










Top 10 by impressions - click to view on X
Late breaking at #ASH23: The addition of subcutaneous daratumumab to bortezomib, lenalidomide, and dexamethasone therapy and lenalidomide maintenance therapy had a significant...
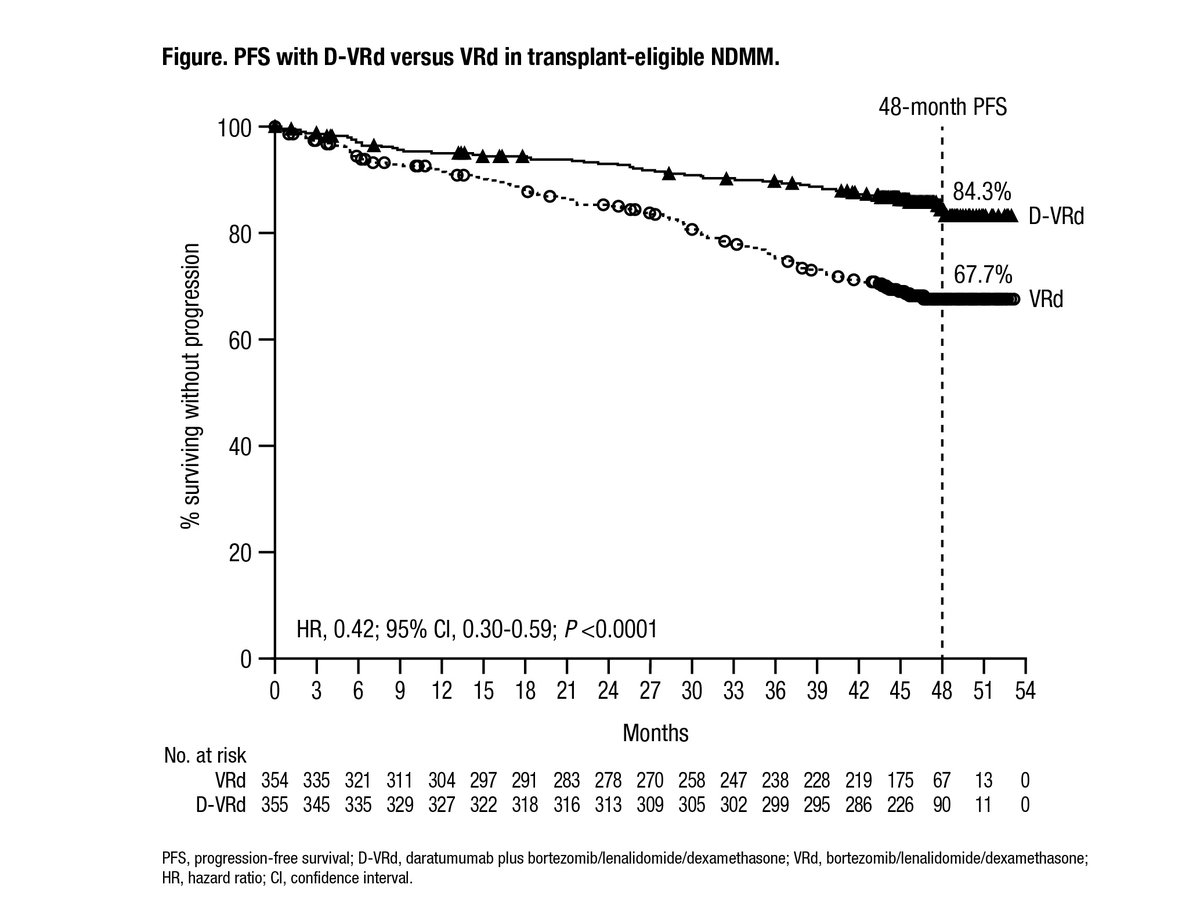
#ASH23 Late Breaking Abstract 1 PERSEUS Newly-Diagnosed Myeloma RCT 709 patients Dara-VRd vs VRd - 48-month PFS rates 84.3% vs 67.7%, HR 0.42, p<0.001 - OS: D-VRd 34 deaths...
As promised, here is my best of #mmsm #ASH23 picks. *Clinical Abstracts* Validation of GRIFFIN trial by Phase III Perseus Trial in transplant eligible NDMM:...
As promised, here is my best of #mmsm #ASH23 picks. *Clinical Abstracts* Validation of GRIFFIN trial by Phase III Perseus Trial in transplant eligible NDMM:...
Thanks @Dr_AmerZeidan for inviting me to present on current treatment of myeloma at the New England Hematologic Malignancies Symposium. A simplified algorithm of frontline therapy today....

