Resectable gastric or gastroesophageal junction (GEJ) adenocarcinoma — AGITG (Australasian Gastro-Intestinal Trials Group) with EORTC, TROG, CCTG intergroup
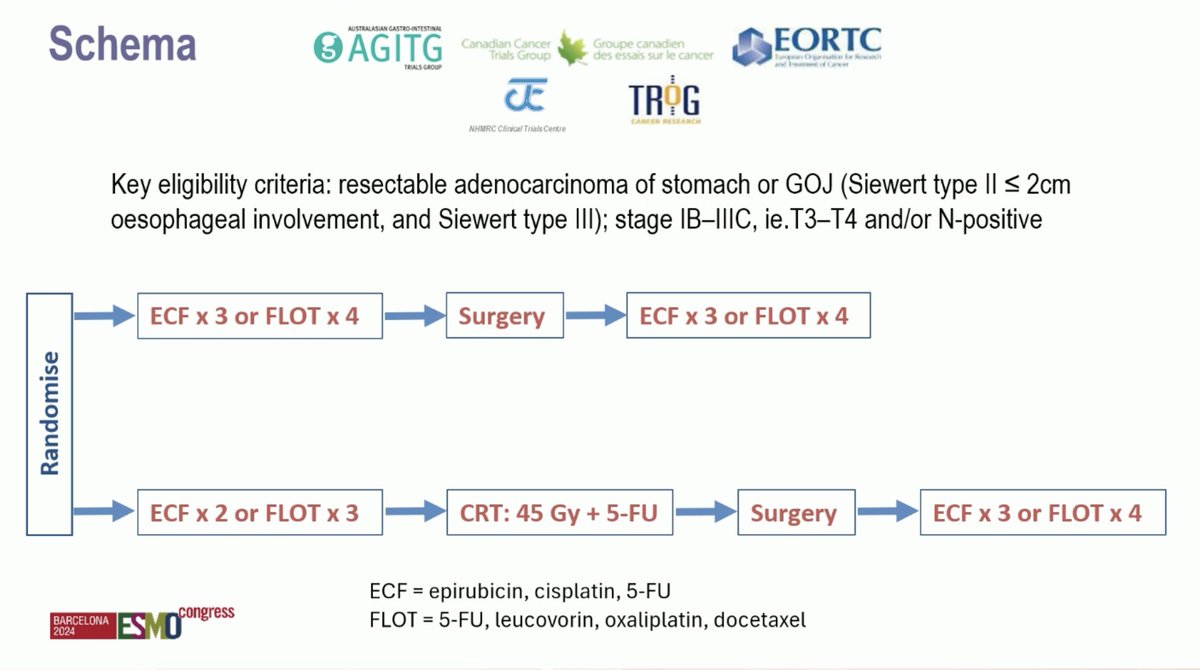
Discover KOL Sentiment on TOPGEAR →Design - Phase 3 intergroup: preop chemoradiation + perioperative chemo (Arm B) vs perioperative chemo alone (Arm A, ECF or FLOT), resectable gastric/GEJ adenocarcinoma (NCT01924819), N=574; primary OS.
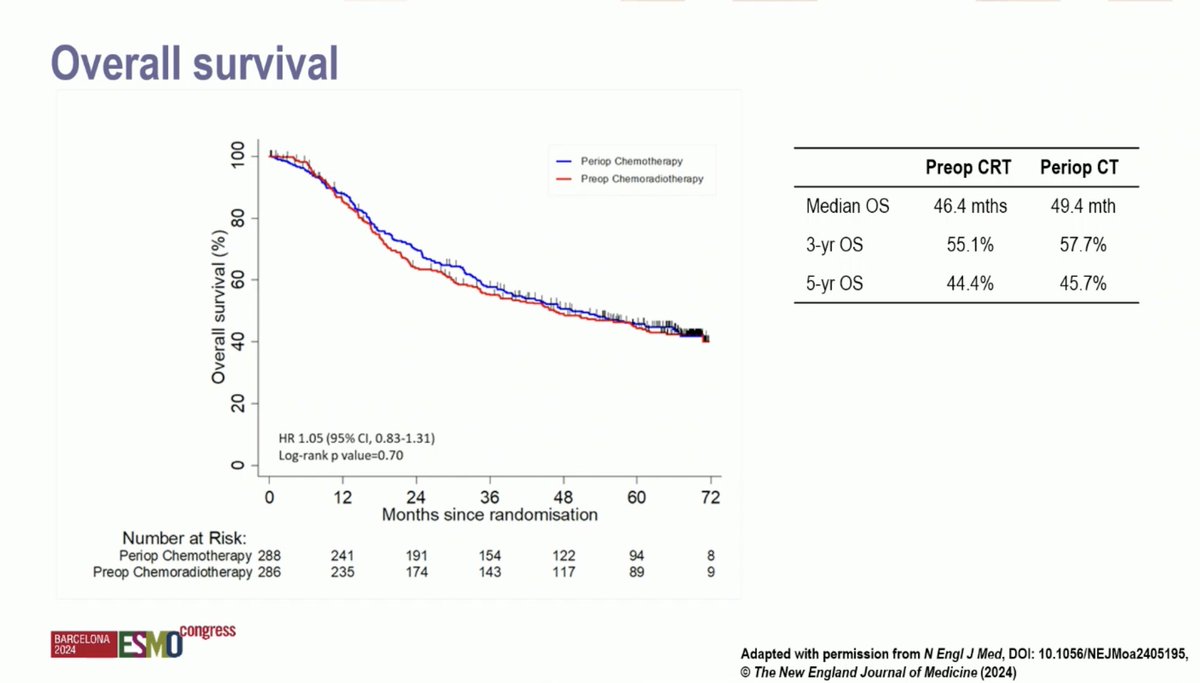
OS (primary, NEGATIVE) - Median 46 vs 49 mo; HR 1.05 (95% CI 0.83-1.31); 5-year OS ~45% in both arms - no survival benefit from adding chemoradiation.
