Locally advanced or metastatic solid tumors (particularly EGFR-mutant NSCLC; also urothelial, NPC, HNSCC, SCLC) — Baili-Bio (Chengdu) Pharmaceutical / SystImmune, Inc.
Discover KOL Sentiment on BL-B01D1 →Design - First-in-class EGFRxHER3 bispecific ADC (iza-bren), multi-tumor Phase 1/2 development program (lead FIH NCT05983432; Phase 3 e.g. NCT06382116); featured data in EGFR-mutant NSCLC (ASCO 2023 / IASLC WCLC 2025).
Efficacy (EGFR-mutant NSCLC, IASLC 2025, n=50) - At 2.5 mg/kg D1D8 Q3W: ORR 66.0%, confirmed ORR 56.0%, median PFS 12.5 mo, median duration of response 13.7 mo.
OS - Median not reached in the EGFR-mutant NSCLC subgroup; 12-month OS rate 80.3%; broader multi-tumor OS immature.
Safety - Predominantly hematologic - grade >=3 neutropenia 34%, leukopenia 30%, thrombocytopenia 19%, anemia 15%; all-grade anemia ~91%; nausea, alopecia.
Regulatory - Investigational - not FDA approved for any indication; registrational Phase 3 studies ongoing (largely in China).
Sponsor / drug - SystImmune / Baili-Bio (Chengdu); BL-B01D1 (izalontamab brengitecan, iza-bren; also BMS-986507).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.














Top tweets by impressions — click to view on X
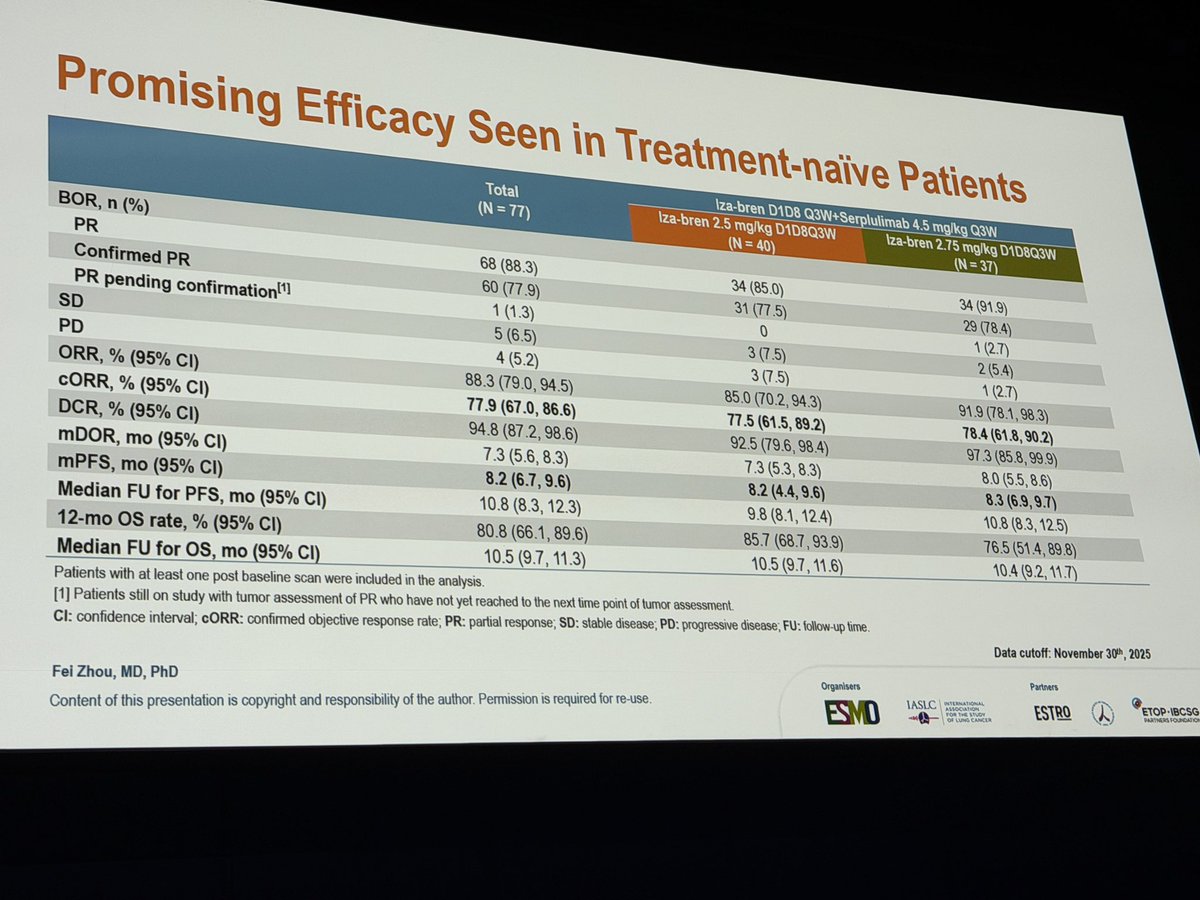
