EGFR-mutated advanced NSCLC with concurrent TP53 mutations — AstraZeneca
Discover KOL Sentiment on TOP Study →Design - Phase 3 multicentre randomized investigator-initiated trial of osimertinib (Tagrisso) + chemotherapy vs osimertinib monotherapy in EGFR-mutant advanced NSCLC with a concurrent TP53 mutation (NCT04695925; Sun Yat-sen University Cancer Center, PI Li Zhang; AstraZeneca drug supply).
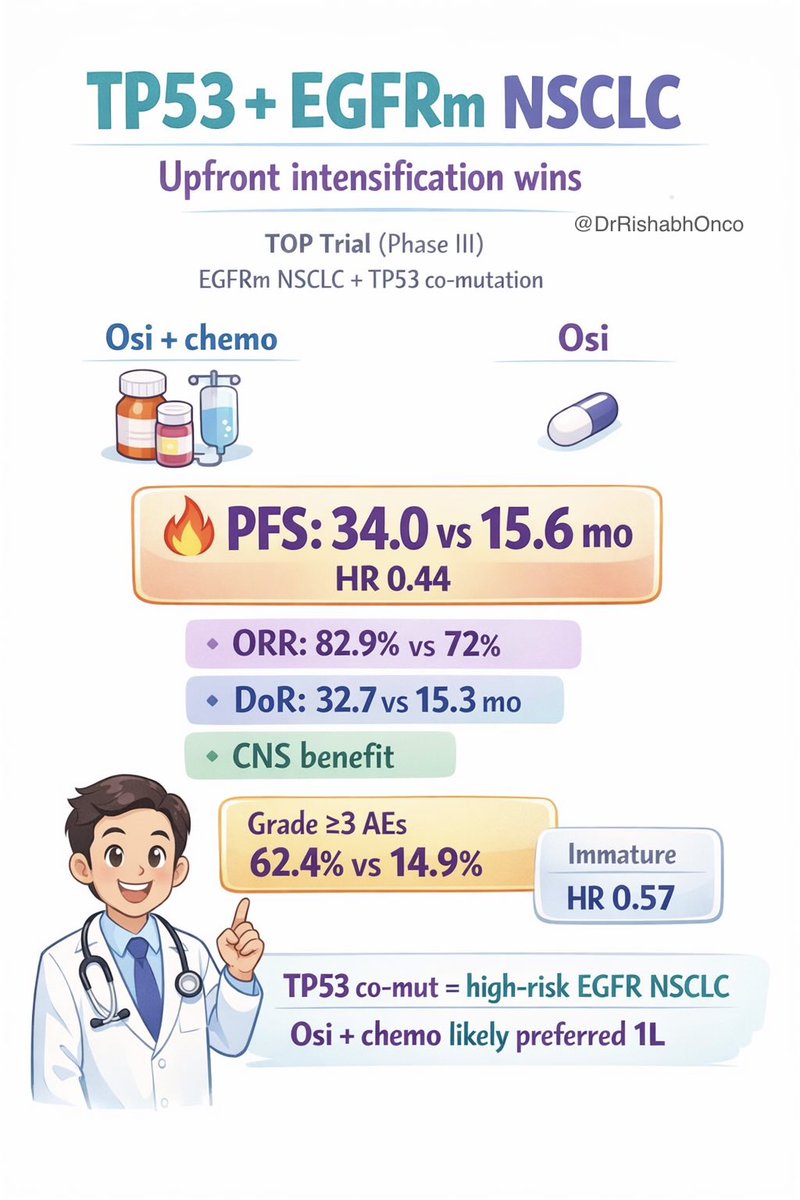
PFS (primary) - Median PFS 34.0 months (95% CI 24.9-36.4) with osimertinib + chemotherapy vs 15.6 months (95% CI 13.0-18.3) with osimertinib monotherapy - a statistically significant improvement.
