SERENA-6 is AstraZeneca's Phase 3, double-blind, ctDNA-guided trial in HR+/HER2-negative advanced breast cancer. Patients who develop an emergent ESR1 mutation on a first-line aromatase inhibitor + CDK4/6 inhibitor switch to camizestrant (AstraZeneca; investigational - no approved brand name yet). At ASCO 2026 (LBA1007) the switch improved PFS (HR 0.45; 16.8 vs 9.2 months) and met PFS2 (25.7 vs 19.1 months). US FDA decision pending.
Discover KOL Sentiment on SERENA-6 →Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated June 24, 2026.






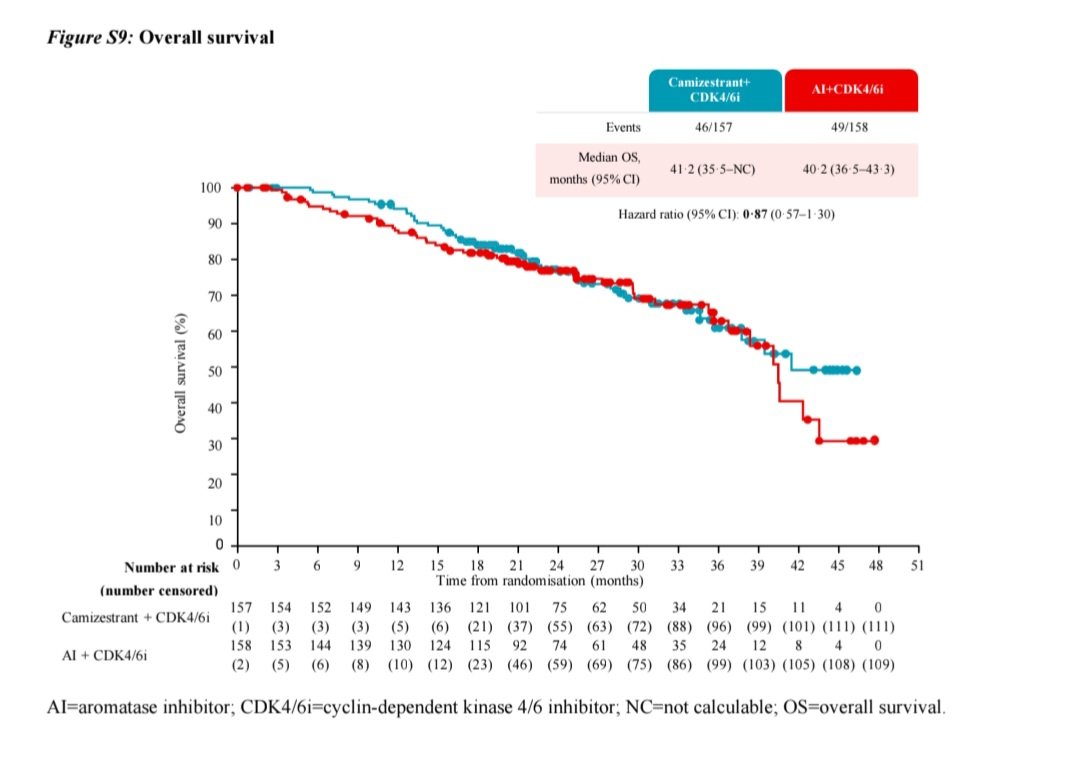
| Arm | N (events) | Median OS (95% CI) | HR (95% CI) |
|---|---|---|---|
| Camizestrant + CDK4/6i | 157 (46) | 41.2 mo (35.5–NC) | 0.87 (0.57–1.30) |
| AI + CDK4/6i | 158 (49) | 40.2 mo (36.5–43.3) |
OS data remain immature and the curves do not show a clear separation (the HR 95% CI crosses 1). From the SERENA-6 final analysis (Figure S9), published in The Lancet Oncology (Jul 14, 2026). Whether an OS benefit emerges with longer follow-up remains open.











Top 10 by impressions - click to view on X
Physician reactions to the June 2 final PFS2 + ctDNA readout (LBA1007).
Highly impactful update from SERENA6. Very nice plateau in the PFS curves with longer follow up, and dramatic reduction in ctDNA and improvement in QoL which suggests deep benefit. Harder to interpret PFS2. Hoping to have this option available for our patients soon. #ASCO26

#ASCO26 | SERENA-6 Early switch to camizestrant + CDK4/6i at the emergence of an ESR1 mutation also improved PFS2 versus continuing AI + CDK4/6i. PFS2: 25.7 vs 19.1 months✅️ HR 0.63, p=0.0037 The strategy is reasonable: intervene with ctDNA before waiting for radiologic
SERENA-6: Very robust data with updated PFS, significant PFS2, and impressive ctDNA clearance. @OncoAlert #ASCO26

SERENA-6 Trial — Final PFS2 Analysis #ASCO26 Switching to camizestrant + CDK4/6i at the emergence of ESR1 mutations in ER+/HER2− advanced breast cancer. Updated PFS: median 7.6-month improvement → HR 0.45, with 1 in 3 patients still progression-free at 24 months. PFS2
#ASCO26 SERENA-6 suggests that switching to camizestrant when ESR1m emerges, rather than waiting for radiologic progression, may be a biologically smart strategy. However, given the heterogeneous and debated nature of PFS2 as an endpoint, this study will likely remain highly

Additional data coming #ASCO26 re: #SERENA6 👀 #bcsm
The SERENA-6 PFS2 results were presented at #ASCO26. The full-text is now published, but the OS data remain immature. The current curves do not show a clear separation. Whether an OS benefit will emerge with longer F/U remains an open question.
Don't miss the thoughtful accompanying editorial by @ValenzaCarmine
< 2 wks to #ASCO25, here is a📝 of 🔑abstracts for general onc that could guide our SoC! - #ATOMIC - #MATTERHORN -...
Metastatic HR+ #BreastCancer #SABCS highlights w/ @hoperugo: ✅ #AMBRE ✅ #MONALEESA ✅ #VIKTORIA1 ✅...
Presented at #ASCO25: In patients with advanced breast cancer, switching to camizestrant with a CDK4/6 inhibitor after ESR1-mutation detection (and before disease progression) led...
The @NEJM has published SERENA-6 data ahead of @ASCO #ASCO25 plenary. Cami joins other SERDS (elacestrant, imlunestrant, vepdegestrant) with activity in ESR1mut...
SERENA-6: ctDNA guided approach to switching from AI to camizestrant upon development of ESR1m in combo with cdk4/6i demonstrates improvement in PFS! PFS2 + OS immature Could be a paradigm shift +...
Thematic take on @ASCO breast cancer abstracts: 1. Move 'em up. DB09, ASCENT-04, SERENA-6 are really just trials of using agents earlier in the course of advanced...