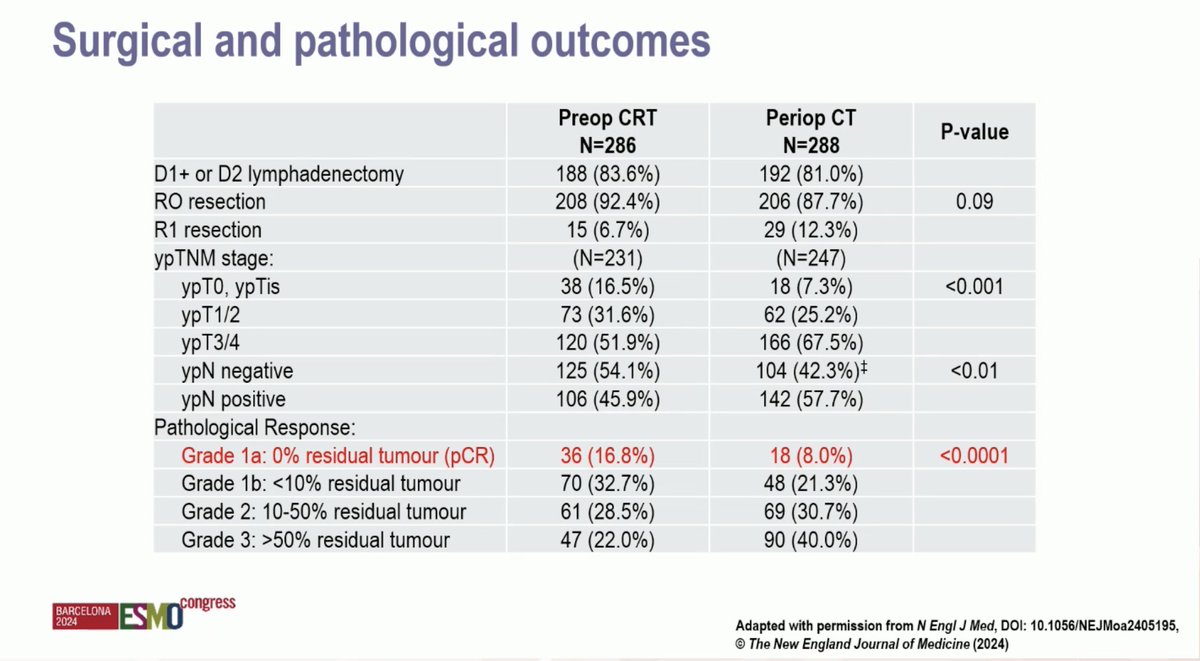
pCR - Improved with chemoradiation (17% vs 8%) but did not translate into an OS benefit.
Safety - Both arms well tolerated; chemoradiation did not increase treatment-related toxicity or surgical risk (compliance 95% RT, 91% chemo; R0 92% both arms).
Regulatory - Investigational/academic - no FDA approval implication; consolidates perioperative chemotherapy (e.g., FLOT) as standard, without routine preoperative chemoradiation.
Sponsor - AGITG with EORTC, TROG, CCTG intergroup.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.





