Gotistobart vs. docetaxel in previously treated squamous NSCLC — BioNTech / OncoC4
Discover KOL Sentiment on PRESERVE-003 →Design - Two-stage, randomized, open-label Phase 3 trial of gotistobart (BNT316/ONC-392, pH-sensitive anti-CTLA-4) vs docetaxel in previously treated squamous NSCLC after PD-(L)1 progression (NCT05671510; BioNTech/OncoC4).
Overall survival (Stage 1) - 54% reduction in risk of death vs docetaxel: HR 0.46 (95% CI 0.25-0.84; nominal p=0.0102); median OS not reached vs 9.95 months; 12-month OS 63.1% vs 30.3%.
Objective response - ORR 20.0% (gotistobart) vs 4.8% (docetaxel); median duration of response 11.0 vs 3.8 months; 12-month PFS 25.2% vs 0%.
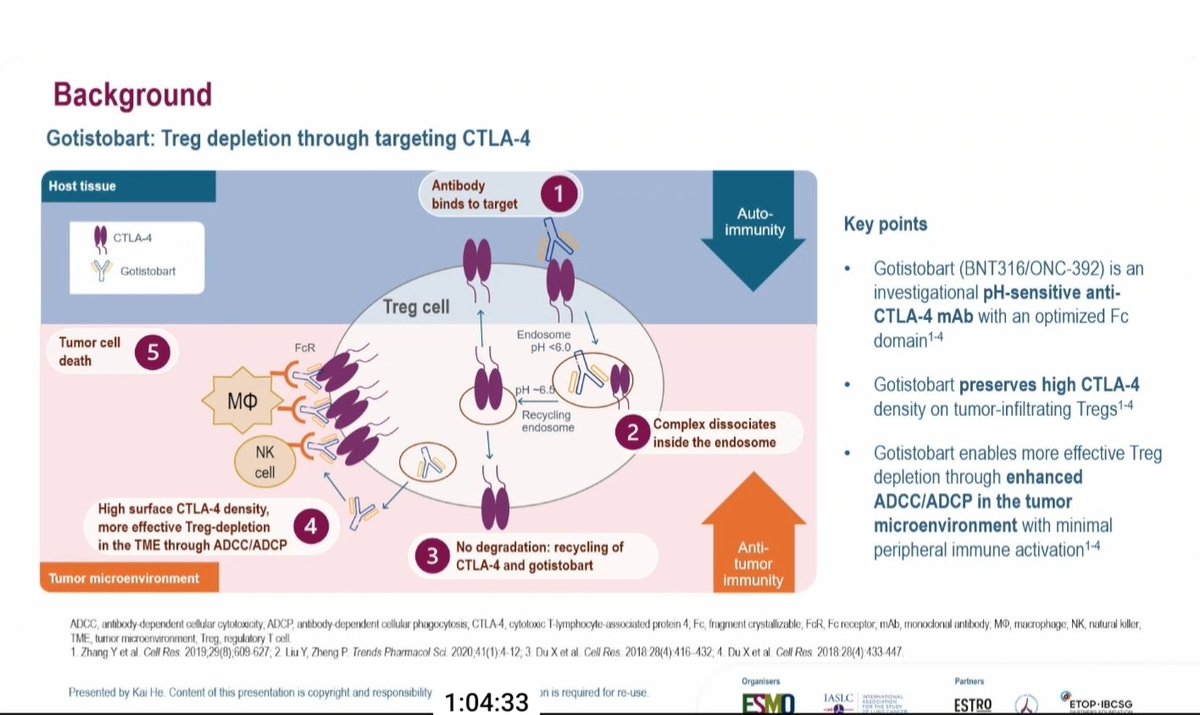
Mechanism - Gotistobart is engineered to preserve CTLA-4 density on tumor-infiltrating Tregs while enabling selective intratumoral Treg depletion, aiming to reduce peripheral immune-related toxicity.
Safety - Designed to minimize peripheral immune activation and reduce immune-related adverse events versus conventional anti-CTLA-4 antibodies.
Regulatory / sponsor - Investigational; not FDA approved (NMPA Breakthrough Therapy Designation in China). BioNTech/OncoC4.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.









Top 10 by impressions — click to view on X
💯 Most exciting “sleeper” study at #ELCC26 waking us and CTLA-4 inhibition up again for a patient subset in great need for new options! One that if holds true in larger experience would definitely pass @PTarantinoMD ‘s 4-wheeled T-test!