#SABCS2025 Francois-Clement Bidard presents updated Serena-6 data. PFS2 and time to ADC/Chemo better with early switch, ctDNA mESR1 fraction decreased. Remaining question is early vs...

#ASCO25. @drteplinsky highlights from phase 3 SERENA-6 trial that found switching to tx w camizestrant if an ESR1 mutation is detected during first-line treatment can help...
As anticipated, SERENA-6 creates a lot of questions. PFS-2 is immature and crossover was not allowed; given PFS on postMonarch & EMBER-3 combo, it is unclear to me that early switch based...

Dr. Nicholas Turner presents SERENA-6, Camizestrant + CDK4/6 inhibitor for the treatment of emergent ESR1 mutations during 1L endocrine-tx and ahead of disease progression in pts with HR+/HER2–...
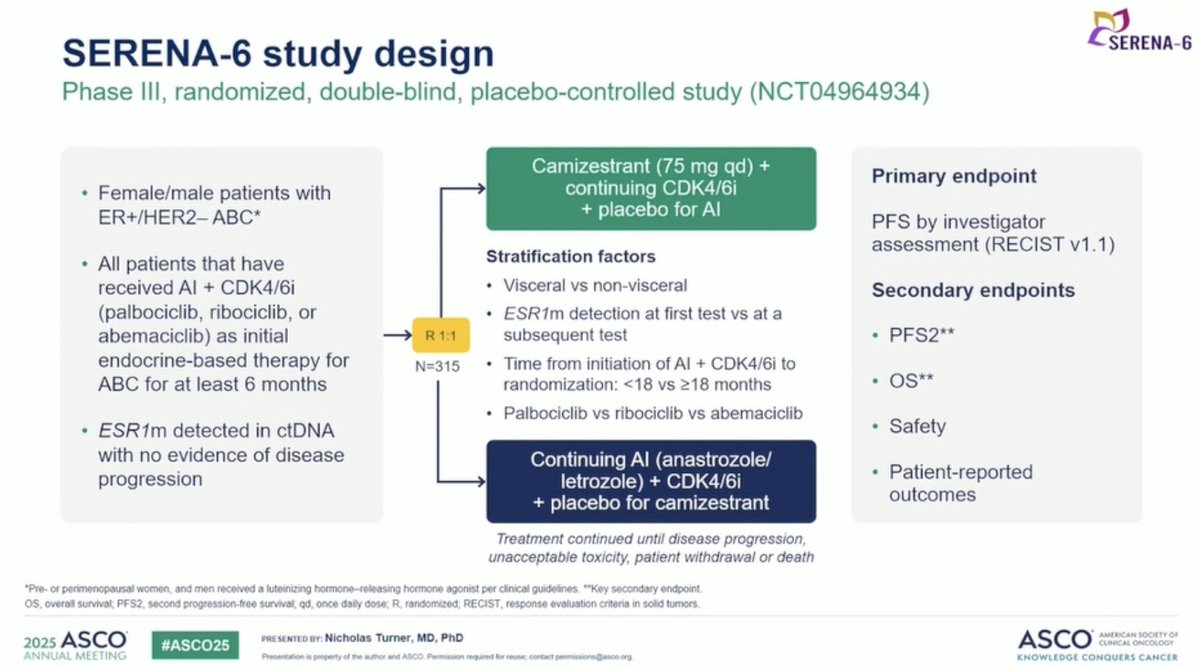
SERENA-6 is a Phase III, global, double-blind, randomized trial evaluating camizestrant, a next-generation oral selective estrogen receptor degrader (SERD), in combination with a CDK4/6 inhibitor versus continuation of aromatase inhibitor plus CDK4/6 inhibitor in patients with HR+/HER2- advanced breast cancer whose tumors develop an emergent ESR1 mutation during first-line therapy. SERENA-6 is the first registrational trial to use circulating tumor DNA (ctDNA)-guided therapy to detect endocrine resistance before clinical progression and direct a preemptive treatment switch.
Phase III, global, double-blind, randomized trial (NCT04964934). Patients on 1L AI + CDK4/6 inhibitor for at least 6 months underwent ctDNA monitoring every 2-3 months for ESR1 mutations using the FDA-approved Guardant360 CDx assay. Upon ESR1 mutation detection (without clinical/radiological progression), patients were randomized to switch to camizestrant + same CDK4/6 inhibitor or continue AI + CDK4/6 inhibitor. Stratified by time of ESR1 detection and time from AI + CDK4/6i initiation to randomization. 315 patients randomized from 3,256 screened.