Top tweets by impressions — click to view on X
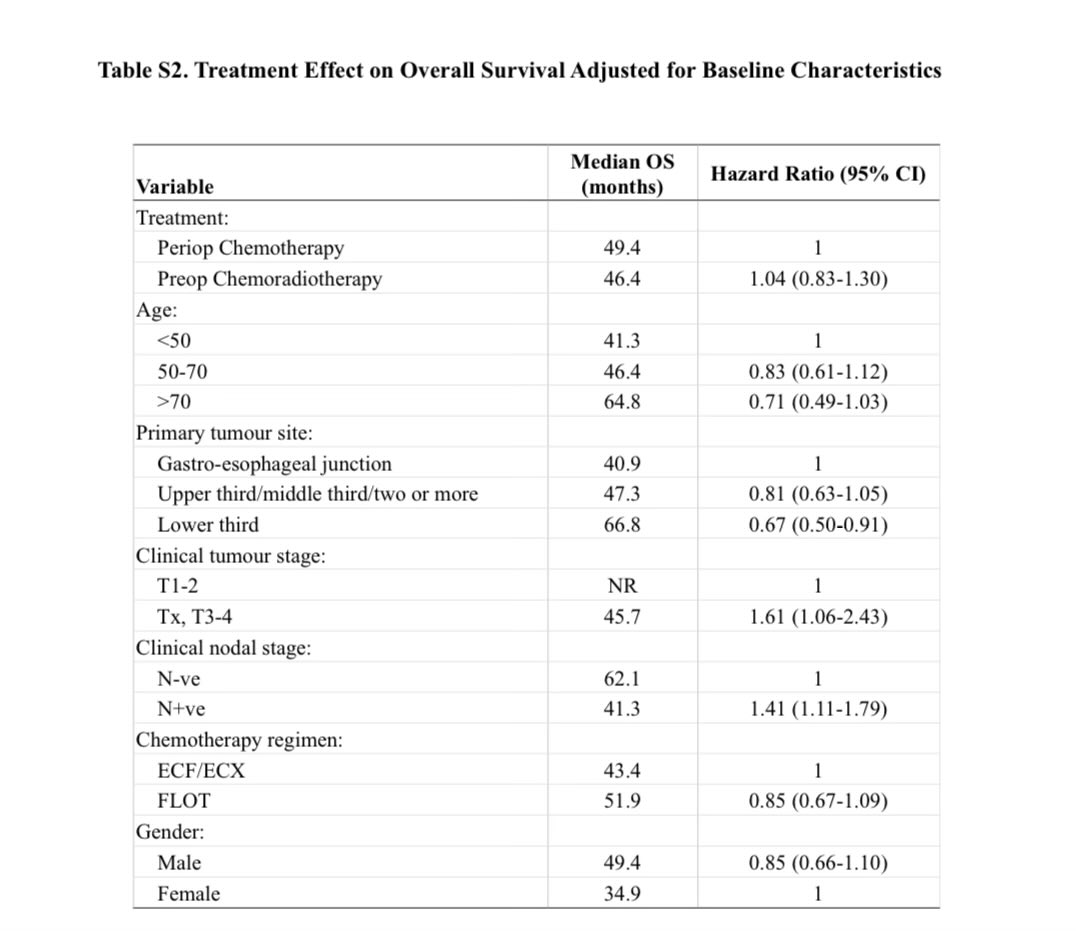
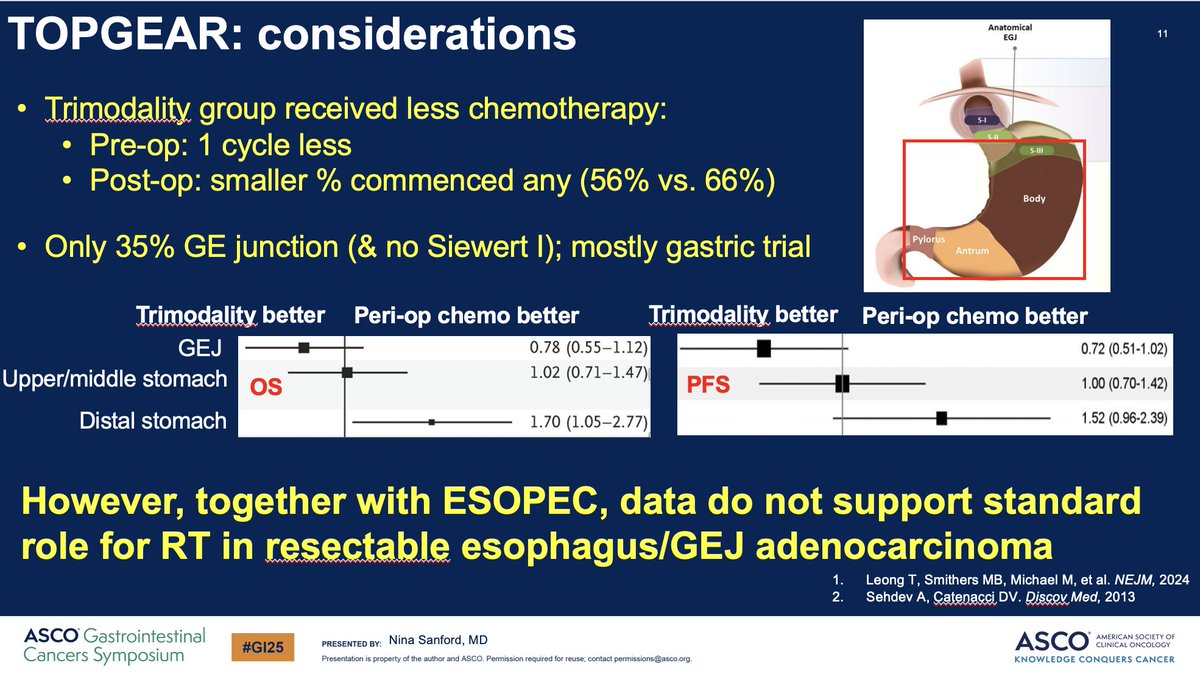
Yes, I made a similar pt in my talk re: TOPGEAR. Differences in treatment effect by primary tumor location. https://t.co/oJOCCH4vzf https://t.co/8cICuiK0aO
@RyanMorseKU @nbn426 @KristenCiombor @NiuSanford The fascinating thing from TOPGEAR = primary tumor site location. Gastric benefits more from chemo, w/important treatment x primary tumor site…
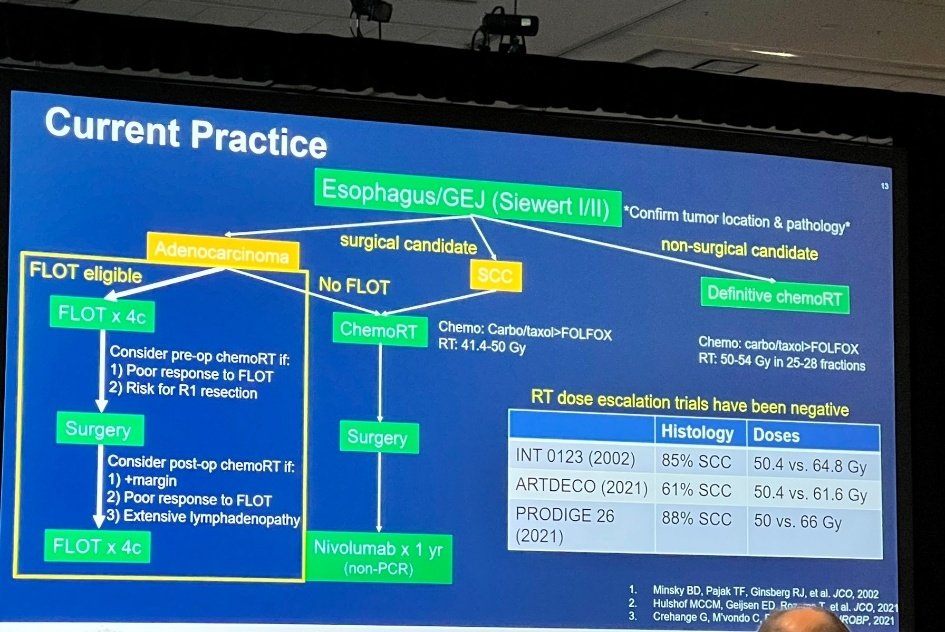
What an amazing session by @NiuSanford and Dr. Sanjay Wani! #GI25 Great discussion on ESOPEC, TOPGEAR and other trials and breakdown of current practice guidelines! Insightful @AnwaarSaeed3…
Trevor Leong, MBBS, MD, FRANZCR, discusses findings from the TOPGEAR trial assessing perioperative chemoradiotherapy in gastric/GEJ cancer. @PeterMacCC @myESMO #ESMO24 #oncology…
7/10 – TOPGEAR #ESOsm #STCsm
Phase 3 - periop CTx with or without preop CRT for resectable gastric cancer
#ESMO24 @myESMO @NEJM @GICancer @CDNCancerTrials
N= 574 pts
👉 33% FLOT
👉pCR 167vs 78%
👉PFS…
TOPGEAR is the definitive Phase 3 answer to whether preoperative chemoradiation improves outcomes over perioperative chemotherapy alone in resectable gastric/GEJ adenocarcinoma. Despite more than doubling pCR (17% vs. 8%) and more tumor/node downstaging, the addition of 45 Gy preoperative CRT did NOT improve OS (46 vs. 49 months) or PFS (31 vs. 32 months). Along with ESOPEC (FLOT > CROSS in esophageal adenocarcinoma), TOPGEAR consolidates perioperative chemotherapy (FLOT) as SOC globally. Role of radiation in this setting is retreating; future direction focuses on improving systemic regimens with immunotherapy (MATTERHORN perioperative durvalumab + FLOT) and targeted agents.
