SKYSCRAPER-01 is a Phase 3 trial of the anti-TIGIT antibody tiragolumab plus atezolizumab versus atezolizumab alone as first-line therapy for PD-L1-high (TPS >=50%) metastatic NSCLC. It was negative on both co-primary endpoints: progression-free survival (7.0 vs 5.6 months; HR 0.78) did not cross the significance boundary, and final overall survival (23.1 vs 16.9 months; HR 0.87; p=0.22) was not significant. Tiragolumab is investigational. Sponsor: Roche/Genentech.
Discover KOL Sentiment on SKYSCRAPER-01 →Design — Phase 3, randomized, double-blind; tiragolumab (anti-TIGIT) + atezolizumab vs atezolizumab alone, 1L PD-L1-high (TPS >=50%) metastatic NSCLC (NCT04294810). (AACR 2025 / primary + final analyses)
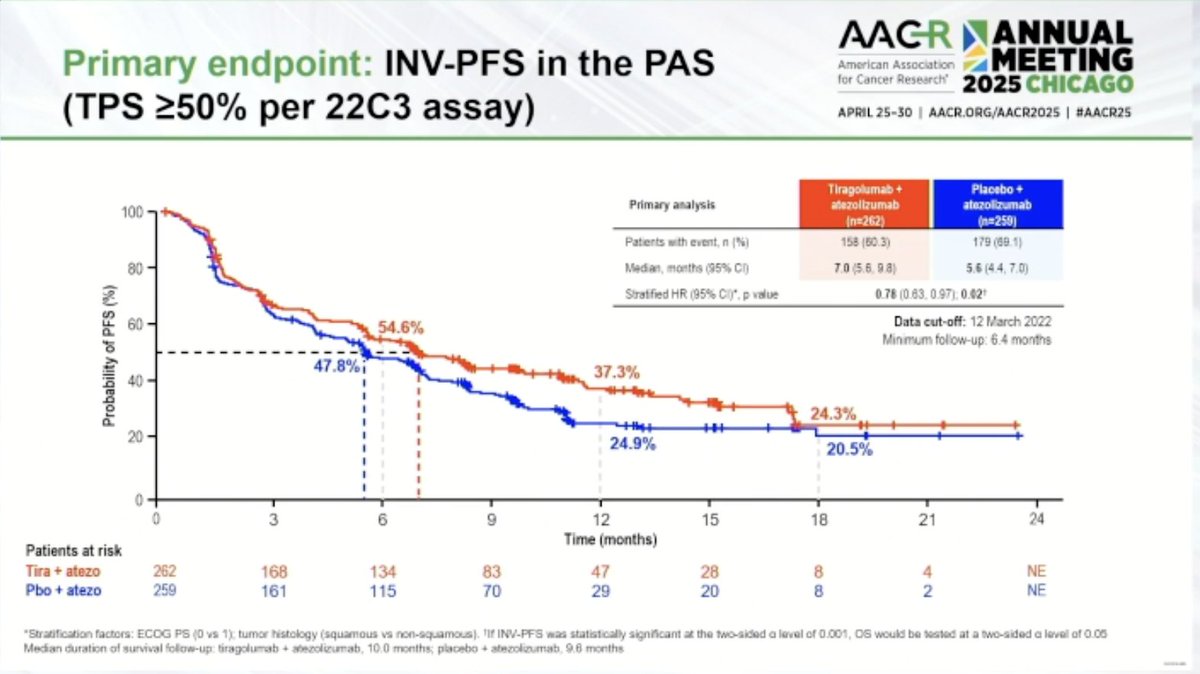
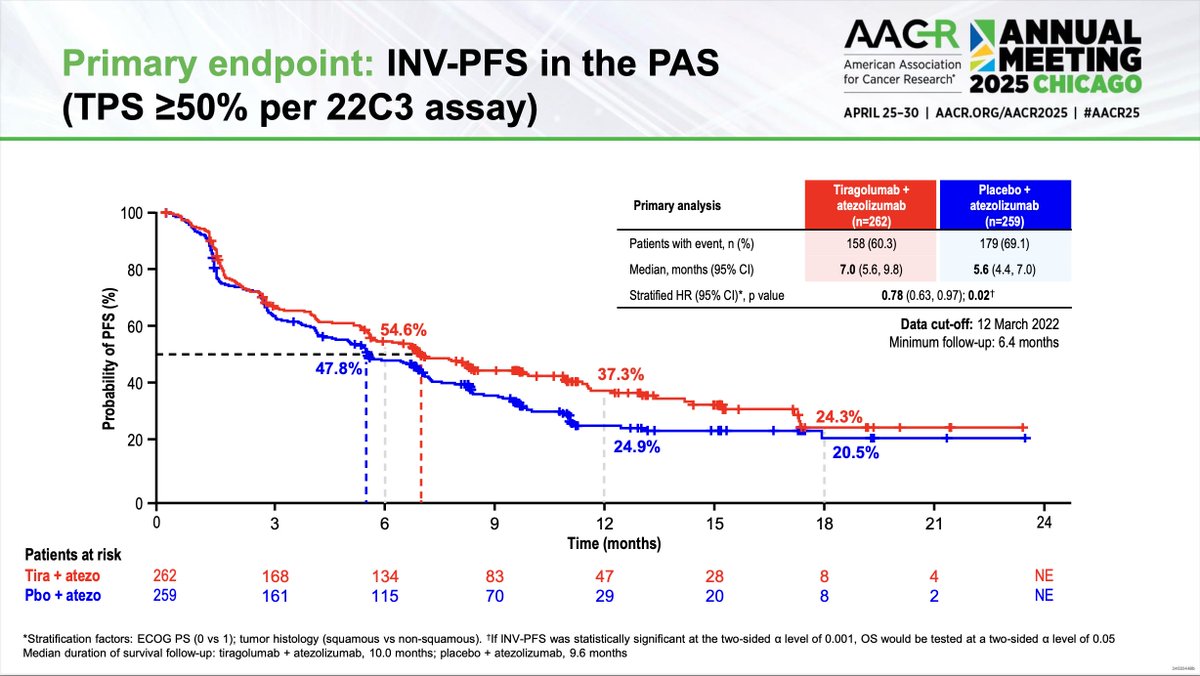
PFS (co-primary) — FAILED — median 7.0 vs 5.6 months (HR 0.78; 95% CI 0.63-0.97; p=0.02); did not cross the pre-specified significance boundary. (primary analysis)
