ADAURA is a Phase 3, double-blind trial of adjuvant osimertinib (Tagrisso) versus placebo after complete resection of stage IB-IIIA EGFR-mutant NSCLC. Osimertinib reduced disease recurrence or death by 83% (stage II-IIIA DFS HR 0.17) and improved overall survival (OS HR 0.49), supporting FDA approval on December 18, 2020. Sponsor: AstraZeneca.
Discover KOL Sentiment on ADAURA →Design — Phase 3, double-blind, placebo-controlled; adjuvant osimertinib 80 mg vs placebo up to 3 yr, resected stage IB-IIIA EGFR-mutant NSCLC, n=682 (NCT02511106). (NEJM)
DFS (primary) — Stage II-IIIA DFS HR 0.17 (99.06% CI 0.11-0.26; p<0.001) — 83% reduction in recurrence or death. (NEJM)
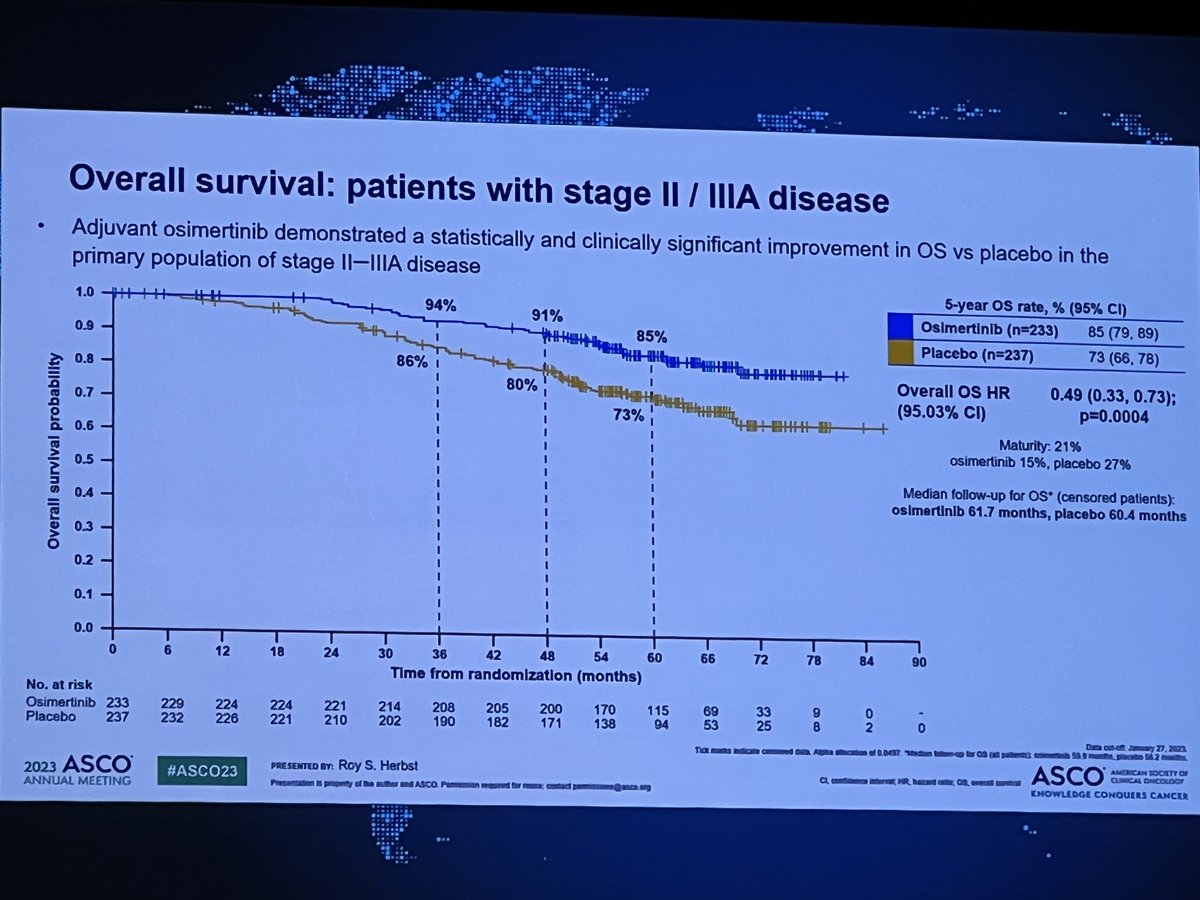
Overall survival — Final OS (stage II-IIIA) HR 0.49 (95.03% CI 0.33-0.73; p=0.0004); 5-year OS 85% vs 73%. (NEJM 2023)
Safety — Consistent with known osimertinib profile: diarrhea 46% vs 20%, paronychia 25% vs 1%; Grade 3+ AEs 20% vs 13%. (NEJM)
Regulatory — FDA approved December 18, 2020 (Project Orbis, breakthrough designation); first targeted adjuvant therapy in NSCLC. (FDA.gov)
Sponsor / Drug — AstraZeneca; osimertinib (Tagrisso), a 3rd-generation EGFR TKI. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.