Adults with HR+/HER2- locally advanced or metastatic breast cancer receiving first-line AI (anastrozole or letrozole) in combination with a CDK4/6 inhibitor (palbociclib, ribociclib, or abemaciclib) for at least 6 months with no disease progression. ESR1 mutation detected in ctDNA during routine monitoring. 315 patients randomized (approximately 1:1).
Camizestrant (oral, once daily) in combination with the patient's ongoing CDK4/6 inhibitor versus continuation of aromatase inhibitor (anastrozole or letrozole) with the same CDK4/6 inhibitor. Treatment switch triggered by ctDNA-detected ESR1 mutation, prior to clinical progression.
Primary endpoint: investigator-assessed PFS per RECIST 1.1. Key secondary endpoints: overall survival (OS) and time to second disease progression (PFS2). Exploratory endpoints: time to deterioration in global health status/quality of life (EORTC QLQ-C30), pain, and other PROs.
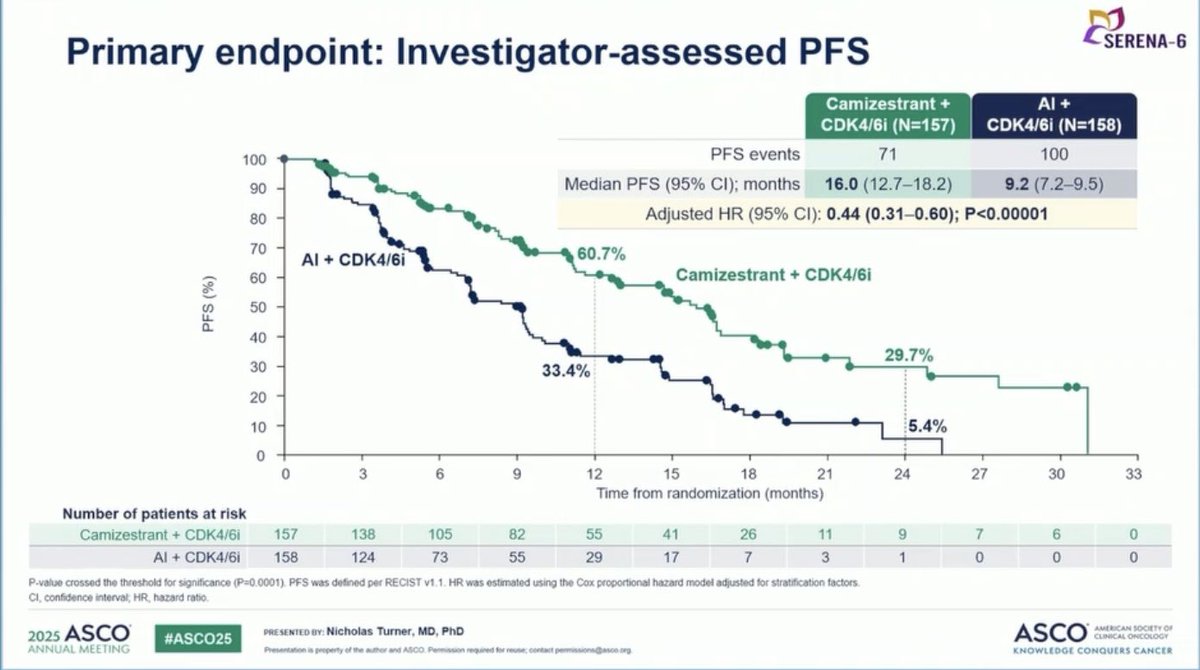
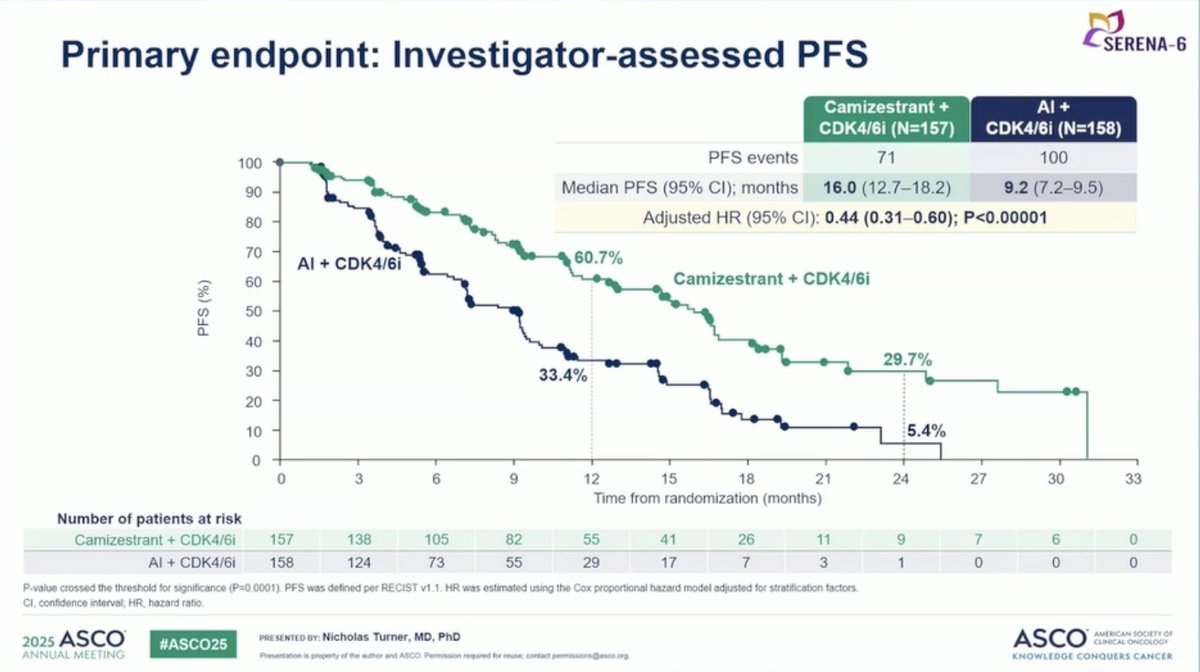
Primary analysis (ASCO 2025 / NEJM, DCO1): SERENA-6 demonstrated a highly significant PFS benefit for the ctDNA-guided switch to camizestrant. Median PFS was 16.0 months (95% CI: 12.7-18.2) with camizestrant versus 9.2 months (95% CI: 7.2-9.5) with continued AI (HR 0.44; 95% CI: 0.31-0.60; p<0.00001), a 56% reduction in the risk of disease progression or death. The 12-month PFS rates were 60.7% versus 33.4%; 24-month PFS rates were 29.7% versus 5.4%. Benefit was consistent across all CDK4/6 inhibitors and ESR1 mutation subgroups.
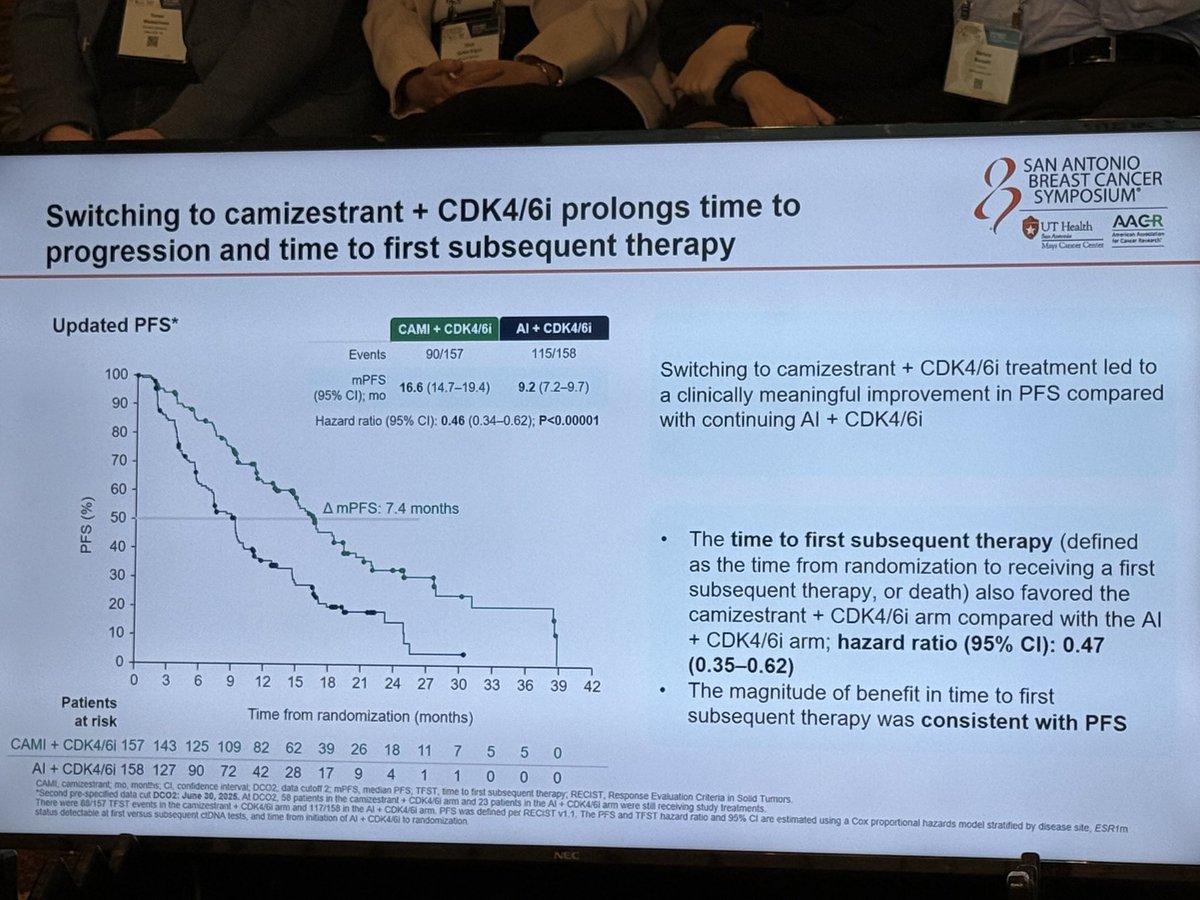
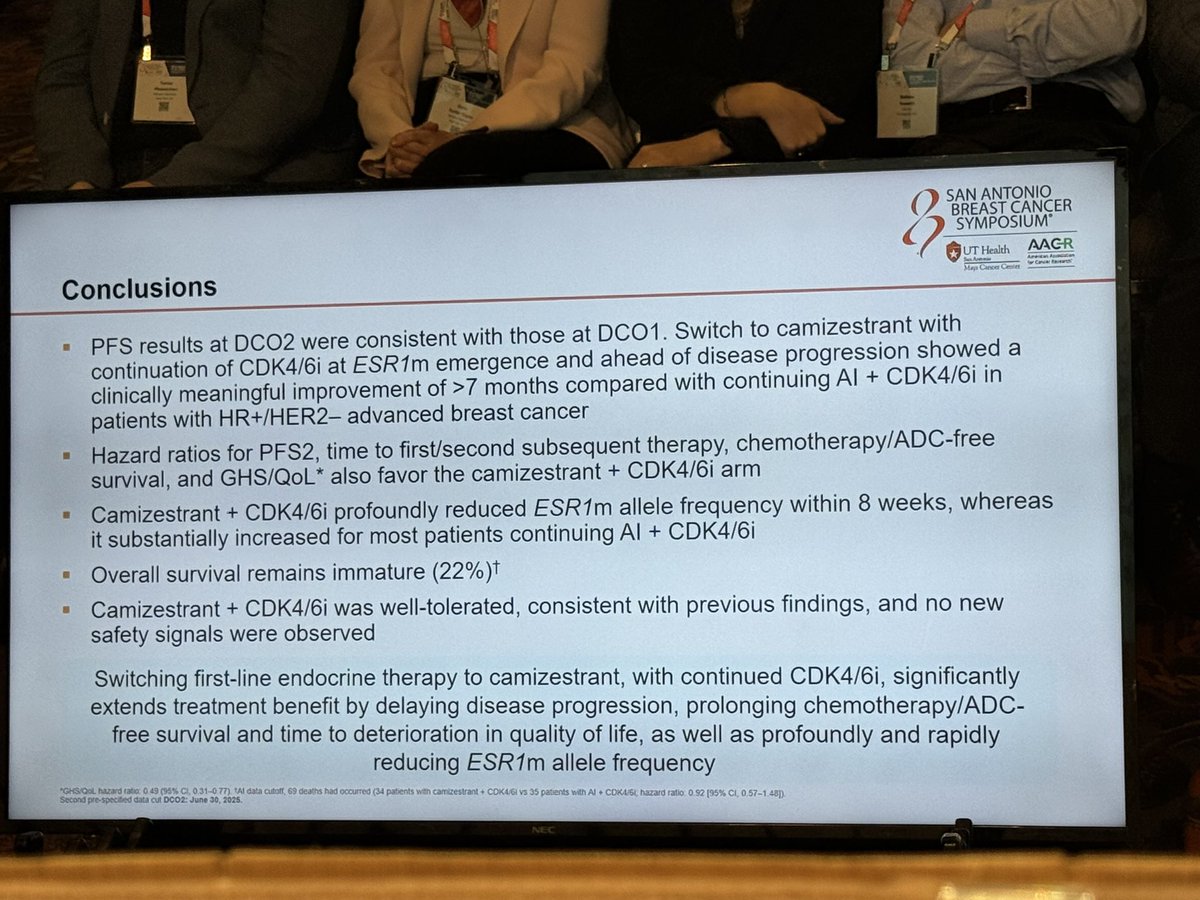
Updated analysis (ASCO 2026, LBA1007, DCO3 / Jan 2 2026, median follow-up 23.5 mo): with longer follow-up the PFS benefit deepened — HR 0.45 (95% CI 0.34-0.59; nominal p<0.00001), median PFS 16.8 months (95% CI 14.7-19.4) versus 9.2 months (95% CI 7.2-9.7), an absolute improvement of 7.6 months. At 24 months, 34.9% of camizestrant patients remained progression-free versus 14.2% on continued AI, with curves showing a durable plateau.