🔜 #ELCC26 @myESMO 🇩🇰 🔥Proffered Paper session 2 ☑️CT screening in non-risk-based population ☑️LATIFY: ceralasertib + durvalumab ☑️ETOP-Roche i-TIMES: immunotherapy timing ☑️PRESERVE-003: gotistobart vs. docetaxel 🎙️Chair: @DrSanjayPopat @APassaroMD @OncoAlert @Larvol #LCSM
🆙 #ELCC26 @myESMO 🇩🇰 🔥Proffered Paper session 2 ☑️PRESERVE-003: Gotistobart vs. Docetaxel 🎯ORR 20% vs. 4.8% 🎯mPFS 2.4m vs. 2.6m 🎙️Dr. Kai He 🎙️Chair: @DrSanjayPopat @APassaroMD 📍NCT05671510 @OncoAlert @Larvol #LCSM
Depleting intratumoral Tregs by ADCC with the FC active CTLA-4 inhibitor, gotistobart, potentially interesting but not preventing hyper progressions and crossing of survival curves. #ELCC2026
Phase 3 (PRESERVE-003): Gotistobart vs Docetaxel Post PD-(L)1 resistant sqNSCLC Early overlap → late separation (~6 months) HR 0.46 | Durable OS benefit 👉 Classic immunotherapy effect #MVOnco #NSCLC #Immunotherapy #LungCancer
Tomorrow at #ELCC26, Dr. Kai He will share data from stage 1 of the global Phase 3 PRESERVE-003 clinical trial evaluating a tumor microenvironment-selective regulatory T cell depletion candidate targeting CTLA-4 in second-line or later therapy of squamous NSCLC.
🔥 Chemo-free after IO failure in sqNSCLC? #ELCC26 Stage 1 PRESERVE-003: gotistobart vs docetaxel in post–PD-(L)1 metastatic sqNSCLC 👇 🧬 Study population •Metastatic sqNSCLC •Progressed on PD-(L)1 inhibitors + platinum chemo 💊 Trial arms •🟣 Gotistobart (CTLA-4

Top Trials to Follow on Day 3 @myESMO #ELCC26 KEYNOTE-671 | NCT06505837 | OptiTROP-Lung03 | NCT06107686 | NCT04938804 | LATIFY | PRESERVE-003 #ELCC #ELCC2026 #Cancer #Oncology #LungCancer #NSCLC #SCLC #lcsm #pembrolizumab #toripalimab #sacituzumab #YL202 #BNT326 #ceralasertib

Gotistobart shows encouraging results in squamous NSCLC 🔬 In PRESERVE-003, it improved response rates and OS vs docetaxel after prior PD-(L)1 therapy. A potential chemo-free option for a high-need population? Learn more in the article below! @myESMO #ELCC26 #lcsm

#ELCC26: Improved overall survival was observed with gotistobart, a novel anti-CTLA-4 antibody, versus docetaxel in stage 1 of the PRESERVE-003 trial in patients with squamous #NSCLC who progressed on anti-PD-(L)1 therapy. #ESMODailyReporter ➡️
PRESERVE-003 (NCT05671510) is a randomized, open-label, active-controlled, global Phase 3 trial evaluating gotistobart (BNT316/ONC-392), an investigational pH-sensitive anti-CTLA-4 monoclonal antibody, versus docetaxel in patients with metastatic squamous NSCLC who progressed on prior anti-PD-(L)1 therapy plus platinum-based chemotherapy. Gotistobart is designed to selectively deplete regulatory T cells (Tregs) within the tumor microenvironment through enhanced ADCC/ADCP while preserving peripheral CTLA-4 function, potentially reducing immune-related adverse events. Stage 1 data were presented at ELCC 2026 by Dr. Kai He and subsequently published in Nature Medicine.
Randomized, open-label, active-controlled Phase 3 trial (Stage 1: n=87). Gotistobart monotherapy vs. docetaxel in 2L+ metastatic squamous NSCLC post PD-(L)1 progression.
Patients with metastatic squamous NSCLC who progressed on anti-PD-(L)1 inhibitors plus platinum-based chemotherapy. n=45 gotistobart, n=42 docetaxel.
Gotistobart (anti-CTLA-4 mAb with pH-sensitive binding and optimized Fc domain for Treg depletion) vs. docetaxel (75 mg/m2 Q3W).
Overall survival (OS) and objective response rate (ORR) per RECIST v1.1. Secondary: PFS, duration of response (DOR), safety.