Top 10 by impressions - click to view on X
Here is the REAL @Plenary_Session on #ADAURA #ASCO23 #ASCO2023 38.5% of people who had recurrence got OSI (very low!) That just...
Hey @JackWestMD, did you already see p25 of the #ADAURA supplementary appendix? Curious of your thoughts given 88% of pts in the placebo arm who developed progression and...
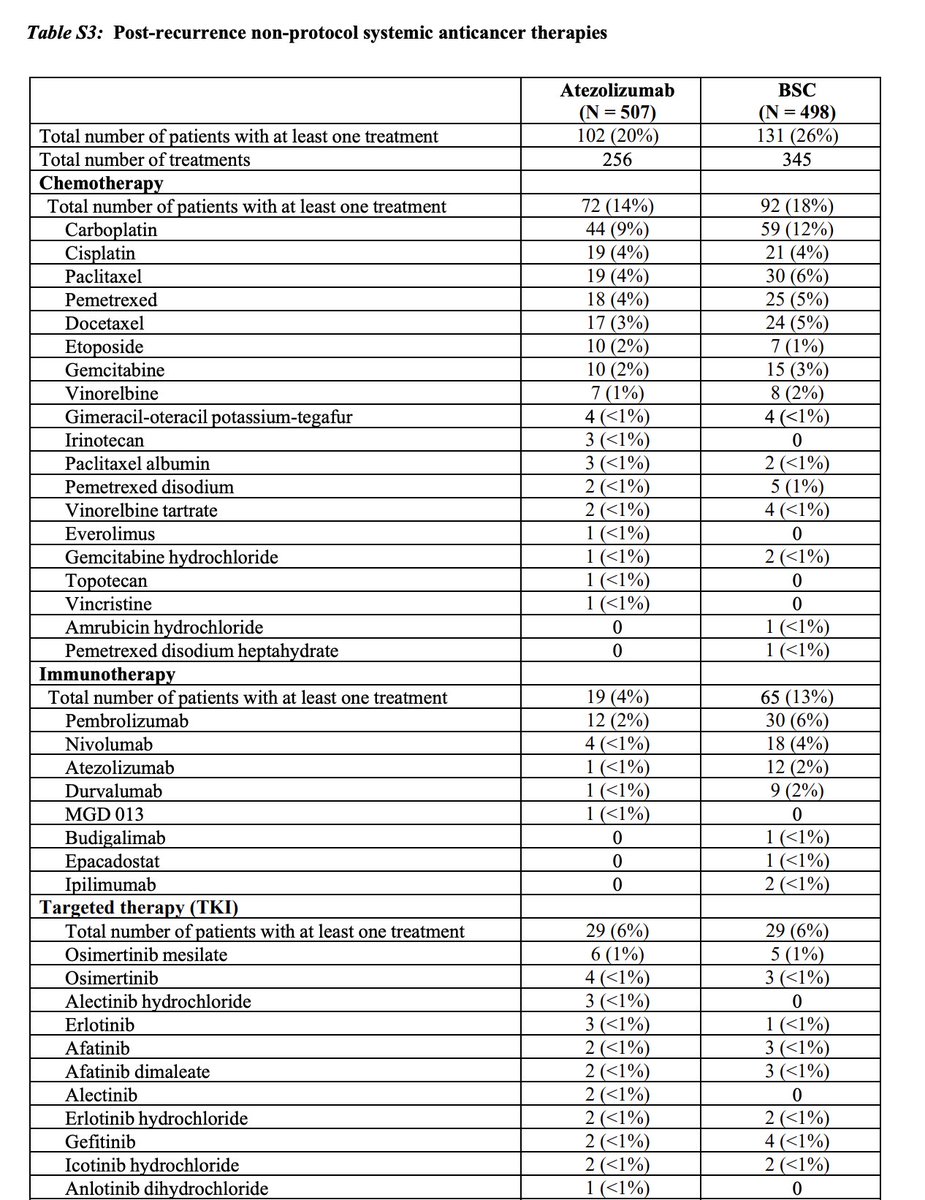
Before we all continue to pile on #ADAURA, can someone tell me % of patients who received Immunotherapy upon progression on IM-010 or KN-91. See figure. I will remind you that...