impressive data in #SCLC26 on IZA-BREN ( EGFRxHER3 ADC) with ICI surplulimab in 1L ES-SCLC:
➡️ ORR 85-92%! across IZABREN doses
➡️ mDOR =7-8 m
➡️ Discontinuation due to TRAEs only 7.3%
Dawn 🌅 of a…
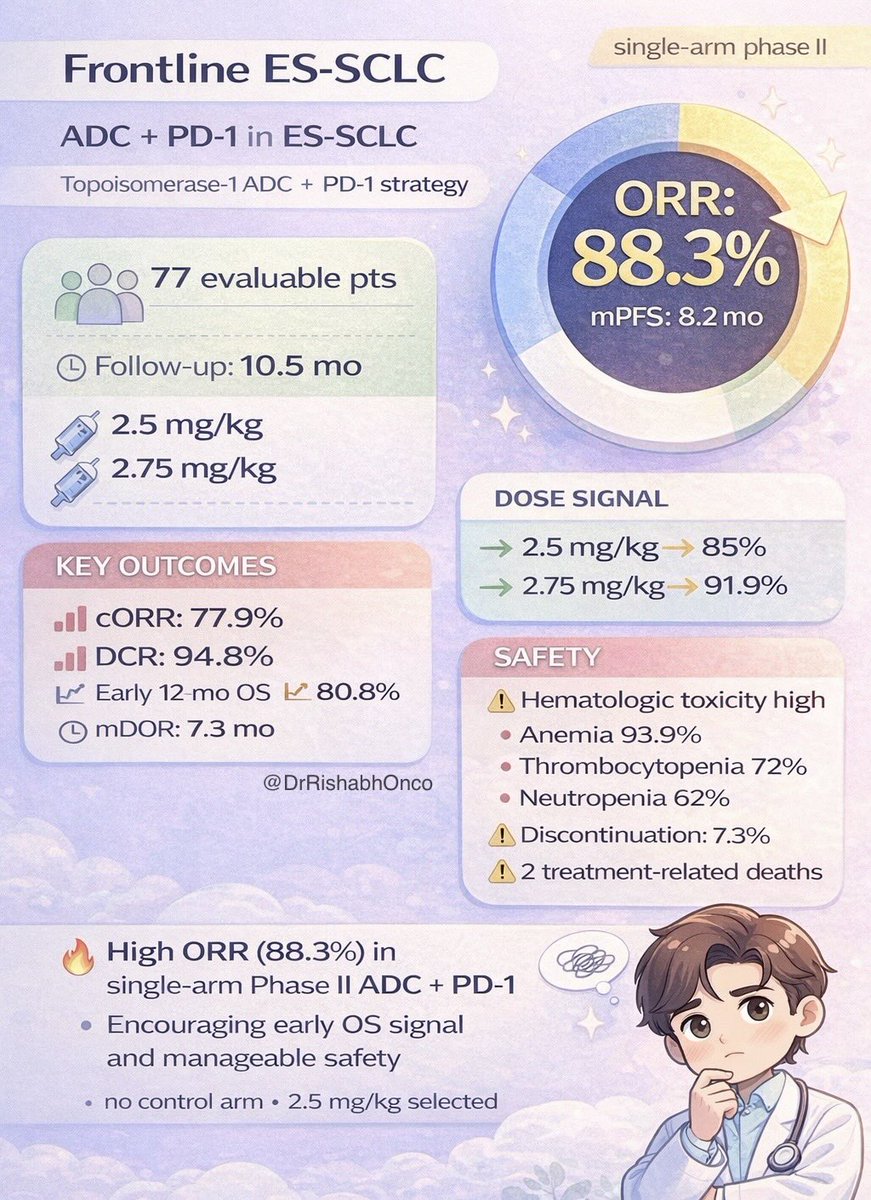
High ORR (88.3%) with a novel ADC + PD-1 combo in frontline ES-SCLC
#ELCC26
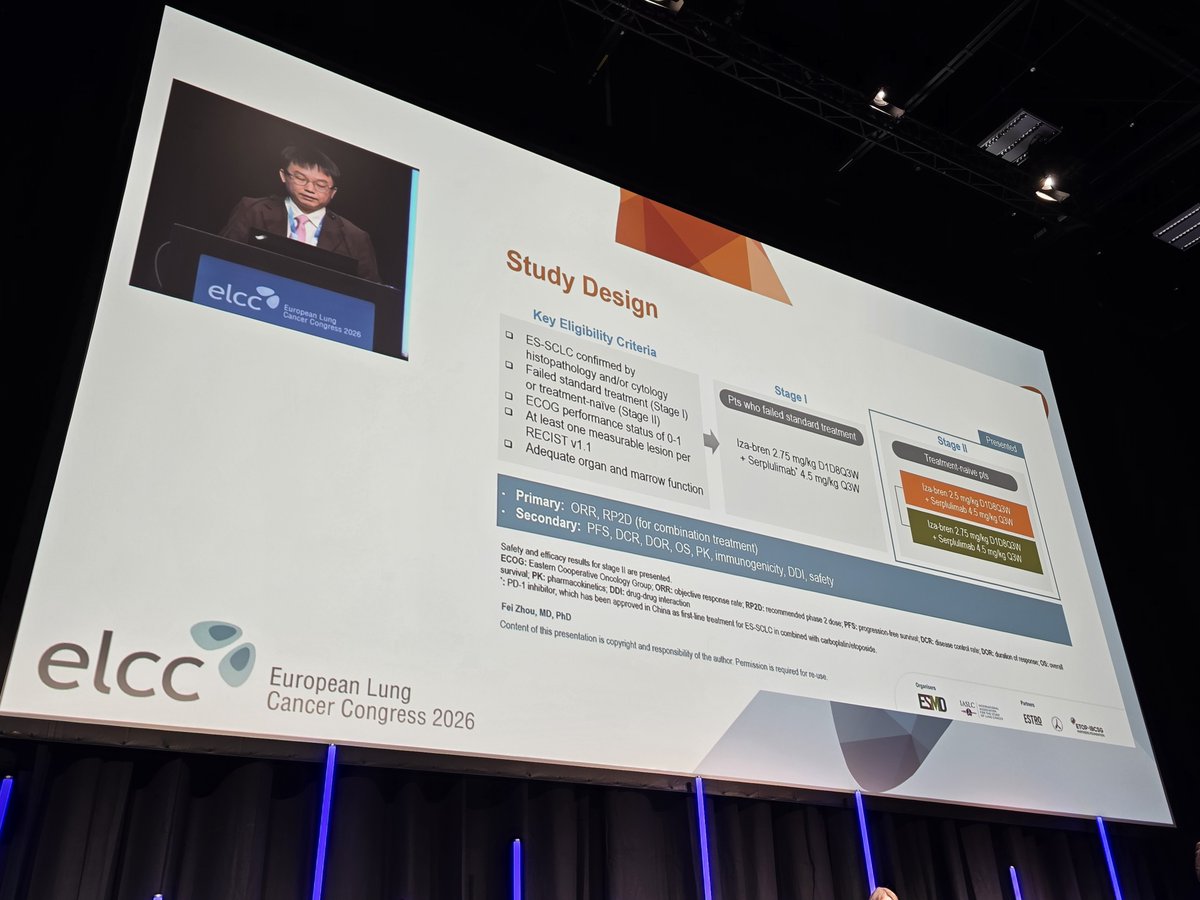
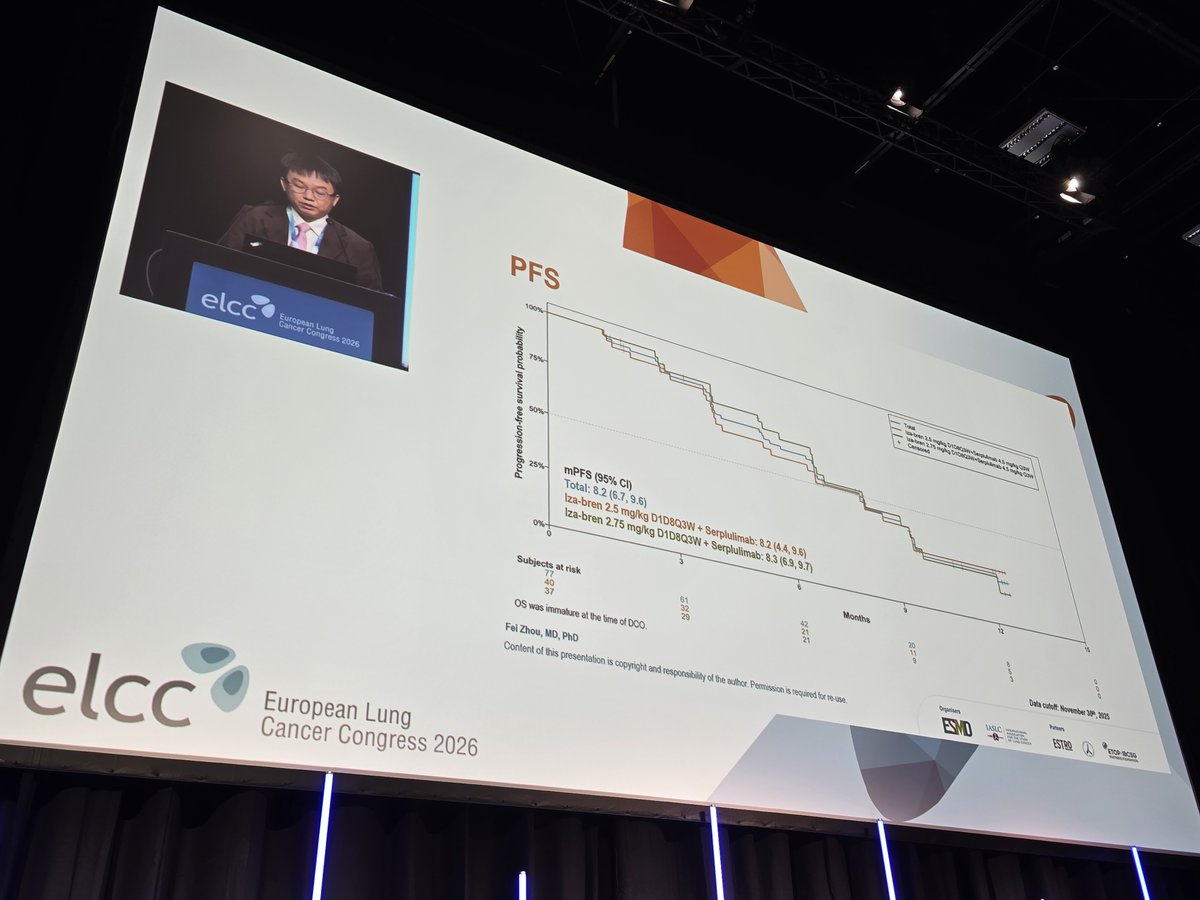
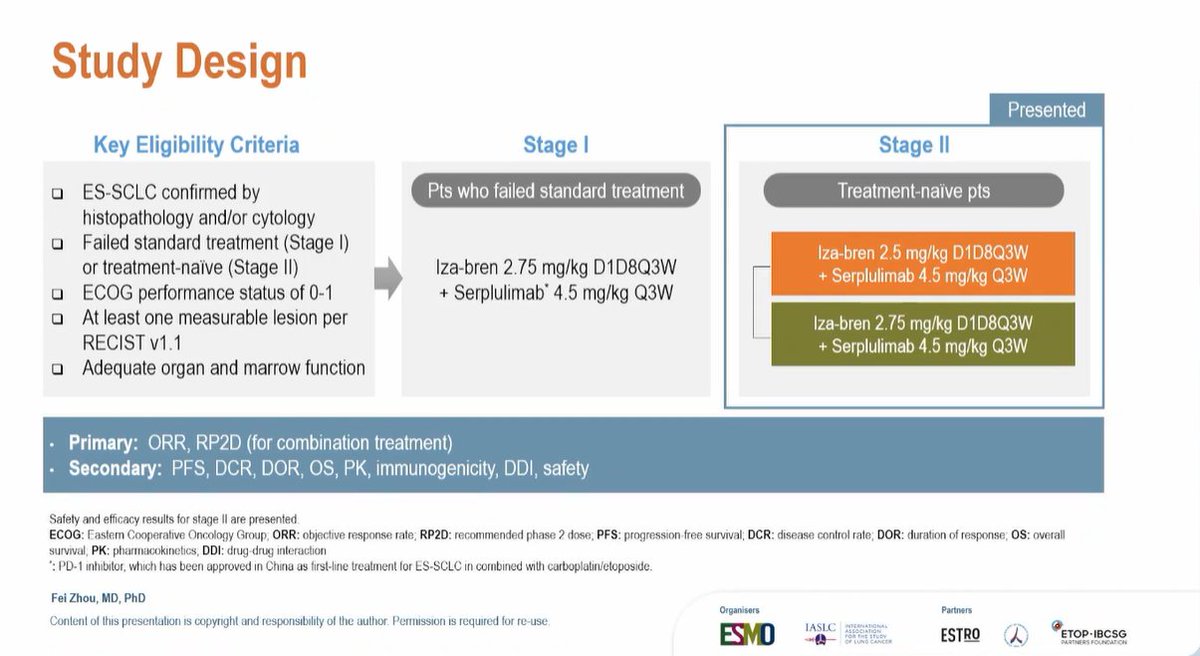
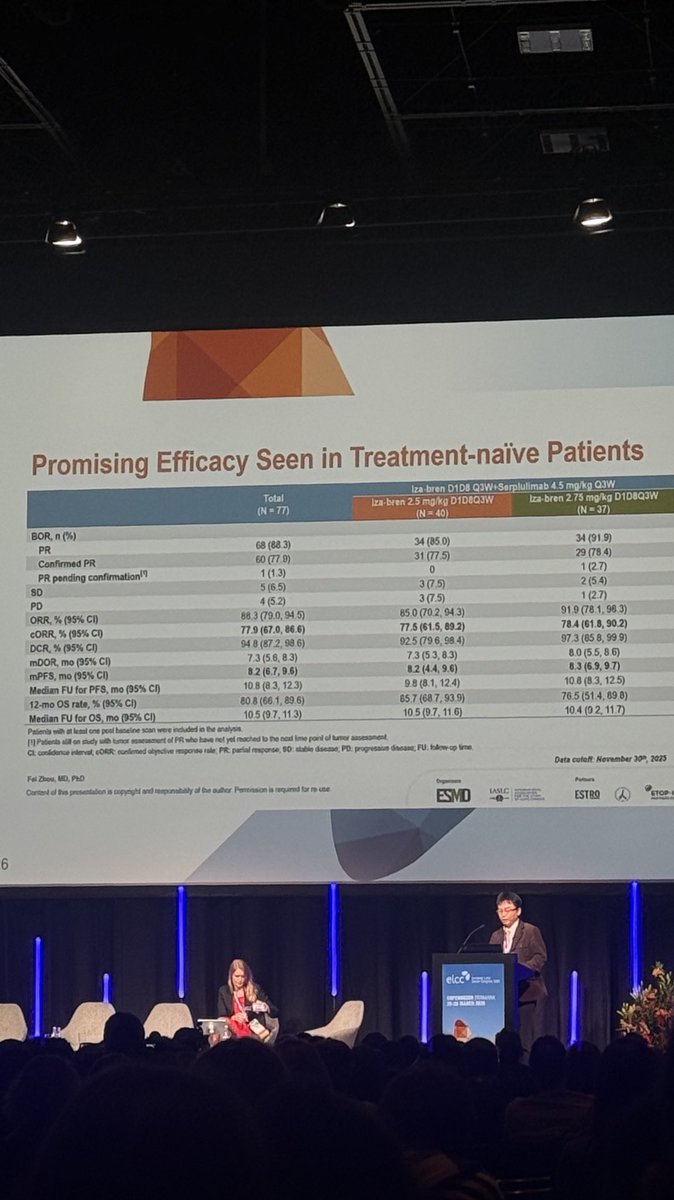
Phase II (408O): iza-bren (EGFR x HER3 bispecific ADC) + serplulimab in treatment-naive ES-SCLC
Study population
77…
🆙 #ELCC26 @myESMO 🇩🇰
🔥Proffered Paper session 1
☑️iza-bren (BL-B01D1) + serplulimab in SCLC