PFS2 (final analysis, ASCO 2026 LBA1007). PFS2 (time to second progression) showed an encouraging trend at the DCO1 interim — HR 0.52 (95% CI 0.33-0.81; 27% maturity) — that did not cross the prespecified interim significance threshold. At the final analysis presented June 2, 2026 (DCO3, 30% maturity), PFS2 was formally met: HR 0.63 (95% CI 0.46-0.86; p=0.00373; median 25.7 vs 19.1 months), with a RECIST-confirmed supplementary HR of 0.64. Camizestrant also extended chemotherapy/ADC-free survival by a median 3.9 months (22.6 vs 18.7 mo; HR 0.64, 95% CI 0.47-0.87).
ctDNA clearance (exploratory) — the analysis AstraZeneca submitted to the FDA. Switching to camizestrant produced a 99% median reduction in total ctDNA by week 8 versus a 64% increase on continued AI. Total ctDNA clearance (Guardant360) was achieved in 51% (50/98) of camizestrant patients versus 1.9% (2/108) of the control arm; in a pooled exploratory analysis ctDNA clearance was associated with an OS benefit (HR 0.39; 95% CI 0.19-0.73).
Overall survival remains immature at 30% maturity (58% information fraction; final analysis not expected until ~2028, trial powered to ~63% for OS); the DCO3 hazard ratio was 0.87 (95% CI 0.57-1.30), favoring camizestrant with confidence intervals continuing to narrow. On quality of life, the DCO3/ASCO 2026 final analysis reported a continued improvement but did not issue an updated median; the longest quantified QoL signal remains the DCO1 (ASCO 2025) primary analysis, where time to deterioration in global health status/QoL was substantially delayed — median 23.0 versus 6.4 months (HR 0.53; p<0.001; AstraZeneca PR, DCO1 — FDA briefing-doc analysis: 20.96 vs 6.37 mo, HR 0.54).
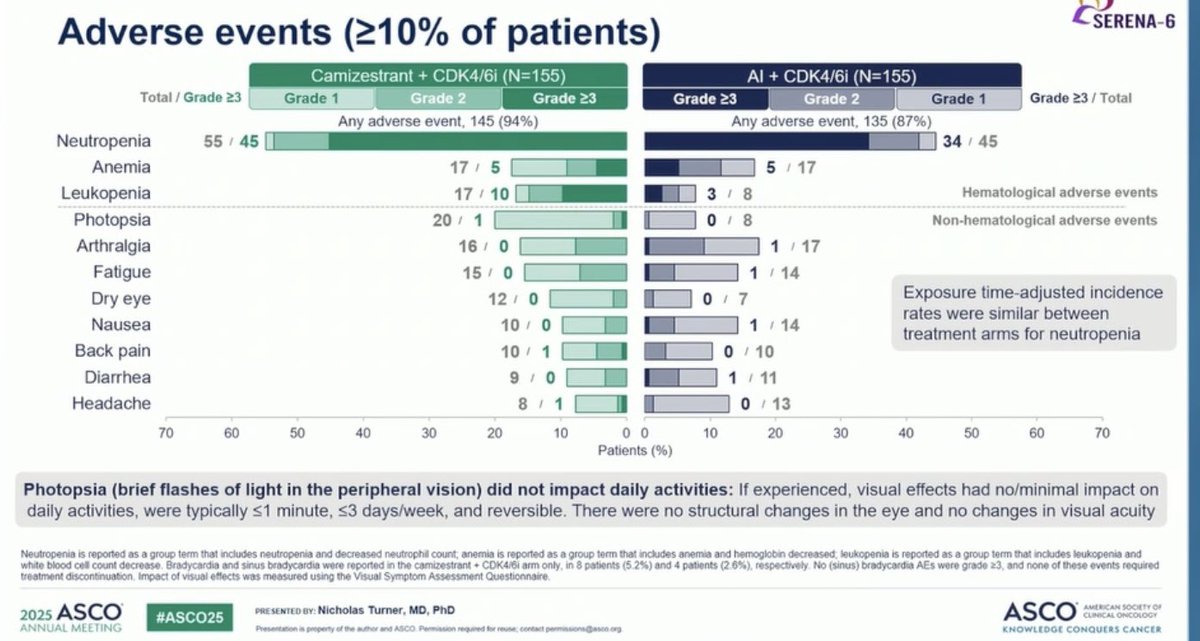