My analysis of ADAURA now on youtube in high resolution #ASCO23 ADAURA OS - Control arm participants who progressed got poor medical car... via @YouTube
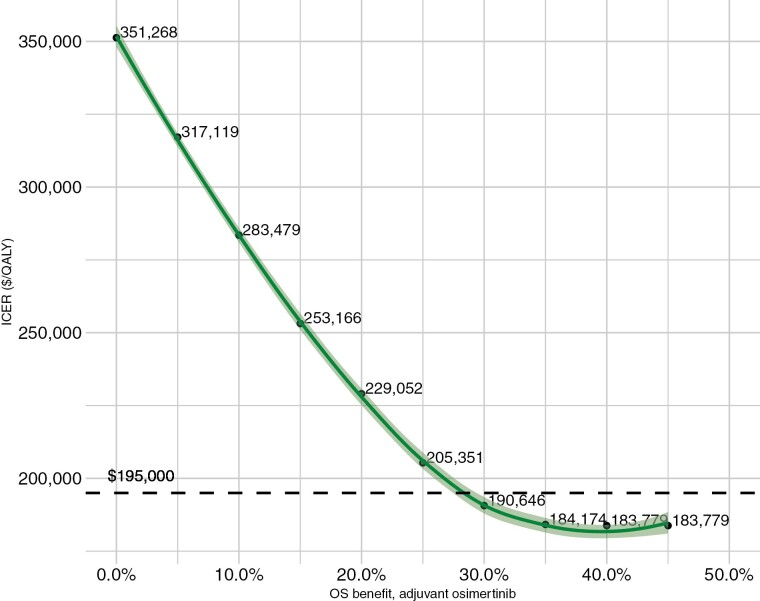
Please check out this cost effectiveness analysis done by @LemmonOnc and I based on various projected final ADAURA OS results. We calculated that adjuvant osimertinib would be cost effective...

So only 79 of 343 patients (23%) in placebo arm got subsequent osimertinib in #ADAURA. Would love to see OS results subgrouped by those who got subsequent osi versus those who did...
"I have to start with #ADAURA because the Cheerleaders are out there in full force." Bring the truth, VP! Oncology has too many Cheerleaders. Put down the pom-poms and...
The average wholesale price of Osimertinib: $440,000. Shouldn't we ensure this OS benefit is real by running a trial with an appropriate control arm before bankrupting...