🎯ORR 88.3%, mPFS 8.2m, 12m OS rate 80.8%
🎙️Dr. Fei Zhou
🎙️Chair: @peters_solange
📍NCT06437509
@OncoAlert…
🔥 Can chemo-free IO + DLL3 targeting redefine 1L ES-SCLC? #ELCC26
Early-phase data of Iza-bren + Serplulimab shows striking activity in treatment-naïve patients
🧪 Study design
➡️ ES-SCLC | ECOG…
🔁REVIEW #ELCC26 @myESMO 🇩🇰
🔥Proffered Paper session 1
☑️iza-bren (BL-B01D1) + serplulimab in SCLC
🎯ORR 88.3%, mPFS 8.2m, 12m OS rate 80.8%
🎙️Dr. Fei Zhou
📍NCT06437509
@OncoAlert @Larvol #LCSM…
✨ Proffered session 1 at #ELCC26:
iza-bren (BL-B01D1) + serplulimab in ES-SCLC! EGFR x HER3 bispecific ADC + PD-1 (Ph. II, 1L setting)
🎯 Total (2.5mg/kg & 2.75mg/kg arms) ORR: 88.3% (cORR…
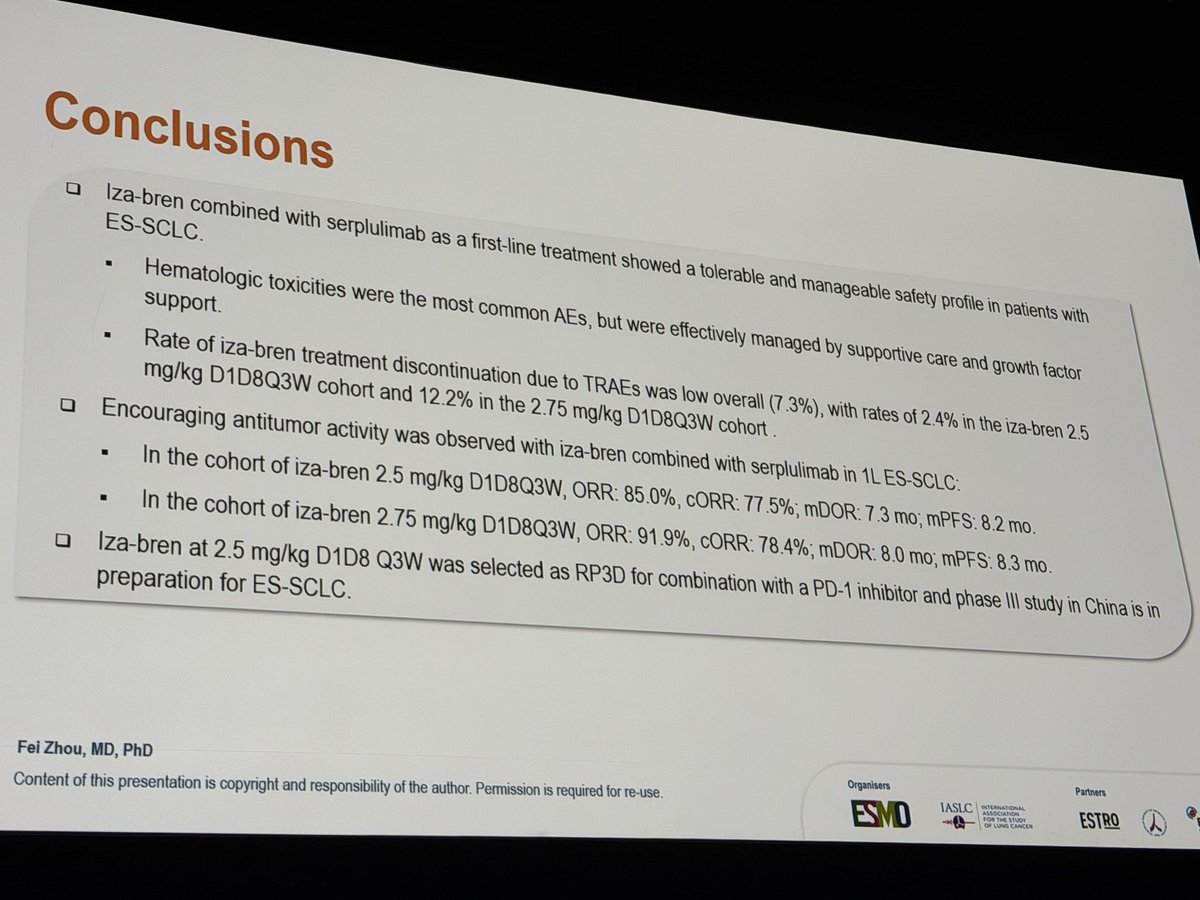
Frontline iza-bren in combination with serplulimab was associated with a tolerable and manageable safety profile and elicited responses in ES-SCLC. @myESMO #ELCC26 #ELCC2026 #lcsm…
@myESMO #ELCC26: Top Trials from Day 1
3082-CL-0101 | TOP | BL-B01D1-204-01 | NCT05879978
#ELCC #ELCC2026 #Cancer #Oncology #LungCancer #NSCLC #SCLC #lcsm #setidegrasib #osimertinib #izabren…

Bispecific ADC iza-bren + serplulimab shows striking phase 2 results in treatment-naive ES-SCLC, nearly doubling mPFS vs standard chemo-immunotherapy. A potential first-line paradigm shift? Read…
BL-B01D1 (iza-bren) is the first-in-class EGFRxHER3 bispecific ADC, combining dual-receptor targeting with a novel topoisomerase-I payload (Ed-04). Multi-tumor Phase I/II program from Baili-Bio/SystImmune. Strongest signal in EGFR-mutant NSCLC post-TKI (ORR 66%, mPFS 12.5 mo at IASLC 2025), motivating ongoing Phase III registrational study in China. Also showing activity in urothelial (ORR 43.5%), NPC (45.8%), and EGFR-wt NSCLC (40.5%). Competes with Dato-DXd (TROPION-Lung) and amivantamab + lazertinib (MARIPOSA) in later-line EGFR NSCLC. Hematologic toxicity is principal safety concern; notable absence of ILD given class risk.