The safety profile of camizestrant was consistent with the known profiles of each component drug. Grade 3+ AEs from all causes occurred in 60% of camizestrant patients versus 46% in the AI arm, with the majority being hematological events associated with CDK4/6 inhibitors: neutropenia (45% vs. 34%), leukopenia (10% vs. 3%), and anemia (5% vs. 5%). Photopsia (brief peripheral flashes of light) was reported with camizestrant but was reversible, with no structural eye changes or impact on daily activities. Treatment discontinuation rates were very low: 1% discontinued camizestrant, 2% discontinued the AI, and CDK4/6 inhibitor discontinuation was 1% in both arms.
SERENA-6 introduces a new treatment paradigm: ctDNA-guided preemptive therapy switching before clinical progression. By detecting ESR1 resistance mutations early and switching to camizestrant, patients gained nearly 7 months of additional PFS and maintained quality of life for 17 months longer. Key questions include the feasibility and cost of routine ctDNA monitoring in clinical practice, whether this approach will be adopted broadly or remain niche, and whether the SERENA-4 trial (first-line all-comers) may obviate the need for monitoring. The regulatory verdict is split: on April 30, 2026 the FDA's ODAC voted 6–3 against the early-switch strategy (immature OS, novel PFS start-point, PFS2 not interpretable at the time), yet on May 22, 2026 the EU CHMP issued a positive opinion recommending approval. On May 27, 2026 the FDA extended the camizestrant PDUFA decision date to review additional data, which AstraZeneca presented at ASCO on June 2, 2026 (LBA1007): the now-final PFS2 was formally met (HR 0.63), and the FDA-requested ctDNA-clearance analysis showed 51% of camizestrant patients clearing total ctDNA versus 1.9% on continued AI — with early clearance linked to better long-term outcomes. Whether these data shift the US decision remains to be seen. See the Regulatory Update section below for the full timeline and latest KOL reactions.