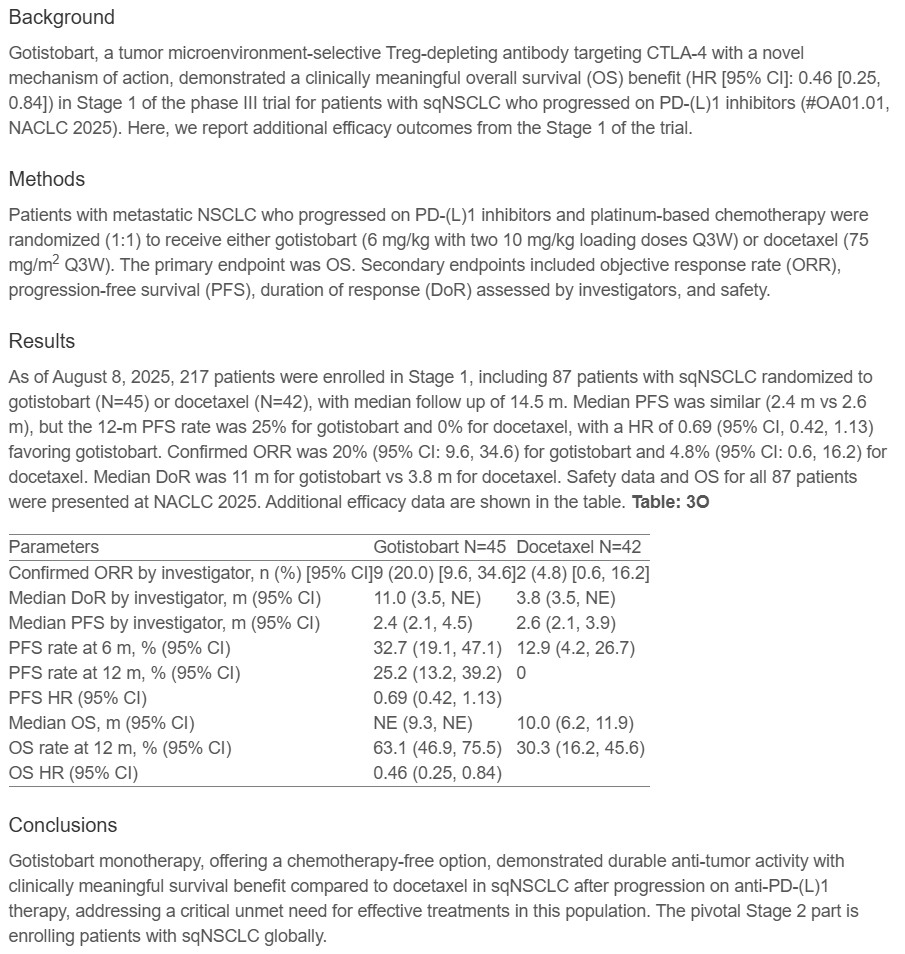
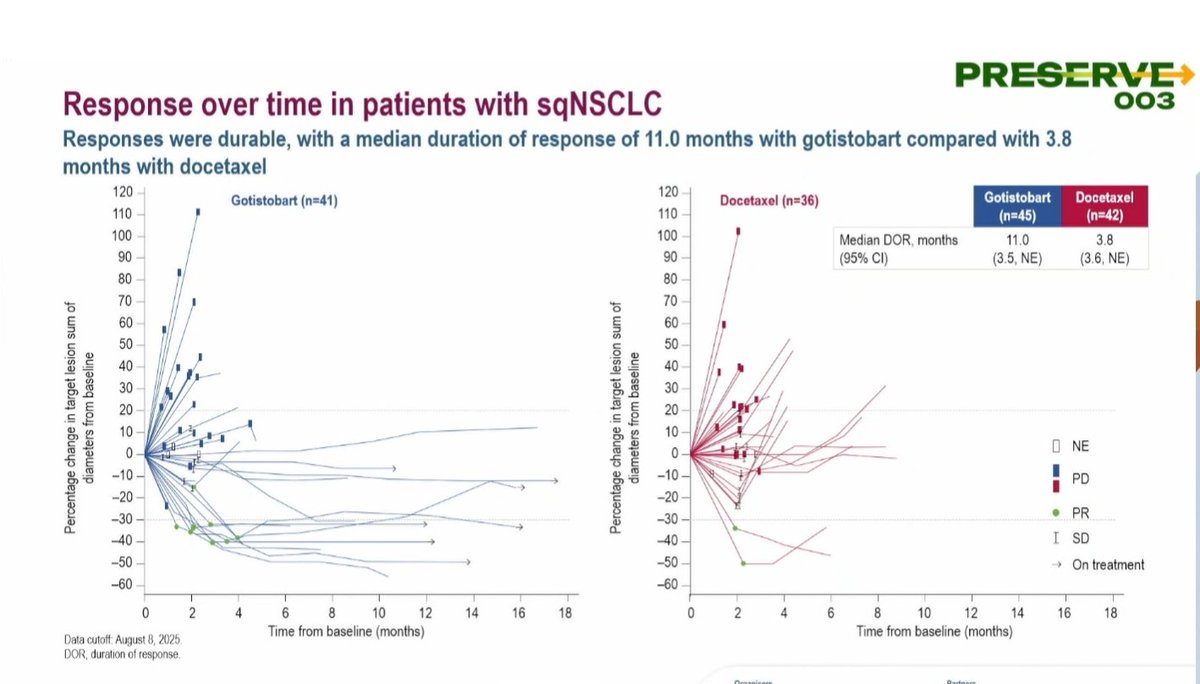
Gotistobart demonstrated a significantly higher ORR of 20.0% compared with 4.8% for docetaxel. Responses were durable, with a median duration of response of 11.0 months with gotistobart vs. 3.8 months with docetaxel. The 12-month PFS rate was 25.2% with gotistobart vs. 0% with docetaxel, though median PFS was similar (2.4 vs. 2.6 months; HR 0.69, 95% CI 0.42-1.13).