Summary of the PERSEUS trial to be presented at #ASH23 These results further support the use of this regimen. (LBA-1 Phase 3 Randomized Study of DARA+VRd Vs Vrd Alone in Pts with...
PERSEUS➡️Important to note that NO signal for increased early mortality from toxicity with Dara-VRd compared to VRd. OS curves trending in the right direction (similar to CASSIOPEIA)! These data...
PERSEUS➡️Important to note that NO signal for increased early mortality from toxicity with Dara-VRd compared to VRd. OS curves trending in the right direction (similar to CASSIOPEIA)! These data...

🚨New update of our New algorithm ; How I treat Newly diagnosed Myeloma: If Fit/Transplant Eligible (Both High & Standard Risk): Dara/RVD x 4 cycles followed by Mel/ASCT followed by...

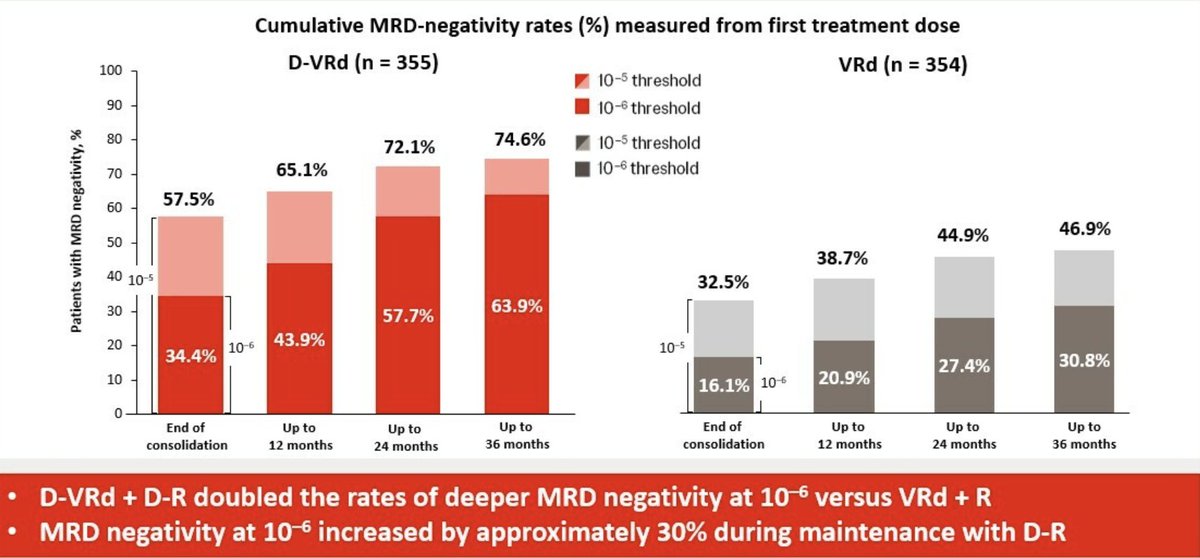
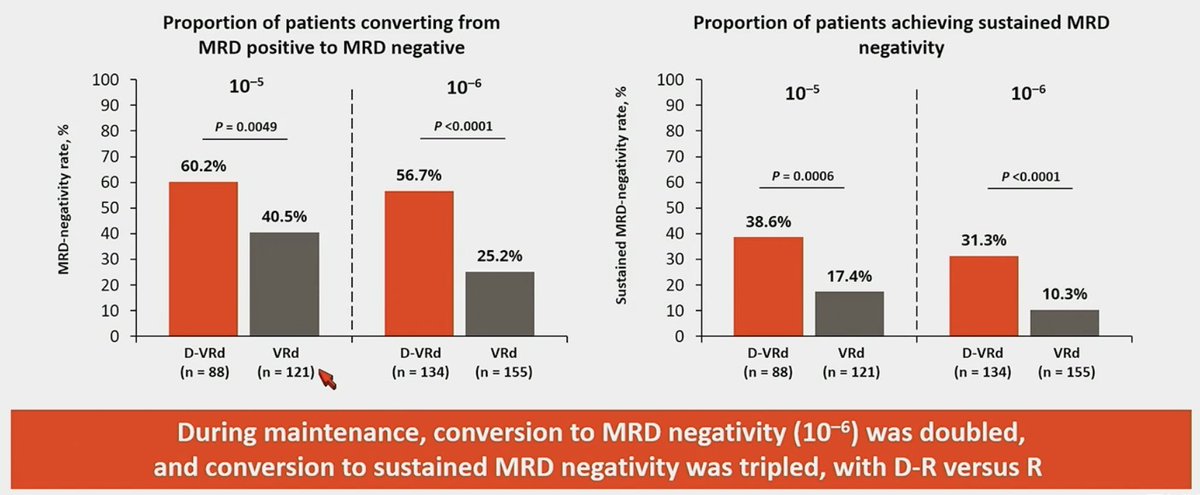
PERSEUS MRD Data: Maintenance upgraded MRD(-) responses up to 2-3 years later, and appears to be more profound with Dara-R maintenance. Dara-VRd/Dara-R doubled chances of reaching MRD negativity...