Overall survival (co-primary) — FAILED — final median 23.1 vs 16.9 months (HR 0.87; 95% CI 0.71-1.08; p=0.22), not statistically significant; data cutoff September 24, 2024. (final OS analysis)
Safety — Higher toxicity with the combination: treatment-related Grade 3/4 AEs 19.9% vs 9.5% (roughly double); immune-mediated AEs 70.0% vs 50.6%; AE discontinuation 16.1% vs 6.5%. (primary/final)
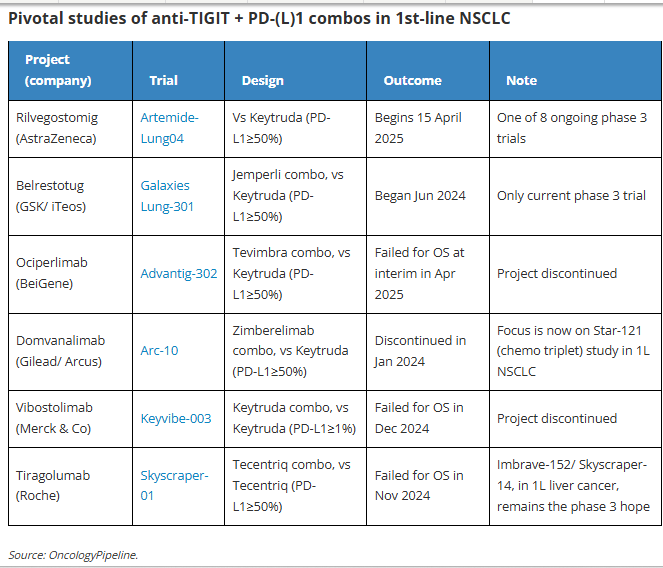
Class implication — A major setback for the anti-TIGIT class; Roche's broader SKYSCRAPER program failed across multiple tumor types (NSCLC, SCLC, cervical, esophageal, liver). (KOL commentary)
Regulatory / Sponsor — INVESTIGATIONAL — tiragolumab is not FDA approved and the combination was negative. Roche / Genentech. (FDA / trial reports)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.