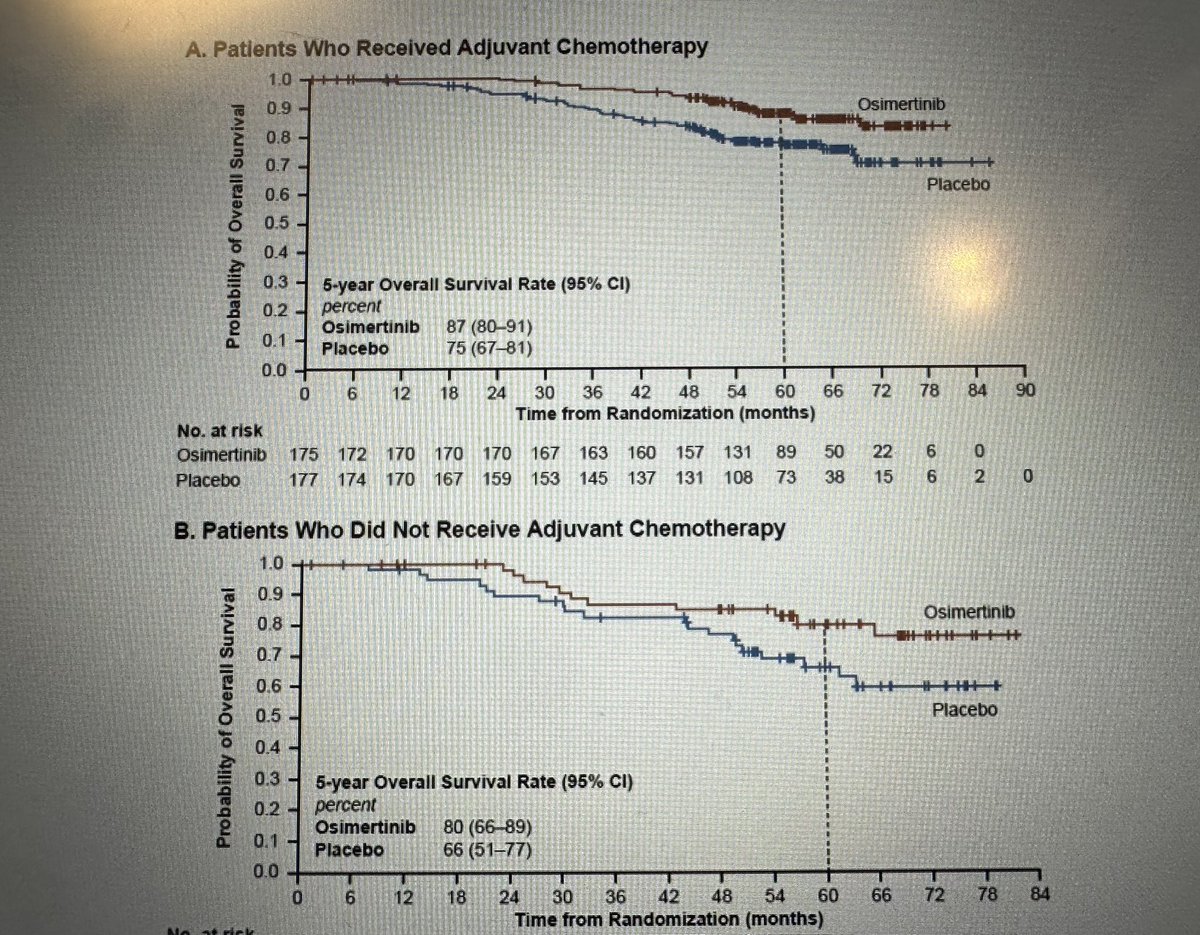
ADAURA; look at NEJM supplementary ; 7% 5y landmark advantage for those who got adjuvant chemo. My view will be to recommend adjuvant chemo before adjuvant osimertinib #ASCO23...
Thanks to @VivekSubbiah for giving @JackWestMD and I a chance to channel our debates into surprising consensus! #LCSM Lessons from ADAURA: Can we improve on a...
ADAURA is a landmark Phase III, double-blind, placebo-controlled trial that established adjuvant osimertinib (Tagrisso) as the standard of care for patients with completely resected stage IB-IIIA EGFR-mutant non-small cell lung cancer. The trial randomized 682 patients across 26 countries to receive osimertinib 80 mg daily or placebo for up to 3 years following surgery, with or without prior adjuvant chemotherapy. ADAURA is the first trial to demonstrate that a targeted EGFR therapy in the adjuvant setting translates a disease-free survival benefit into a statistically significant overall survival benefit.
Phase III, international, double-blind, 1:1 randomized, placebo-controlled trial in patients with completely resected stage IB-IIIA EGFR-mutant (exon 19 deletion or L858R) non-squamous NSCLC. EGFR mutations were identified prospectively using the cobas EGFR Mutation Test. Adjuvant chemotherapy was permitted but not mandated.