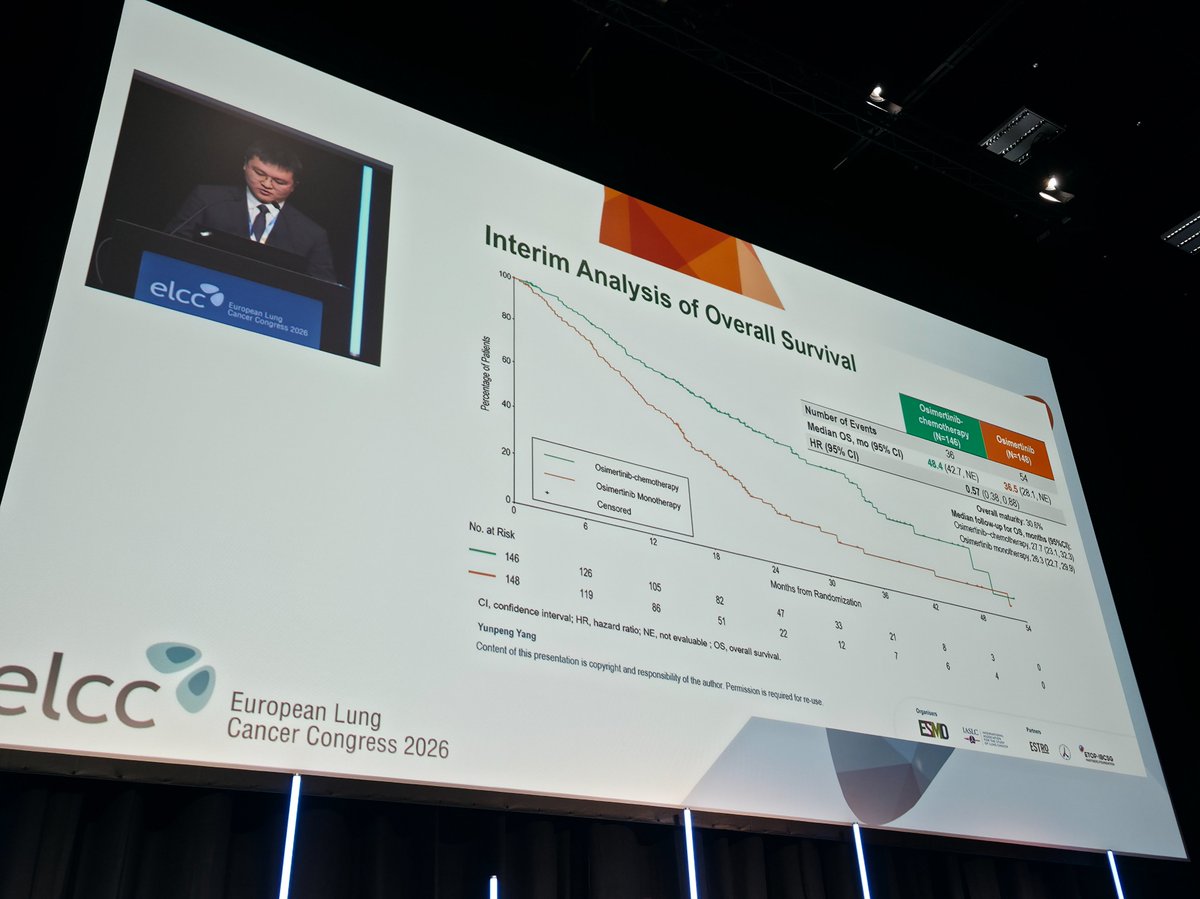
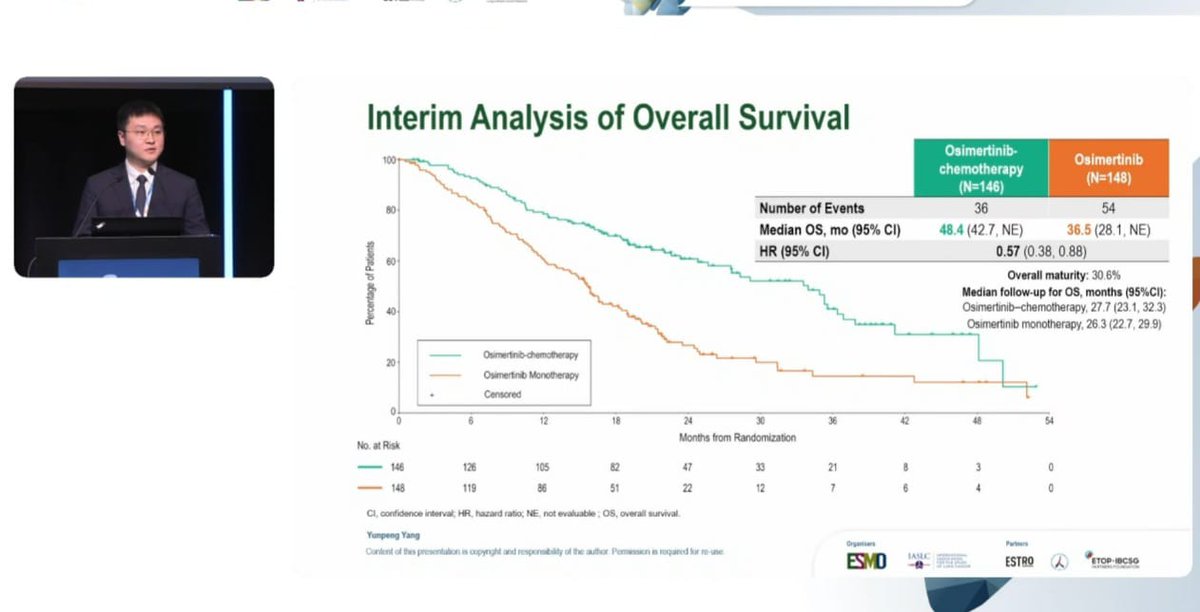
Overall survival (interim) - Immature (30.6% maturity); encouraging trend favoring the combination (median OS 48.4 vs 36.5 months, HR 0.57, 95% CI 0.38-0.88); formal OS testing pending.