Gotistobart reduced the risk of death by 54% compared with docetaxel (HR 0.46, 95% CI 0.25-0.84; nominal p=0.0102). Median OS was not reached with gotistobart (95% CI 9.33 to NE) vs. 9.95 months with docetaxel (95% CI 6.18-11.93). The 12-month OS rate was 63.1% with gotistobart vs. 30.3% with docetaxel. OS curves showed early overlap with late separation beginning around 6 months, consistent with a classic immunotherapy effect.
Gotistobart is designed as a pH-sensitive anti-CTLA-4 antibody that preserves high CTLA-4 density on tumor-infiltrating Tregs while enabling selective Treg depletion in the tumor microenvironment through enhanced ADCC/ADCP. This mechanism aims to minimize peripheral immune activation and reduce immune-related adverse events compared with first-generation CTLA-4 inhibitors. Full safety data from Stage 1 are reported in the Nature Medicine publication.
PRESERVE-003 Stage 1 results position gotistobart as a potential chemo-free treatment option for patients with squamous NSCLC who progress after PD-(L)1 therapy, a population with limited options and high unmet need. The durable OS benefit and classic immunotherapy curve separation suggest gotistobart may offer meaningful long-term benefit for a subset of patients. Gotistobart remains investigational; the FDA has granted orphan drug designation for squamous NSCLC. Note: the FDA placed a partial clinical hold on the trial due to differing results in the nonsquamous cohort. Stage 2 enrollment continues for the squamous population.
PRESERVE-003 (NCT05671510) is a two-stage, randomized, open-label Phase 3 trial run by BioNTech and OncoC4 comparing gotistobart (BNT316/ONC-392), a pH-sensitive anti-CTLA-4 antibody, against docetaxel in patients with previously treated metastatic squamous non-small cell lung cancer whose disease progressed after a PD-(L)1 inhibitor and platinum-based chemotherapy.
In the Stage 1 readout, gotistobart reduced the risk of death by 54% versus docetaxel, with an overall-survival hazard ratio of 0.46 (95% CI 0.25-0.84; nominal p=0.0102); median overall survival was not reached versus 9.95 months, and 12-month overall survival was 63.1% versus 30.3%. The objective response rate was 20.0% versus 4.8%, with a longer median duration of response (11.0 versus 3.8 months).
No. Gotistobart (BNT316/ONC-392) is an investigational pH-sensitive anti-CTLA-4 antibody and is not FDA-approved. China's National Medical Products Administration granted it Breakthrough Therapy Designation, but it remains investigational in the United States pending further data.
Gotistobart is engineered to be pH-sensitive so that it preserves high CTLA-4 density on tumor-infiltrating regulatory T cells while enabling their selective depletion within the tumor microenvironment through enhanced ADCC/ADCP. The goal is to concentrate anti-tumor activity in the tumor while minimizing peripheral immune activation and reducing immune-related adverse events compared with conventional anti-CTLA-4 antibodies.
Patients with squamous NSCLC who progress after PD-(L)1 therapy and chemotherapy have limited options, typically docetaxel. PRESERVE-003 Stage 1 positions gotistobart as a potential chemotherapy-free option with a durable overall-survival benefit and classic immunotherapy curve separation, addressing a population with high unmet need pending confirmatory data.