SERENA-6 is AstraZeneca's Phase 3, double-blind, ctDNA-guided early-switch trial in HR+/HER2-negative advanced breast cancer. Patients on a first-line aromatase inhibitor plus a CDK4/6 inhibitor who develop an emergent ESR1 mutation detected by ctDNA switch to camizestrant plus their CDK4/6 inhibitor, versus continuing the aromatase inhibitor.
The primary endpoint was investigator-assessed PFS. At ASCO 2026 (LBA1007), the camizestrant early switch improved PFS to 16.8 versus 9.2 months (HR 0.45).
The key secondary endpoint PFS2 (time to second progression) was met: 25.7 versus 19.1 months (HR 0.63).
SERENA-6 used circulating tumor DNA (ctDNA) to detect emergent ESR1 mutations and trigger the early treatment switch before clinical progression. ctDNA clearance was 51% with the camizestrant switch versus 1.9% with continued aromatase inhibitor.
Camizestrant is investigational in this setting. The US FDA ODAC voted 6-3 against on April 30, 2026 and the US PDUFA date was extended; the EU CHMP issued a positive opinion on May 22, 2026.
Jul 14, 2026 — Full-text now published. The SERENA-6 final PFS2 analysis presented at ASCO 2026 has now been published in full in The Lancet Oncology, with an accompanying editorial. KOLs continue to flag immature overall survival: Yakup Ergün, MD (@dr_yakupergun) notes “the OS data remain immature … the current curves do not show a clear separation,” while Paolo Tarantino, MD (@PTarantinoMD) points readers to the thoughtful accompanying editorial.
After the April 30 ODAC vote, camizestrant's regulatory path has split sharply between the US and the rest of the world. Here is the timeline:
Sources: AstraZeneca press release (May 27, 2026) · OncLive · pharmtech · FirstWord Pharma — see Media & Publications above.
Fresh breast-oncology KOL discussion of the EU CHMP opinion and the FDA decision-date extension, curated from X (May 22–27, 2026). Tweet text is verbatim.
BREAKING: the @FDAOncology will extend the PDUFA date to review additional data to support the approval of camizestrant based on the SERENA-6 trial.