Safety - Consistent with FLAURA2, with no new safety signals; the combination carried higher toxicity than monotherapy, as expected when adding chemotherapy.
Regulatory / sponsor - Investigational TP53-guided strategy; osimertinib (Tagrisso) approved in EGFR-mutant NSCLC and osimertinib + chemotherapy approved 1L broadly (FLAURA2). Sponsor Sun Yat-sen University Cancer Center; AstraZeneca drug supply. Presented at ELCC 2026.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.








Top 10 by impressions — click to view on X
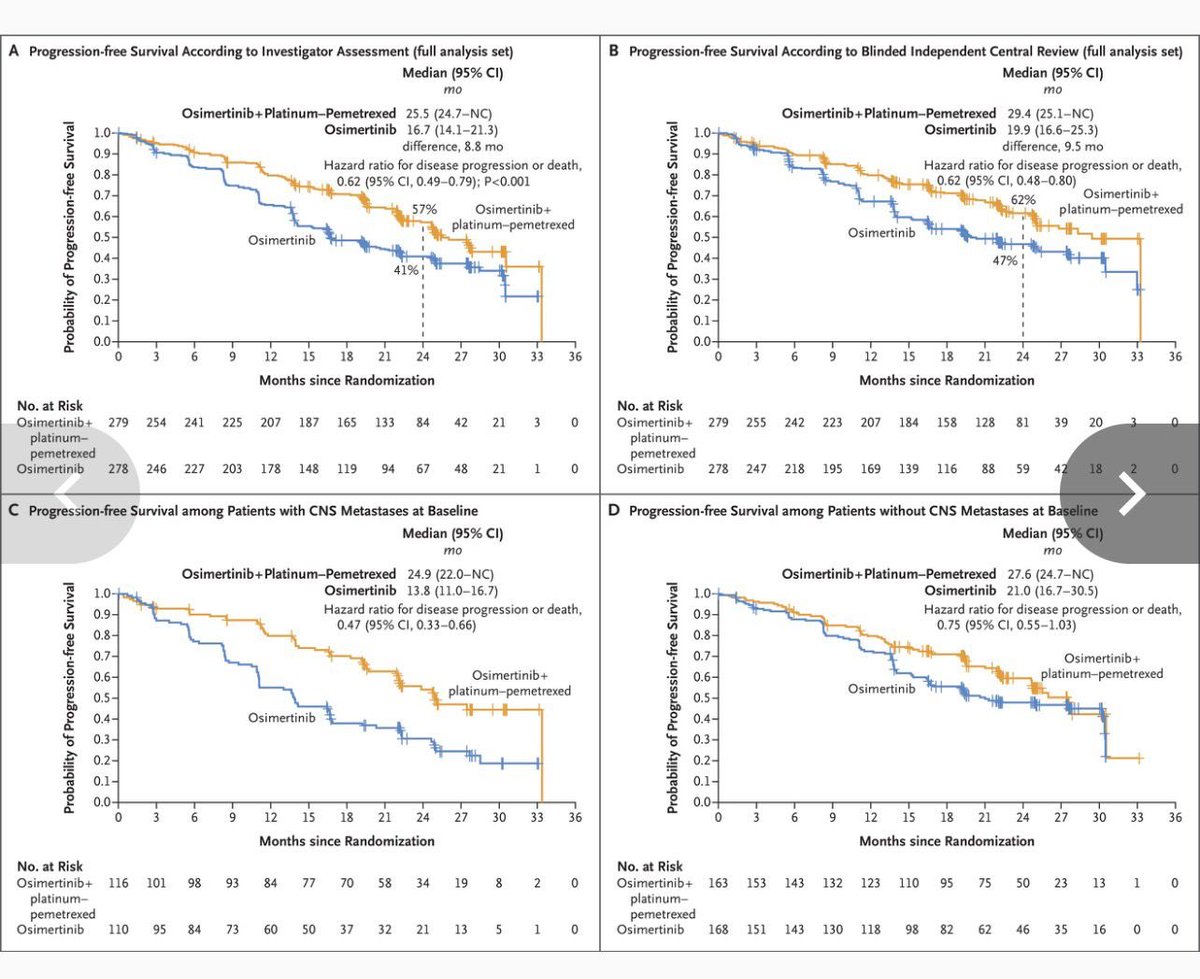
Important study tackling a highly relevant question in #EGFRm #NSCLC. One observation: the PFS and OS curves look visually identical, even though the reported medians differ—perhaps suggesting an inadvertent duplication of the PFS KM figure.
TP53 + EGFRm NSCLC - upfront intensification wins #ELCC26 TOP Trial (Phase III) Osi +/- chemo in EGFRm + TP53 co-mutation. PFS: 34.0 vs 15.6 mo (HR 0.44, p<0.001) ORR: 82.9% vs 72.0% DoR: 32.7 vs 15.3 mo