Top 10 by impressions - click to view on X
🍨Genentech is dissolving its cancer immunology group and its VP of cancer immunology Ira Mellman will leave the company Mellman, who discovered endosomes, led all cancer research at Genentech before...
Dr. @peters_solange presents SKYSCRAPER-01: tiragolumab + atezolizumab vs. atezo + placebo in 1L PD-L1 high advanced NSCLC As we had seen on prior press-release there is no statistically...
SKYSCRAPER-01 presented at #AACR25 by Dr. @peters_solange: phase III study of first-line atezolizumab + tiragolumab (anti-TIGIT) or placebo in PD-L1 high NSCLC. Some...
Hardly anyone thought $RHHBY Skyscraper-01 Tigit postmortem was worth covering, so I decided to take a look. Via @ApexOnco -> #AACR25
No significant benefit with co-targeting PDL1 and TIGIT in NSCLC. Though there is an interesting positive trend in all outcomes (PFS, ORR, OS). Additional biomarkers needed to define who benefits.
Say a prayer for $GSK $ITOS & $AZN in #Tigit
#Skyscraper01 #TIGIT #Tiragolumab Inadvertent disclosure...? What is this? - Tiragolumab+Atezo: 22.9 months [95% CI: 17.5, NE] - Atezo: 16.7 months...

🆙#AACR25 #LCSM in advance 🔥#CT051 - SKYSCRAPER-01: Tiragolumab + atezo vs placebo + atezo in patients with previously-untreated PD-L1-high, locally...

JUST In: @Roche SKYSCRAPER-01 latest—> The phase 3 trial found adding anti-TIGIT tiragolumab to PDL1 atezolizumab does not prolong OS despite initial trend in 2023 ! Via...

$ROG $RHHBY Roche Pharma Day 2024 Sept 30,2024 #TIGIT Final OS results for Ph III (SKYSCRAPER-01) in 1L PD-L1 high NSCLC expected in Q4 2024 $MREO $ITOS $RCUS $AGEN $BGNE $NVS $AZN...