Median: 46 months (preop CRT + perioperative chemo (Arm B)) vs. 49 months (perioperative chemo alone (Arm A, ECF or FLOT)). HR 1.05 (95% CI 0.83-1.31) 5-year OS rate rate: 45% (CRT + chemo) vs. 45% (chemo alone). Phase 3 intergroup trial enrolled N=574 (Arm A chemo alone 288, Arm B CRT + chemo 286). Tumor location: 35% at GEJ; Stage: 88% T3, 60% node-positive. Median follow-up 67 months. Median OS 46 months (CRT) vs. 49 months (chemo alone) — HR 1.05 (95% CI 0.83-1.31) — NOT significantly different. 5-year OS ~45% in both groups. Median PFS 31 vs. 32 months. Primary endpoint NOT MET. Leong et al., NEJM 2024.
HR 1.05 (95% CI 0.83-1.31) OS was the primary endpoint (see above). Despite pCR improvement with CRT (17% vs. 8%), no OS difference. Investigators concluded preoperative CRT should NOT become routine SOC. Consolidates perioperative chemotherapy (FLOT, per ESOPEC for esophageal; FLOT4 for gastric) as SOC.
Both arms well-tolerated and feasible. Addition of CRT did not increase treatment-related toxicity or surgical risks. Compliance 95% RT, 91% chemo. Surgery performed 84% (CRT) vs. 89% (chemo alone). R0 resection 92% in both. pCR 17% vs. 8% (significantly better with CRT) but no OS translation. Toxicity: similar across groups, no major increase in surgical or GI/hematologic toxicities.
❌ Negative Phase 3: Preoperative CRT adds no OS benefit to perioperative chemo in resectable gastric/GEJ cancer. TOPGEAR is the definitive Phase 3 answer to whether preoperative chemoradiation improves outcomes over perioperative chemotherapy alone in resectable gastric/GEJ adenocarcinoma. Despite more than doubling pCR (17% vs. 8%) and more tumor/node downstaging, the addition of 45 Gy preoperative CRT did NOT improve OS (46 vs. 49 months) or PFS (31 vs. 32 months). Along with ESOPEC (FLOT > CROSS in esophageal adenocarcinoma), TOPGEAR consolidates perioperative chemotherapy (FLOT) as SOC globally. Role of radiation in this setting is retreating; future direction focuses on improving systemic regimens with immunotherapy (MATTERHORN perioperative durvalumab + FLOT) and targeted agents.
TOPGEAR (EORTC-22114-40111-GITCG-ROG) is a Phase 3 intergroup randomized trial (NCT01924819) that tested whether adding preoperative chemoradiotherapy to perioperative chemotherapy improves outcomes in resectable gastric or gastroesophageal junction adenocarcinoma. Arm B received preoperative chemoradiation plus perioperative chemotherapy, and Arm A received perioperative chemotherapy alone (ECF or FLOT), with overall survival as the primary endpoint.
No. TOPGEAR was a negative trial. Median overall survival was 46 months with preoperative chemoradiation plus chemotherapy versus 49 months with chemotherapy alone (HR 1.05; 95% CI 0.83-1.31), and 5-year overall survival was about 45% in both arms - no survival benefit from adding chemoradiation.
Preoperative chemoradiation did significantly increase the pathologic complete response rate (17% versus 8%), but this did not translate into longer overall survival. The investigators concluded that preoperative chemoradiotherapy should not become routine standard of care in resectable gastric/GEJ cancer.
TOPGEAR consolidates perioperative chemotherapy (such as FLOT) as the standard for resectable gastric/GEJ adenocarcinoma and argues against routinely adding preoperative chemoradiation. There is no drug approval involved; this is a treatment-strategy comparison that informs multidisciplinary practice.
Yes. Both arms were well tolerated and feasible. Adding chemoradiation did not increase treatment-related toxicity or surgical risk; compliance was 95% for radiotherapy and 91% for chemotherapy, surgery was performed in the large majority of patients, and R0 resection was achieved in 92% of both arms.