What's going on with these KM plots from lung cancer trials?!
The PFS and OS curves for a similar trial FLAURA-2 were okay. How did this new trial have such an unbelievably smooth curve for the same intervention?
Not all EGFR NSCLC is the same... TP53 co-mutation changes the game #ELCC26 Phase 3 TOP trial EGFR + TP53 mutated advanced NSCLC. PFS: 34.0 vs 15.6 mo HR 0.44. OS (immature):
#ELCC26 @myESMO Proffered Paper session 1 TOP study: Osimertinib +/- Chemo in EGFRm + TP53 mutation PFS HR 0.44 (95%CI 0.32-0.61), ORR 82.9% vs. 72.0% Dr. Yunpeng Yang NCT04695925
Osimertinib plus Chemo is way forward in metastatic NSCLC With P53 mutation. Expected results. @RManochakian @Alfdoc2 @DrewMoghanaki @myESMO @FordePatrick #elcc2026

TOP trial shows benefit of osi+chemio in EGFR mut/P53 mut NSCLC with early separation of OS curve (not occurring in Flaura2). P53 mut could be DISRUPTIVE and non-DISRUPTIVE which are functionally different categories. #ELCC2026

#ELCC26 proffered paper session 1 with results of the TOP trial: chemo+osi compared to osi alone in #EGFRmut #NSCLC with #TP53 mutations: Impressive doubling of PFS, points to consider:

TOP: first prospective phase III trial showing osi plus CTx significantly prolongs PFS vs. osi monotherapy in advanced EGFRm NSCLC with TP53 co-mutations. PFS 34 m. vs 15.6 m. #ELCC2026 @OncoAlert
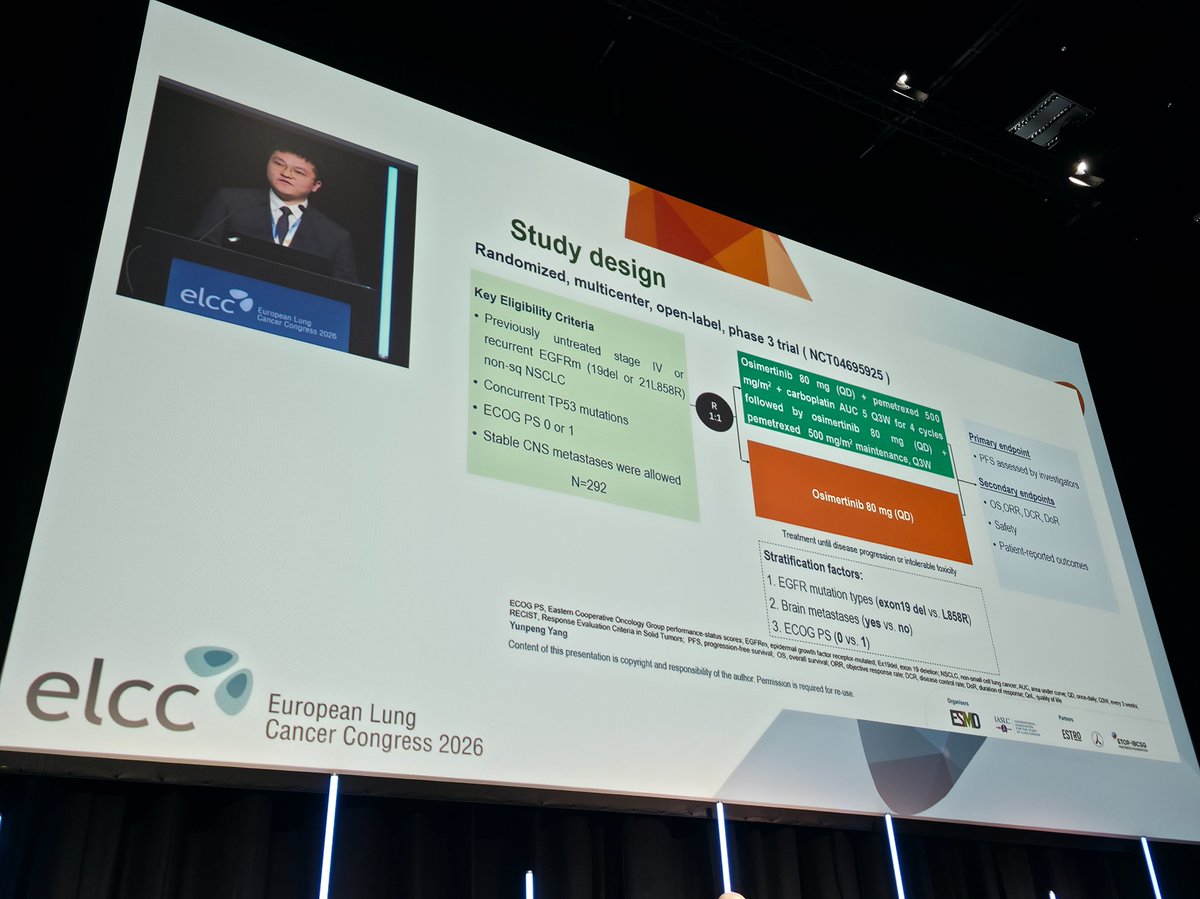
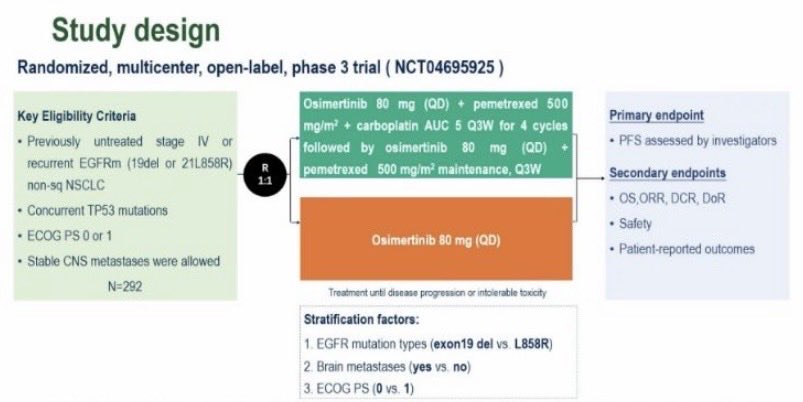
The TOP Study is a randomized, multicenter, open-label, phase 3 trial (NCT04695925) evaluating osimertinib plus chemotherapy versus osimertinib monotherapy in previously untreated patients with EGFR-mutated advanced NSCLC harboring concurrent TP53 mutations. Presented at ELCC 2026, the study enrolled 294 patients and demonstrated that adding chemotherapy to osimertinib significantly improved progression-free survival. This is the first prospective phase III trial to address the question of treatment intensification in this molecularly defined high-risk subgroup.