🔥 NEWS Camizestrant with a CDK4/6i recommended for approval in the EU by CHMP for advanced ER+ BC at detection of ESR1 mutation, before clinical progression. After all the post-ODAC discussions, for me this is a wonderful news, especially for patients
Additional data coming #ASCO26 re: #SERENA6 👀 #bcsm

🩸 SERENA-6 is a test of whether we are ready to treat molecular progression before radiographic progression in HR+/HER2− advanced breast cancer. In pts on 1L AI + CDK4/6i with emerging ESR1 mutations by ctDNA, switching to camizestrant + CDK4/6i improved PFS: 16.0 vs 9.2

The Europeans have approved camizestrant upon emergence of an ESR1 mutation. In light of the 6-3 ODAC against this, I wonder if the EU vote will sway the FDA 🤔 #bcsm

LBA1007 SERENA-6 Final PFS2: ctDNA-guided early switch to camizestrant on emergent ESR1m. Primary PFS shown at ASCO 2025 (HR 0.44). FDA ODAC reviewed pre-ASCO.

🩸 The oral SERD story | Tue Jun 2 | Hall D1. persevERA (LBA1006): giredestrant + palbociclib vs letrozole + PALBO in 1L HR+/HER2-. Press release: NEGATIVE. Oral SERDs don't beat the AI when given to everyone upfront. …but SERENA-6 (LBA1007) asks a smarter question: don't…

The problem is, who will pay for ctDNA testing until ESR1 arise? How many times we should test? Should we combine it with radiologic imaging? And if we detect both ESR1 mut and radiologic PD, will camizestrant be reimbursed in that case? So, nice approval, complex implementation
April 30, 2026 — The FDA Oncologic Drugs Advisory Committee (ODAC) voted 6–3 against recommending approval of camizestrant (AstraZeneca) for ESR1-mutant HR+/HER2− advanced breast cancer based on the SERENA-6 ctDNA-guided early-switch strategy. Reviewers cited concerns about immature OS data, the surrogate endpoint (PFS measured from ESR1-mutation detection), and whether the strategy meaningfully improves patient outcomes.
Why it's contested: Cami supporters argue PFS extension is meaningful and that ESR1-guided switch is a novel paradigm. Critics argue the OS curves are immature and that PFS with a biomarker-triggered switch may not translate into real clinical benefit.
Click any thread tab to see the full discussion. Threads ranked by total KOL discussant count (replies + quote-tweets). Replies in green, quote-tweets in blue. Wall Street, stock-promo, and analyst chatter excluded.

Not sure I had seen this before— Kaplan-Meier curve for overall survival in SERENA-6, with a median follow up of 23.5 months and 30% maturity https://t.co/Wtg2zFJNm2 https://t.co/cXfuOGphiL

Very important data. Even in the absence of oral SERD at crossover, there is no apparent OS benefit as yet for switch based on molecular ESR1mut detection without radiological progression. And in current practice, all

SERENA6、まだ30% maturityとしても、今のところOSに関しては延長の傾向もなさそうだな… https://t.co/mZ8Q5QVSDM

で、そのOSがどうなってるかというと画像的PD前から経口SERDを使ってもmaturity 30%の途中経過���ほとんど曲線は重なっている。しかも2026年の今や画像的PDになれば経口SERDを使うのが標準治療になっているので、実臨床はこの差はさらに縮まりそう。 https://t.co/qZhLHHRSmf

Clueless! https://t.co/iafUUb7zQH

Good catch. With 30% maturity, this is just the trailer. The late separation is interesting, but will the HR hold with further follow-up?

Grok feels like there will be OS benefit, may have to wait beyond 2028.. Grok OS prediction for SERENA-6 (camizestrant + CDK4/6i vs AI + CDK4/6i) based on the PFS data:The PFS benefit is exceptionally strong — HR 0.44 (

Yeah what about that HR?
Clueless
At risk patient in single digits during the late curve separation, doesnt mean much

There is no late separation, median follow-up is about 24 months, you can't look at the tail of the curve yet. This is a no OS benefit curve, results completely immature.

There is no real late separation. It’s just a function of very few patients at that point in the curve. There is no OS signal with current data.

Agree, just an statistical artifact

➡️As a biomarker advocate, this decision needs commenting. #SERENA6 proves #camizestrant has strong drug activity in emerging ESR1m disease, stronger than approved SERDs post-progression. FDA accepts PFS without OS for other SERDs at radiographic progression; the higher bar htt

Exactly https://t.co/UJBUMkBd3N
I wonder if they chose conservatism- don’t forgot prostate ca patients are treated for biochemical progression

If you’re worried having a coherent causal estimand will “harm precision oncology”, it needs harming. The amount of unjustifiable hype around ctDNA is absurd on many levels

At its core, it��s a choice between speed and consistency. In this case, regulators chose consistency. Totally agreed with @FDAOncology

Thank you for sharing! Agree that there are the two separate questions that you posed. As a community oncologist, it is really the molecular switch strategy that’s getting the most interest. SERENA6 screened 3256 pts a
Cheaper and accessible
eventually WGS ctDNA will be cheap. ddPCR is very cheap already

It is much more expensive. Periodic ctDNA compared to just at progression to see if there is the mutation or not to decide….

Should blame the trial sponsor for who didn’t allow for cross-over and therefore the most important piece of data is missing to answer the most important question of: does it matter to get Camizestrant earlier vs later?
A lot of trials from this sponsor don’t allow for crias-over in other settings 😅
Was the early vs later use the most important question for the other trials you have in your mind though?
This is really the takeaway from today's #ODAC vote 6-3 against recommending approval of #camizestrant at this time based on #SERENA6. We don't know yet what the benefit of an early switch in the absence of radiographic PD is long term. PFS2 as designed here doesn't answer. http

As patients, most of us want the same thing: promising science, thoughtful drug development, & clear evidence that new approaches will meaningfully help patients live better & longer. Today’s FDA ODAC discussion

Do you think if crossover allowed or including QoL measures as 1° or 2° endpoint would have made a difference? I sure would have pushed for that if I, as someone #NotDeadYet w/ MBC, had been involved in early stages of t
I mean, all speculation...but yes, if crossover had been allowed and patients did BETTER if they got cami EARLIER, 💯 we'd have an approval right now in my opinion. When this trial enrolled, patients didn't have access
Totally agree with this result We need more time to see details of OS https://t.co/aNV1BTs8rj
This is so dumb. ODAC is really filled with morons.

FDA suggests a new clinical trial: Arm A — Early Intervention Strategy Imediate switch to: camizestrant + CDK4/6 inhibitor Arm B — Standard Strategy Continue: aromatase inhibitor (AI) + CDK4/6 inhibitor Switch to: camize
The current paradigm, based on radiological progression, has critical limitations: It detects resistance at an advanced stage; it reflects a phase of higher tumor burden and clonal diversity; and it reduces the effective

The N needed to answer early vs. late will be a magnitude bigger. As a society, we need to decide if we want more trials (smaller) on more MOAs OR do we want bigger trials on fewer MOAs. Which philosophy over time will
Didn’t Serena-6 show a >9 mo improvement in ESR1 mt 🤔@oncoalert #bcsm https://t.co/Q63bj4Nmzn

In met Prostate Ca, darolutamide is FDA-approved for M0 (non-metastatic) CRPC with the goal of preventing clinical progression — i.e., bone mets. These are pts with only biochemical progression (M0 disease) who have an a
I’m not really 😉
And who puts patients on Fulvestrant monotherapy? We needed Cami.
Exactly
Imagine how in might work in combo, which is more likely scenario post progression on a CDK4/6 inhibitor.
Where did you get the 9 months period ?
https://t.co/SFzKbaclML There will be people who agree & disagree with @US_FDA decision on #SERENA6 #cami, but fantastic document by FDA 👏 educating & clearly outlining reasons for the decision and how PFS2 will be interpreted. A must read for drug developers and pharm
Promising precision oncology strategy, but not yet practice-changing until FDA review is complete. https://t.co/JZHAuv65FL