Median: 66.0 % ORR (EGFR-mutant NSCLC (prior TKI, chemo-naive) at 2.5 mg/kg D1D8 Q3W). EGFR-mutant NSCLC (IASLC 2025, n=50) rate: 66.0% (ORR) vs. 56.0% (cORR) vs. 12.5% (mPFS months) vs. 13.7% (mDOR months). mOS at 12 months (EGFR-mutant subgroup) rate: 80.3% (12-mo OS rate %) vs. not reached% (mOS). ORR by tumor type (ASCO 2023) rate: 61.8% (NSCLC EGFR-mut) vs. 40.5% (NSCLC EGFR-wt) vs. 45.8% (NPC) vs. 14.3% (SCLC) vs. 7.7% (HNSCC). Urothelial cancer (NCT05785039) rate: 43.5% (ORR) vs. 91.3% (DCR). IASLC WCLC 2025 (most recent data, EGFR-mutant NSCLC subgroup): 50 patients with prior TKI + chemo-naive treated at 2.5 mg/kg D1D8 Q3W. ORR 66.0%, confirmed ORR 56.0%, median PFS 12.5 months, median DOR 13.7 months, mOS not reached (12-mo OS rate 80.3%). ASCO 2023 FIH Phase 1 (N=150, all tumor types): ORR 61.8% (EGFR-mut NSCLC), 40.5% (EGFR-wt NSCLC), 45.8% (NPC), 14.3% (SCLC), 7.7% (HNSCC). Urothelial cancer Phase Ib/II (NCT05785039): ORR 43.5%, DCR 91.3%. MTDs: 3.0 mg/kg D1D8 Q3W and 6.0 mg/kg D1 Q3W. Zhang et al., JCO 41:3001 (2023).
OS data: median not reached in EGFR-mutant NSCLC subgroup (IASLC 2025); 12-month OS rate 80.3%. No mature OS data from ASCO 2023 FIH across broader tumor types. Phase III registrational study ongoing in China as monotherapy for EGFR-mutant NSCLC post-3rd-generation TKI progression. 1.2% of patients discontinued due to TRAEs; no treatment-related deaths reported at IASLC 2025.
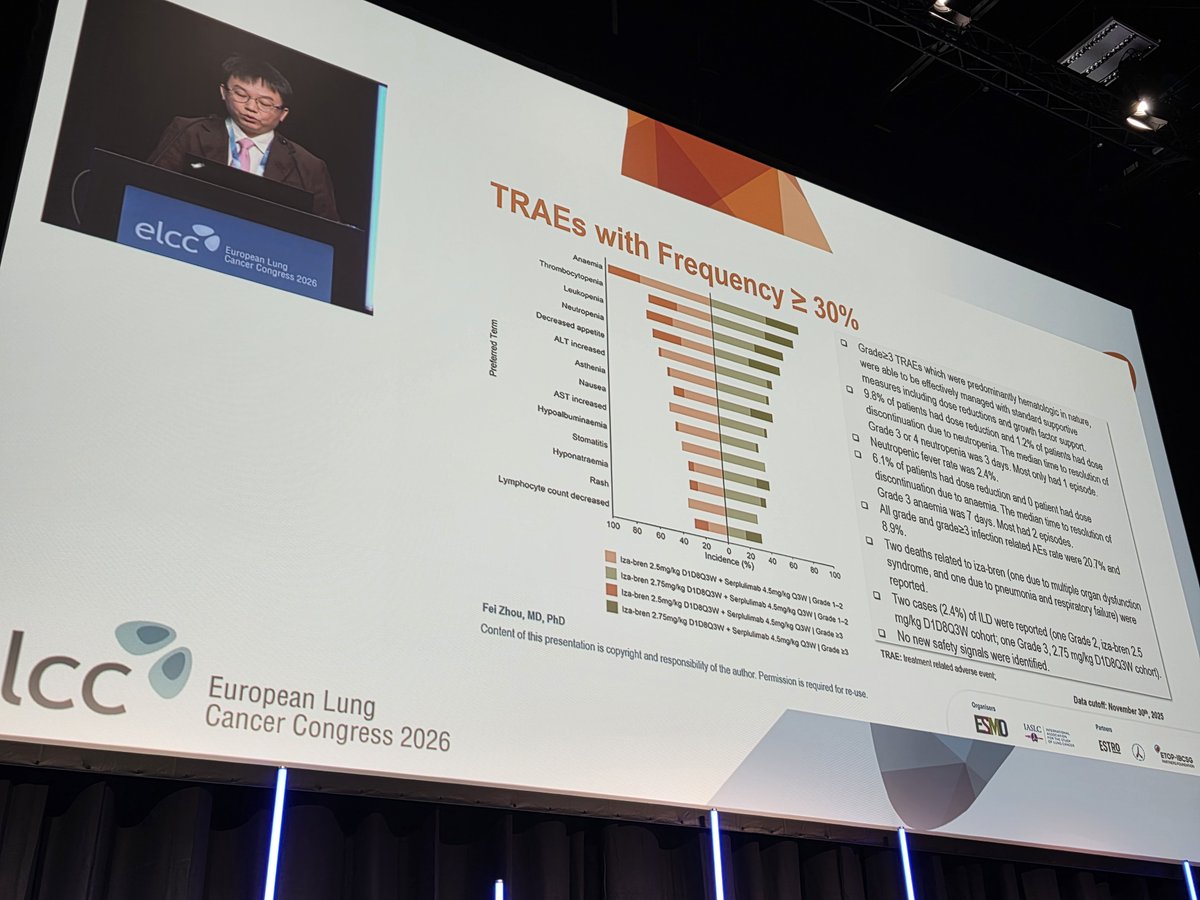
Grade ≥3 adverse events: neutropenia 34%, leukopenia 30%, thrombocytopenia 19%, anemia 15%% (hematologic). Key AEs: anemia (all-grade 90.6%; IASLC 2025), leukopenia (all-grade 80.7%), neutropenia (all-grade 78.4%), thrombocytopenia (all-grade 74.3%), nausea (29%), alopecia (30%), vomiting (28%), diarrhea (15%), NO ILD observed. Most common TRAEs are hematologic (anemia, leukopenia, neutropenia, thrombocytopenia all >70% any-grade in IASLC 2025 cohort). Non-hematologic TRAEs mostly low-grade: nausea, alopecia, asthenia. Grade ≥3 diarrhea only 2%; nausea/asthenia/decreased appetite <1% Grade ≥3. No ILD observed — notable given class risk of topoisomerase-I ADCs. Only 1.2% discontinued due to TRAEs. No treatment-related deaths.