Adults with completely resected stage IB-IIIA (AJCC 7th edition) NSCLC harboring EGFR exon 19 deletions or L858R mutations, with WHO performance status 0-1. Approximately 60% of patients received adjuvant chemotherapy prior to randomization. Stratified by disease stage, mutation type, and race.
Osimertinib 80 mg orally once daily versus placebo for up to 3 years or until disease recurrence or unacceptable toxicity.
Primary endpoint: investigator-assessed disease-free survival (DFS) in patients with stage II-IIIA disease. Key secondary endpoints: DFS in the overall population (stage IB-IIIA), overall survival (OS), health-related quality of life, and safety. CNS DFS was a prespecified exploratory endpoint.
Osimertinib demonstrated a profound DFS benefit versus placebo. In the primary population (stage II-IIIA), DFS HR was 0.17 (99.06% CI: 0.11-0.26; p<0.001), representing an 83% reduction in the risk of recurrence or death. Median DFS was not reached with osimertinib versus 19.6 months with placebo. Updated analysis at 4 years showed sustained benefit with DFS HR of 0.23 (95% CI: 0.18-0.30). CNS DFS HR was 0.24 (95% CI: 0.14-0.42), demonstrating significant protection against brain metastases.
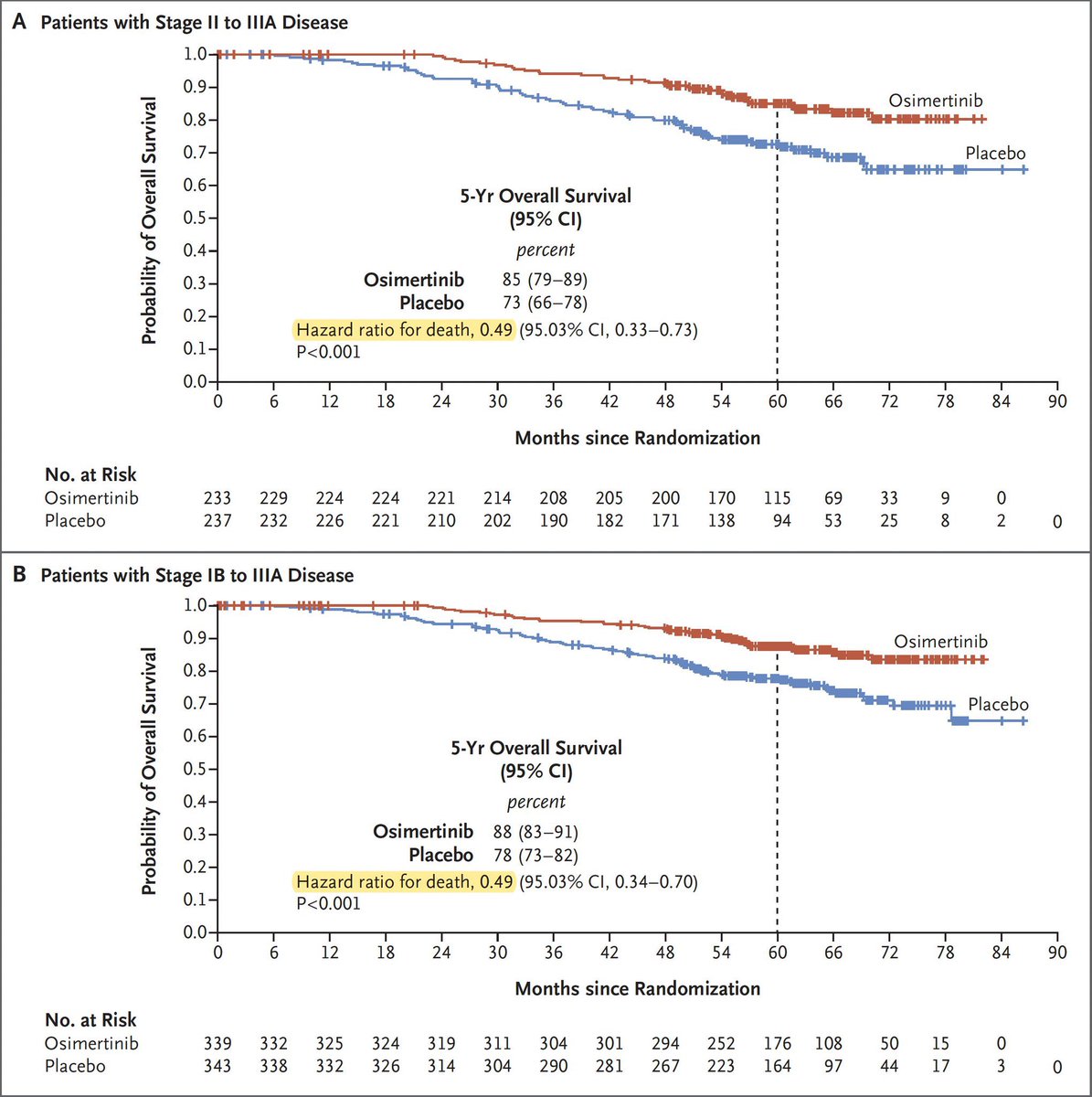
The planned final OS analysis demonstrated a statistically significant survival benefit. In stage II-IIIA patients, OS HR was 0.49 (95.03% CI: 0.33-0.73; p=0.0004), with 5-year OS rates of 85% versus 73%. In the overall population (stage IB-IIIA), OS HR was 0.49 (95.03% CI: 0.34-0.70; p<0.0001), with 5-year OS rates of 88% versus 78%. Osimertinib is the only EGFR TKI to demonstrate a significant OS benefit in the adjuvant setting.
The safety profile was consistent with known osimertinib toxicity. Most common adverse events were diarrhea (46% vs 20%), paronychia (25% vs 1%), and dry skin (23% vs 6%). Grade 3+ adverse events occurred in 20% of osimertinib patients versus 13% with placebo. Treatment discontinuation due to AEs was 11% versus 3%. No fatal AEs were reported with osimertinib. Extended follow-up showed no new safety signals, with grade 3+ AEs of 23% versus 14%.