Trial design insufficient to answer the clinical question (Not that Cami isn't effective -PFS hazard ratio of 0.44 is real). The question: whether ctDNA-guided early switching is better than switching at radiographic pro

Şunu inceleyelim 🤔 https://t.co/tAgkaPoO2N
💯! Perfectly stated 🙌

Agree. The analysis was enlightening and overall the emphasis on cross-over is important moving forward. One interesting comment was the fall off in numbers of baseline to 3 mo QOL responses. @OncoAlert
Fascinating read - have only gotten through part but if I download it I’ll have hours and hours to read all 99 pages on ✈️ next week, although I won’t be able to talk to you about it in person!
UPDATED JUNE 2026: Top rows capture the ASCO 2026 (#ASCO26) reaction to the June 2 final PFS2 + ctDNA readout (LBA1007). Below those are the post-ODAC reaction (April 30, 2026 vote 6–3 against) and earlier ASCO 2025 / SABCS 2025 commentary.








































What is ironic is that ODAC (albeit with slightly different composition) voted overwhelmingly for capivasertib plus abiraterone in PTEN-deficient mHSPC. Loss of PTEN is another resistance driver. - PFS and OS magnitude
What is ironic is that ODAC (albeit with slightly different composition) voted overwhelmingly for capivasertib plus abiraterone in PTEN-deficient mHSPC. Loss of PTEN is another resistance driver. - PFS and OS magnitude
What is ironic is that ODAC (albeit with slightly different composition) voted overwhelmingly for capivasertib plus abiraterone in PTEN-deficient mHSPC. Loss of PTEN is another resistance driver. - PFS and OS magnitude
You probably also heard during the discussion that the treatment paradigm is changing extremely quickly - oral SERDs were not yet standard of care for 2L when SERENA-6 was originally designed. Were they then supposed to
I don’t think this hinges on OS. But the important point here is that trials are limited by what we know at the start and by availability of next Rx. And this is impossible to fix. @OncBrothers @OncoAlert
Altho we all want cami approval it is important to note the novel & futuristic trial design. Changing Rx for resistance markers vs PD. Lack of crossover an issue in determining LT benefit. Low return of QOL docs. We
Agree with this comment and approach. This is the holy grail of oncology therapy. Reacting to biology and microscopic changes before macroscopic manifestation. With the same information regarding clonal evolution, we wou
The trial design muddied causality FDA is apprehensive this would have quietly rewritten the rules — something they have an immune reaction to unless the data are unassailable. FDA still licking wounds from prior appr
The lag between when a trial is designed and when a trial starts, and the changes in SOC that occur in that timeframe, are a problem. How can we fix this?
Disagree, the unmet need in breast cancer significantly lower. Wrong indication selection.
How would you have designed the trial?
Dude, the problem was the design and integrity of the data, not the strategy. You don’t change how it’s done till you have convincing evidence of a better way. Masterly inactivity. This came close, but no cigar.
Dude, just say you don't believe in PFS.
Yes, I caught this part. Was really puzzled.
Advisory committees need to be banned. If I ever have cancer before hilariously being run over by a parrot driving a Tesla, I'm going to break every law in the book to get myself a cure.
And also, how would you design this trial, please say it!
AZ should’ve answered FDA’s real question — does switching at ESR1m beat switching at progression? That’s not 20/20 hindsight—FDA telegraphed discomfort with early-switch (2021) and PFS2 limits (2024). AZ chose 🚀spee
A crossover design would have had a much bigger N. oSERD would have stopped other clones stopped by AI. Again, at the end of the day, society has to decide how to allocate patients and $$ towards development of new dru
Don’t put words in my mouth. PFS is great, but show me where r=1 to OS. The biggest problems were TTD not in SAP and limitations in quality after 12w, no BICR PFS2 (and not reg EP anyway), on background of novel Tx parad
In context of novel treatment paradigm, x-over would have made sense, whereas in current paradigm (at rPD) it would not have given oSERD not established SoC. oSERD may stop eSR1m clone, but you don’t know that it stops a
Ha. Left to you, there would be no need to run a trial at all. Anyway, N was like 300, for a blockbuster indication that accrued v quickly. Hardly prohibitive to increase that. No point discussing further; bar is higher
AZ traded ~25–40% NPV for speed to first-mover positioning — not irrational, but high regulatory risk, imo
This decision is disgusting and cruel. It almost doubled PFS and should be conditionally approved on QoL metrics as well. MoA is proven and strong.
John is arguing for a crossover trial if I am not mistaken. This would confound the OS on the control arm, and requiring a bigger and longer trial. Serena-6 screened 3325 patients to get 315 ESR1m. You are basically ask
Add to it a relative small population. Makes a crossover trial very challenging. It confounds the OS. It will take much longer to read out
Thanks for your thoughts 👏🏻👏🏻👏🏻
Besides massive cost to use an experimental agent in crossover.
There were no SERDs available when this trial started, but suspect FDA would have accepted the control arm switching over to cami on radiographic progression to answer early v late question, even if it confounded OS
You’re answering a biology question (does SERD work in ESR1m), But, FDA is asking a timing question (is earlier better than later) — and SERENA-6 never actually tests that.
Crossover matters. The FDA correctly identified that Serena-6 compares early versus never, not early versus late. For my work in thoracic oncology, this methodology lesson is invaluable. We need cleaner data.
Maybe true at trial start—but 2021–24 saw SERDs emerge AZ could’ve prospectively built sequencing (e.g., switch to SERD at progression, even investigational) FDA’s issue isn’t >wrong control< —it’s failure to tes