🔬 Promising first-in-class EGFRxHER3 bispecific ADC — Phase III ongoing in EGFR-mutant NSCLC post-3rd-gen TKI. BL-B01D1 (iza-bren) is the first-in-class EGFRxHER3 bispecific ADC, combining dual-receptor targeting with a novel topoisomerase-I payload (Ed-04). Multi-tumor Phase I/II program from Baili-Bio/SystImmune. Strongest signal in EGFR-mutant NSCLC post-TKI (ORR 66%, mPFS 12.5 mo at IASLC 2025), motivating ongoing Phase III registrational study in China. Also showing activity in urothelial (ORR 43.5%), NPC (45.8%), and EGFR-wt NSCLC (40.5%). Competes with Dato-DXd (TROPION-Lung) and amivantamab + lazertinib (MARIPOSA) in later-line EGFR NSCLC. Hematologic toxicity is principal safety concern; notable absence of ILD given class risk.
BL-B01D1 (izalontamab brengitecan, 'iza-bren'; also BMS-986507) is a first-in-class EGFRxHER3 bispecific antibody-drug conjugate that pairs dual-receptor targeting with a topoisomerase-I payload. It is being developed by SystImmune/Baili-Bio across a multi-tumor program, with the most-discussed data in EGFR-mutant non-small cell lung cancer. The lead first-in-human study is NCT05983432.
In the EGFR-mutant NSCLC cohort reported at IASLC WCLC 2025 (n=50, at 2.5 mg/kg on days 1 and 8 every 3 weeks), BL-B01D1 produced an objective response rate of 66.0% (confirmed 56.0%), a median progression-free survival of 12.5 months, and a median duration of response of 13.7 months, with a 12-month overall survival rate of 80.3%. Overall survival was not yet mature.
No. BL-B01D1 (iza-bren) is investigational and is not FDA approved for any indication. Registrational Phase 3 studies are ongoing, largely in China (for example, in EGFR-mutant NSCLC after third-generation TKI progression). Its efficacy and safety are still being established in randomized trials.
Toxicity is predominantly hematologic. Grade 3 or higher events included neutropenia (34%), leukopenia (30%), thrombocytopenia (19%), and anemia (15%), with high all-grade rates of anemia (about 91%), leukopenia, neutropenia, and thrombocytopenia, plus nausea and alopecia. This myelosuppression profile is an important consideration for its development and combination strategies.
Targeting both EGFR and HER3 with a single antibody-drug conjugate may improve tumor delivery of the cytotoxic payload and address resistance driven by HER3 signaling, which is relevant after EGFR-TKI failure in NSCLC and across several EGFR/HER3-expressing tumors. BL-B01D1 is the first-in-class molecule pursuing this dual-target ADC approach.