ADAURA established adjuvant osimertinib as the standard of care for resected stage IB-IIIA EGFR-mutant NSCLC, with both DFS and OS benefits. The results underscore the importance of early EGFR mutation testing at diagnosis. Key clinical debates include the optimal treatment of stage IB patients, whether adjuvant chemotherapy adds benefit on top of osimertinib (subgroup analyses suggest it may not), the 3-year treatment duration question, and post-recurrence treatment strategies. ADAURA-2 (stage IA), NeoADAURA (neoadjuvant), and TARGET (5-year duration) are ongoing to address these questions.
ADAURA is a Phase 3, double-blind, placebo-controlled trial (NCT02511106) of adjuvant osimertinib (Tagrisso) versus placebo for up to 3 years in 682 patients with completely resected stage IB-IIIA EGFR exon 19 deletion or L858R non-small cell lung cancer.
Yes. On December 18, 2020 the FDA approved osimertinib (Tagrisso) for adjuvant therapy after tumor resection in patients with EGFR exon 19 deletion or exon 21 L858R-mutant NSCLC, as detected by an FDA-approved test. It was the first targeted therapy approved in the adjuvant NSCLC setting.
In the primary stage II-IIIA population, adjuvant osimertinib reduced the risk of disease recurrence or death by 83% (DFS HR 0.17; 99.06% CI 0.11-0.26; p<0.001) versus placebo. The benefit extended to the overall stage IB-IIIA population.
Yes. The final overall survival analysis showed a statistically significant benefit in stage II-IIIA patients (OS HR 0.49; 95.03% CI 0.33-0.73; p=0.0004), with 5-year OS rates of about 85% with osimertinib versus 73% with placebo.
Osimertinib (Tagrisso) is a third-generation EGFR tyrosine kinase inhibitor developed by AstraZeneca. In ADAURA it was given at 80 mg orally once daily for up to 3 years following complete surgical resection.



















