PERSEUS is a landmark Phase III, open-label, randomized trial that established subcutaneous daratumumab (Darzalex Faspro) plus bortezomib, lenalidomide, and dexamethasone (D-VRd) as a new standard of care for transplant-eligible patients with newly diagnosed multiple myeloma. The trial randomized 709 patients across 14 countries in Europe and Australia to D-VRd induction/consolidation followed by daratumumab-lenalidomide (D-R) maintenance versus VRd induction/consolidation followed by lenalidomide (R) maintenance alone. PERSEUS is the first Phase III trial to demonstrate that adding subcutaneous daratumumab to VRd with MRD-guided maintenance confers an unprecedented PFS benefit in transplant-eligible NDMM.
Phase III, multicenter, international, open-label, 1:1 randomized, active-controlled trial (NCT03710603; EMN-17) in transplant-eligible patients with NDMM ages 18-70. Patients were stratified by ISS stage and cytogenetic risk. MRD was assessed using the clonoSEQ NGS assay (Adaptive Biotechnologies) at 10^-5 and 10^-6 sensitivity thresholds.
Adults aged 18-70 with newly diagnosed multiple myeloma eligible for autologous stem cell transplant (ASCT), with ECOG performance status 0-2. A total of 709 patients were randomized (D-VRd n=355; VRd n=354). 14.8% had ISS stage III disease and 21.7% had high cytogenetic risk (t[4;14], t[14;16], or del[17p]).
Experimental arm: 4 cycles D-VRd induction (SC daratumumab 1800 mg weekly cycles 1-2, Q2W cycles 3-4, plus VRd), single ASCT, 2 cycles D-VRd consolidation, then D-R maintenance (daratumumab Q4W + lenalidomide 10 mg) for minimum 2 years with MRD-guided daratumumab stopping. Control arm: 4 cycles VRd induction, single ASCT, 2 cycles VRd consolidation, then lenalidomide maintenance until progression.
Primary endpoint: progression-free survival (PFS) assessed by IRC per IMWG criteria. Key secondary endpoints: overall complete response or better rate, overall MRD-negativity rate (10^-5 threshold), and overall survival (OS).
At a median follow-up of 47.5 months, D-VRd significantly improved PFS versus VRd alone. The PFS HR was 0.42 (95% CI: 0.30-0.59; P<0.0001), representing a 58% reduction in the risk of disease progression or death. The FDA label cites HR 0.40 (95% CI: 0.29-0.57; P<0.0001), a 60% risk reduction. Estimated 48-month PFS rates were 84.3% for D-VRd versus 67.7% for VRd. Median PFS was not reached in either arm. Subgroup analyses showed consistent PFS benefit across ISS stage III and high cytogenetic risk patients.
Overall survival data remain immature. At the time of the primary analysis, 78 deaths had occurred (D-VRd: 34 [9.6%]; VRd: 44 [12.4%]). A trend favoring D-VRd is emerging but has not yet reached statistical significance. The trial remains ongoing with OS as a key secondary endpoint.
The safety profile was consistent with known daratumumab and VRd toxicity, with no new safety concerns. Grade 3-4 AEs occurred in 91.5% of D-VRd patients vs 85.6% of VRd patients. The most common Grade 3-4 hematologic AEs were neutropenia (62.1% vs 51.0%), thrombocytopenia (29.1% vs 17.3%), and febrile neutropenia (9.4% vs 10.1%). Any-grade infusion-related reactions occurred in 6.0% with D-VRd (Grade 3-4: 0.9%). The most common overall AEs (20% or more) included peripheral neuropathy, fatigue, edema, pyrexia, upper respiratory infection, constipation, diarrhea, musculoskeletal pain, insomnia, and rash. Serious AEs occurred in 57.0% vs 49.3%.
PERSEUS established D-VRd followed by MRD-guided D-R maintenance as a new standard of care for transplant-eligible NDMM, representing a major advance over VRd alone. The MRD-guided maintenance approach allows patients who achieve sustained deep responses to stop daratumumab while continuing lenalidomide, potentially improving long-term quality of life. Key clinical debates include D-VRd versus D-VTd backbone selection (CASSIOPEIA used thalidomide), the optimal duration of daratumumab maintenance, whether MRD-guided treatment discontinuation can be extended further, and the role of quadruplet therapy in elderly patients (aged 65-70 subgroup).




























