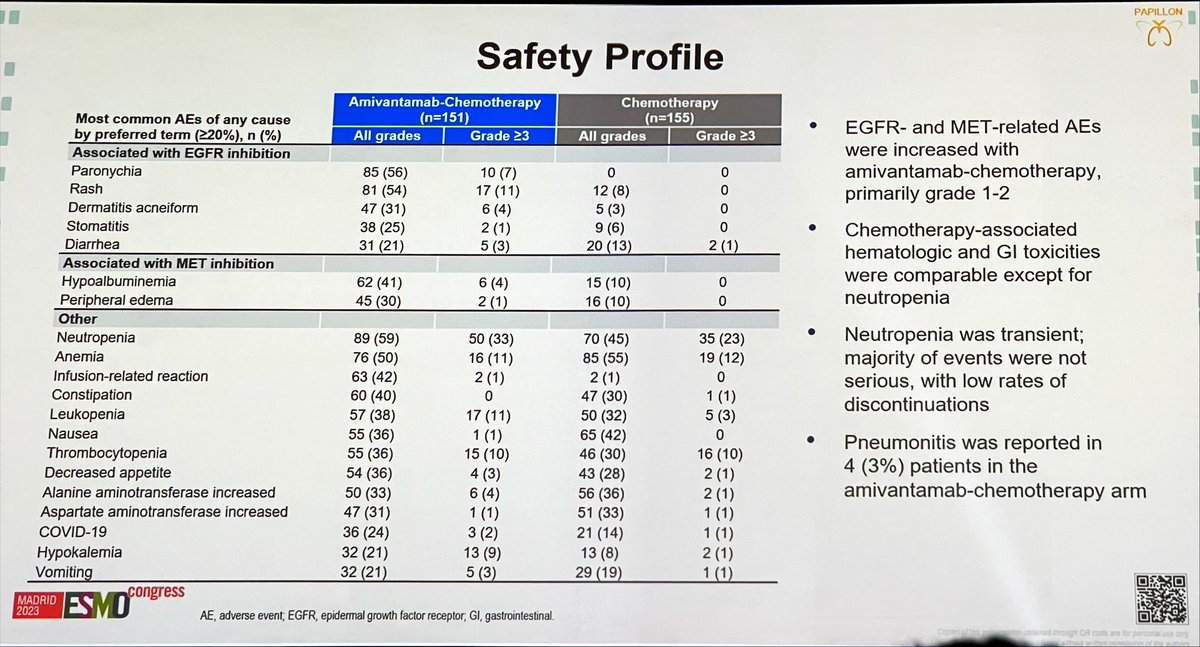
The amivantamab combination added class-typical EGFR/MET toxicities — infusion-related reactions, rash, and paronychia — on top of the chemotherapy backbone. Full adverse-event rates are detailed in the NEJM publication.
On March 1, 2024, the FDA approved amivantamab-vmjw (Rybrevant) with carboplatin and pemetrexed for the first-line treatment of locally advanced or metastatic NSCLC with EGFR exon 20 insertion mutations — the first FDA-approved frontline regimen for this population, based on the confirmatory Phase 3 PAPILLON study.