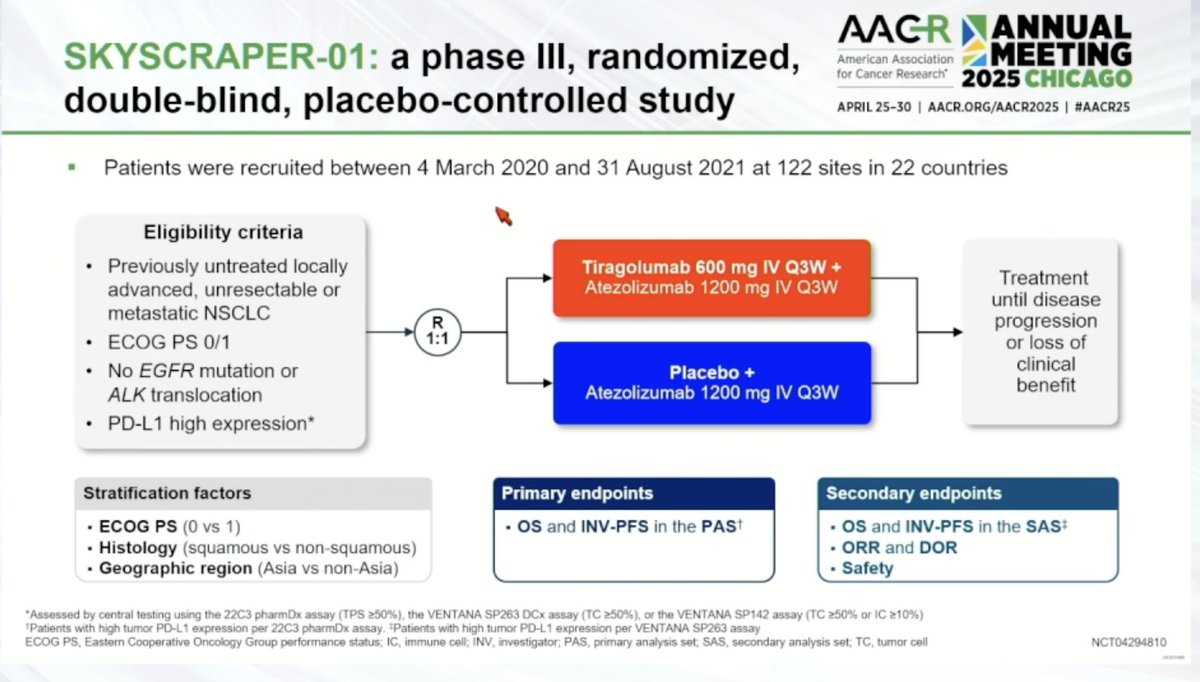
SKYSCRAPER-01 is a Phase III, global, double-blind, placebo-controlled trial that evaluated the addition of tiragolumab (an anti-TIGIT antibody) to atezolizumab (Tecentriq) versus atezolizumab alone as first-line treatment for patients with PD-L1-high (TPS >=50%) locally advanced unresectable or metastatic NSCLC. The trial FAILED both co-primary endpoints of investigator-assessed PFS and overall survival. The study enrolled 534 patients (521 in the primary analysis set) across a global, 1:1 randomized design. SKYSCRAPER-01 was initiated based on promising phase 2 CITYSCAPE data, but the phase 3 results did not replicate the earlier signal, marking a major setback for the TIGIT inhibitor class.
Phase III, global, double-blind, 1:1 randomized, placebo-controlled trial (NCT04294810). Patients were stratified by ECOG PS (0 vs. 1), histology (squamous vs. nonsquamous), and geographic region (Asia vs. non-Asia). PD-L1 high expression was centrally assessed using the 22C3 pharmDx IHC assay (TPS >=50%). No companion diagnostic was co-developed.
Adults with previously untreated, locally advanced unresectable or metastatic NSCLC with high PD-L1 expression (TPS >=50% by 22C3 assay), ECOG PS 0-1, no EGFR mutation or ALK translocation. Primary analysis set (PAS): 521 patients (262 combination, 259 control). Full analysis set: 534 patients.
Tiragolumab 600 mg IV plus atezolizumab 1200 mg IV every 3 weeks versus placebo plus atezolizumab 1200 mg IV every 3 weeks, administered on day 1 of each 21-day cycle until disease progression, loss of clinical benefit, or unacceptable toxicity.
Co-primary endpoints: investigator-assessed PFS and OS in the primary analysis set (TPS >=50% per 22C3 assay). Secondary endpoints: OS and PFS in the secondary analysis set (TC >=50% per SP263 assay), ORR, DOR, and safety. Statistical design allocated only 0.001 alpha to PFS, with 0.049 alpha for OS.
The trial FAILED its PFS endpoint. At the primary analysis (minimum follow-up 6.4 months), median PFS was 7.0 months (95% CI, 5.6-9.8) with tiragolumab + atezolizumab versus 5.6 months (95% CI, 4.4-7.0) with atezolizumab alone. The PFS HR was 0.78 (95% CI, 0.63-0.97; p=0.02), representing a 22% numerical reduction in risk, but the p-value of 0.02 did NOT clear the prespecified alpha threshold of 0.001. The 18-month PFS rates were 24.3% vs. 20.5%. A final PFS analysis at 9.9 months median follow-up confirmed median PFS of 7.0 months.