Randomized 1:1, multicenter, open-label, phase 3 trial. Osimertinib 80 mg daily plus pemetrexed/carboplatin for 4 cycles followed by osimertinib plus pemetrexed maintenance versus osimertinib 80 mg daily monotherapy.
Previously untreated stage IV or recurrent EGFR-mutated (exon 19 deletion or L858R) non-squamous NSCLC with concurrent TP53 mutations. ECOG PS 0-1; stable CNS metastases allowed. N=294 (146 combo, 148 mono).
Experimental: osimertinib 80 mg QD + pemetrexed 500 mg/m2 + carboplatin AUC 5 Q3W for 4 cycles, then osimertinib + pemetrexed maintenance. Control: osimertinib 80 mg QD monotherapy. Stratified by EGFR mutation type, brain metastases, and ECOG PS.
Primary endpoint: investigator-assessed PFS. Secondary endpoints: OS, ORR, DCR, DoR, safety, and patient-reported outcomes.
Osimertinib plus chemotherapy demonstrated a statistically significant improvement in PFS compared to osimertinib monotherapy, with a median PFS of 34.0 months (95% CI: 24.9-36.4) versus 15.6 months (95% CI: 13.0-18.3). The stratified hazard ratio was 0.44 (95% CI: 0.32-0.60; P<0.001), representing an improvement of approximately 18.4 months. PFS benefit was consistent across all prespecified subgroups.
OS data was immature at this interim analysis (30.6% maturity). There was an encouraging trend favoring the combination arm with median OS of 48.4 months versus 36.5 months (HR 0.57; 95% CI: 0.38-0.88). Formal statistical testing of OS was not performed at this interim timepoint.
The safety profile of osimertinib plus chemotherapy was consistent with that reported in the FLAURA2 study, with no new safety signals identified. The combination was associated with higher toxicity compared to monotherapy, as expected with the addition of chemotherapy. Detailed adverse event data were presented alongside the efficacy results.
These findings provide key evidence supporting a molecular risk-guided, individualized treatment strategy for EGFR-mutated advanced NSCLC. Notably, the FLAURA2 trial (osimertinib + chemotherapy in the broader 1L EGFRm population) has received FDA approval, but that indication does not specifically address TP53 co-mutated patients. The TOP study is the first prospective trial to demonstrate that TP53 co-mutation identifies a poor-prognostic subgroup that derives particular benefit from the osimertinib-chemotherapy combination (HR 0.44 vs FLAURA2's HR 0.62 in the unselected population). While the FLAURA2 approval provides a regulatory pathway for this combination, the TOP data suggest TP53 testing may help guide treatment intensification decisions within that approved framework. However, the duplicate KM figure controversy at ELCC 2026 underscores the need for corrected data and peer-reviewed publication before drawing definitive conclusions.
The TOP Study (NCT04695925) is a Phase 3, investigator-initiated randomized trial from Sun Yat-sen University Cancer Center (principal investigator Li Zhang, with AstraZeneca supplying drug) comparing osimertinib (Tagrisso) plus chemotherapy against osimertinib monotherapy in patients with EGFR-mutant advanced non-small cell lung cancer who also have a concurrent TP53 mutation - a subgroup with historically worse outcomes.
Adding chemotherapy to osimertinib significantly improved progression-free survival, with a median of 34.0 months versus 15.6 months for osimertinib alone. Overall survival was immature at interim analysis (30.6% maturity) but showed an encouraging trend favoring the combination (median 48.4 versus 36.5 months, hazard ratio 0.57), with formal statistical testing pending further follow-up.
Osimertinib (Tagrisso) is FDA-approved in EGFR-mutant NSCLC, and osimertinib plus chemotherapy is approved more broadly in the first-line EGFR-mutant setting based on the FLAURA2 trial. The TOP Study specifically evaluates a TP53-co-mutation-guided strategy; that biomarker-selected use is investigational and is the focus of this trial.
The safety profile of osimertinib plus chemotherapy was consistent with that reported in FLAURA2, with no new safety signals identified. As expected, adding chemotherapy increased toxicity compared with osimertinib monotherapy, so the improved efficacy must be weighed against greater treatment burden.
Concurrent TP53 mutations mark a poor-prognosis subgroup within EGFR-mutant NSCLC, and the TOP Study supports a molecular risk-guided, individualized first-line strategy: intensifying treatment with osimertinib plus chemotherapy for TP53-co-mutant patients who are most likely to benefit, while potentially sparing lower-risk patients the added toxicity.