The trial FAILED its OS endpoint. At the final OS analysis (minimum follow-up 36.8 months; data cutoff September 24, 2024), median OS was 23.1 months (95% CI, 17.7-28.8) with the combination versus 16.9 months (95% CI, 14.6-21.3) with atezolizumab alone. The OS HR was 0.87 (95% CI, 0.71-1.08; p=0.22), a non-significant 13% reduction in risk of death. The 36-month OS rates were 38.3% vs. 33.6%. The OS HR deteriorated from earlier interim signals (0.82 at first interim, 0.81 at second interim) to 0.87 at the final analysis.
The combination showed higher toxicity. Grade 3/4 all-cause AEs: 41.2% vs. 33.8%. Treatment-related Grade 3/4 AEs: 19.9% vs. 9.5% (approximately double). Immune-mediated AEs: 70.0% vs. 50.6% overall; Grade 3/4 irAEs: 16.1% vs. 9.9%. Treatment discontinuation due to AEs: 16.1% vs. 6.5%. Systemic corticosteroids required: 24.3% vs. 12.5%. Key immune toxicities included rash (42.4% vs. 19.0%), hepatitis (20.2% vs. 17.1%), adrenal insufficiency (5.6% vs. 0.12%). Grade 5 TRAEs: 1.5% vs. 0.8%.
SKYSCRAPER-01 represents a definitive failure for tiragolumab in 1L PD-L1-high NSCLC, and more broadly a major blow to the TIGIT inhibitor class. Roche's entire SKYSCRAPER program has now failed across multiple tumor types (NSCLC, SCLC, cervical, esophageal, liver cancer), with the company discontinuing most studies by early 2025. The phase 2 CITYSCAPE data that inspired this trial (PFS HR 0.29 in PD-L1-high subgroup) proved to be one of the most misleading signals in recent oncology. Other anti-TIGIT molecules (domvanalimab, rilvegostomig, belrestotug) remain in phase 3 testing. The failure raises fundamental questions about whether TIGIT is a viable therapeutic target.
SKYSCRAPER-01 (NCT04294810) is a Phase 3, randomized, double-blind trial of the anti-TIGIT antibody tiragolumab plus atezolizumab versus atezolizumab alone as first-line therapy for PD-L1-high (tumor proportion score >=50%) locally advanced or metastatic non-small cell lung cancer. It was sponsored by Roche/Genentech.
No. SKYSCRAPER-01 was negative on both co-primary endpoints. Median progression-free survival was 7.0 versus 5.6 months (HR 0.78; p=0.02) but did not cross the pre-specified significance boundary, and at final analysis median overall survival was 23.1 versus 16.9 months (HR 0.87; 95% CI 0.71-1.08; p=0.22), which was not statistically significant.
No. Tiragolumab, an anti-TIGIT monoclonal antibody, is not FDA approved for any indication. The tiragolumab plus atezolizumab regimen studied in SKYSCRAPER-01 is investigational and failed to demonstrate a statistically significant benefit. Atezolizumab (Tecentriq) is separately approved in NSCLC, but the tiragolumab combination is not.
SKYSCRAPER-01 is widely viewed as a definitive failure for tiragolumab in first-line PD-L1-high NSCLC and a significant blow to the anti-TIGIT class more broadly. Roche's wider SKYSCRAPER program subsequently failed across multiple tumor types, and most of those studies were discontinued.
Yes. The combination roughly doubled treatment-related Grade 3/4 adverse events (19.9% vs 9.5%) and increased immune-mediated adverse events (70.0% vs 50.6% any-grade), with treatment discontinuation due to adverse events of 16.1% versus 6.5% — added toxicity without an offsetting survival benefit.


