Len-refractory MM (1-3 prior lines) - Janssen / Legend
Discover KOL Sentiment on CARTITUDE-4 →Design — Phase 3; cilta-cel (Carvykti, BCMA CAR-T) vs standard care (PVd or DPd) in lenalidomide-refractory R/R multiple myeloma, 1-3 prior lines (NCT04181827). (FDA label / NEJM 2023)
PFS — Median PFS not reached vs 11.8 mo — HR 0.26 (95% CI 0.18–0.38), p<0.001 (74% risk reduction); MRD-negativity (10⁻⁵) 62% vs 18.5%. (CARTITUDE-4, page data / NEJM)
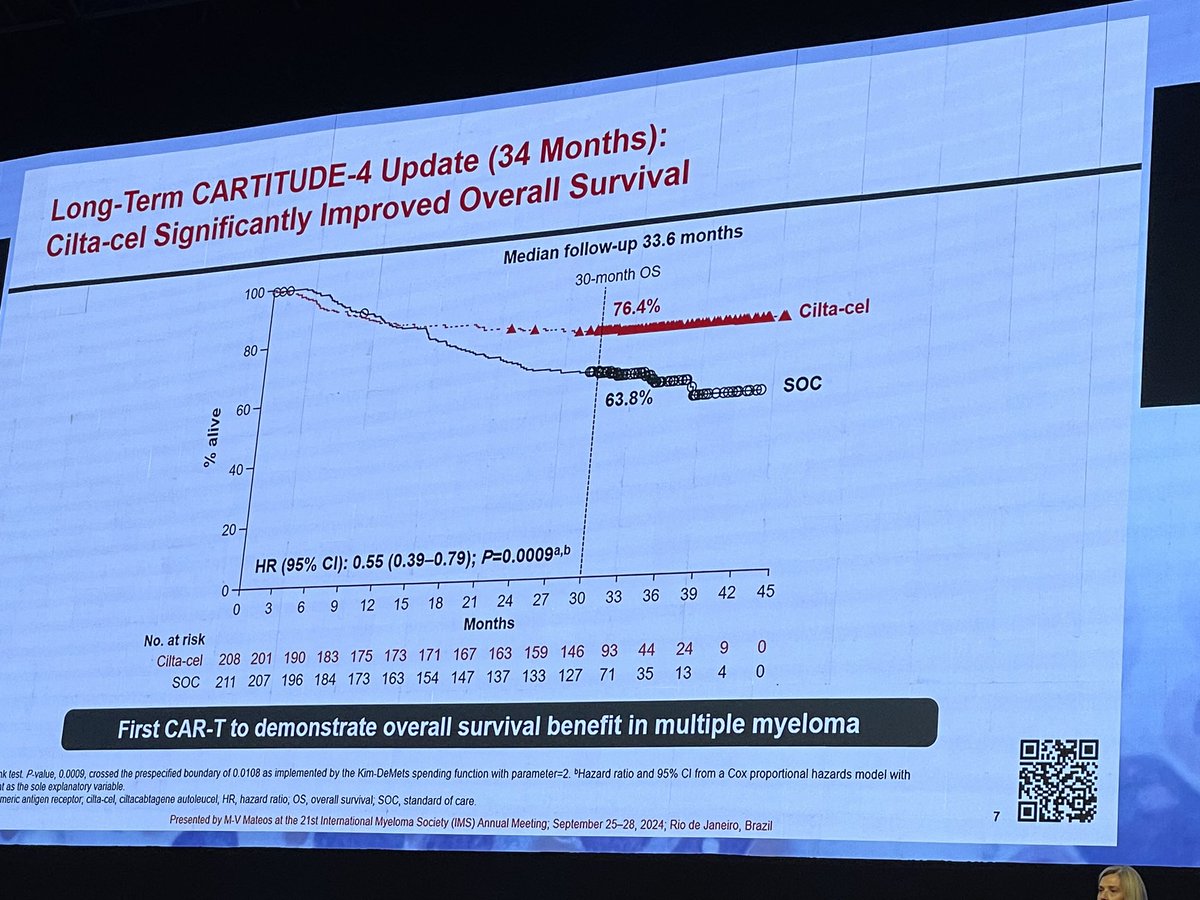
OS — Significant overall survival benefit: HR 0.55 (95% CI 0.39-0.79; p=0.0009); 30-mo OS 76% vs 64% — first cell therapy with an OS benefit in myeloma. (ASH 2025 update)
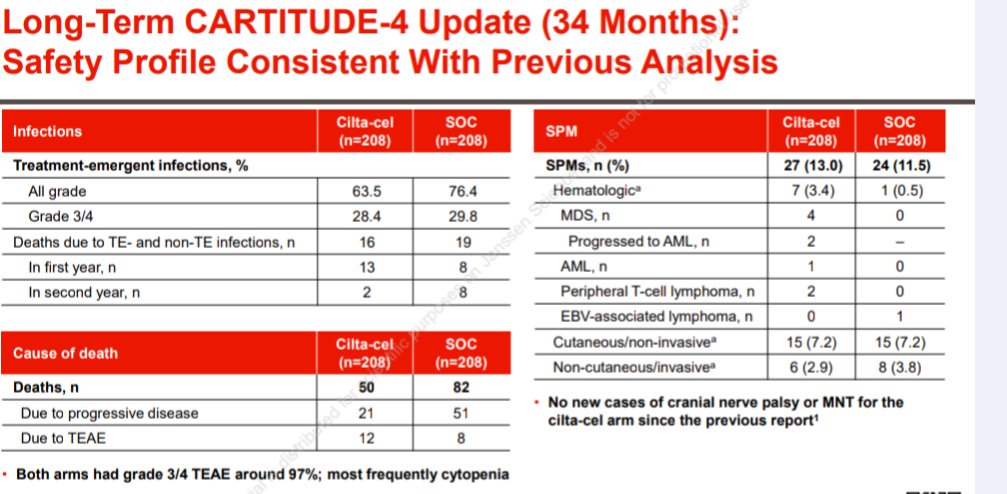
Safety — CRS 78% (3% Gr 3-4); ICANS 7% (0.5% Gr 3); Gr 3/4 cytopenias >50%. (page data)
Regulatory — FDA approved (Apr 5, 2024) for R/R MM after ≥1 prior line incl. PI+IMiD and lenalidomide-refractory. (FDA.gov)
Sponsor / Drug — Janssen (J&J) / Legend Biotech; ciltacabtagene autoleucel (Carvykti), single BCMA CAR-T infusion. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 20, 2026.











Top 10 by impressions - click to view on X
#mmsm How to counsel patients about Cilta Cel using the data from CARTITUDE-4 and FDA ODAC meeting for earlier use With data of Cilta cel and Ide cel, assuming having access to...
CARTITUDE-4 risk of secondary hematologic malignancies is very concerning. I am becoming increasingly concerned about this CART being used in the frontline (and god forbid) smoldering setting Also...
Car T is officially a hematopoietic carcinogen. If the trial control arm was ethical it would include Kpd and DKd and it might be a negative trial.
Parkinson's disease is through the roof with car t. Not 1% anymore. 3%. And it seldom gets better. Car t is a 470k disaster in the making. If the trial allowed KPd and DKd...
👀 OS data from CARTITUDE-4 (cilta-cel CAR-T versus #MMsm standard therapies in 1-3 lines). This is WONDERFUL to see!! Looking forward to hearing the ODAC meeting later this week......
Breaking: ODAC votes 11-0 to recommend approval of ciltacel in patients with relapsed/refractory multiple myeloma in earlier stages. I’m glad. Right call. But we need to be careful. Read on.
CAR T #cartitude4 #mmsm
This is truly an excellent thread on how to discuss Cilta Cel with your patients. Samer provides excellent insight and shares how his brain is processing the new data. Much better tweet than just...
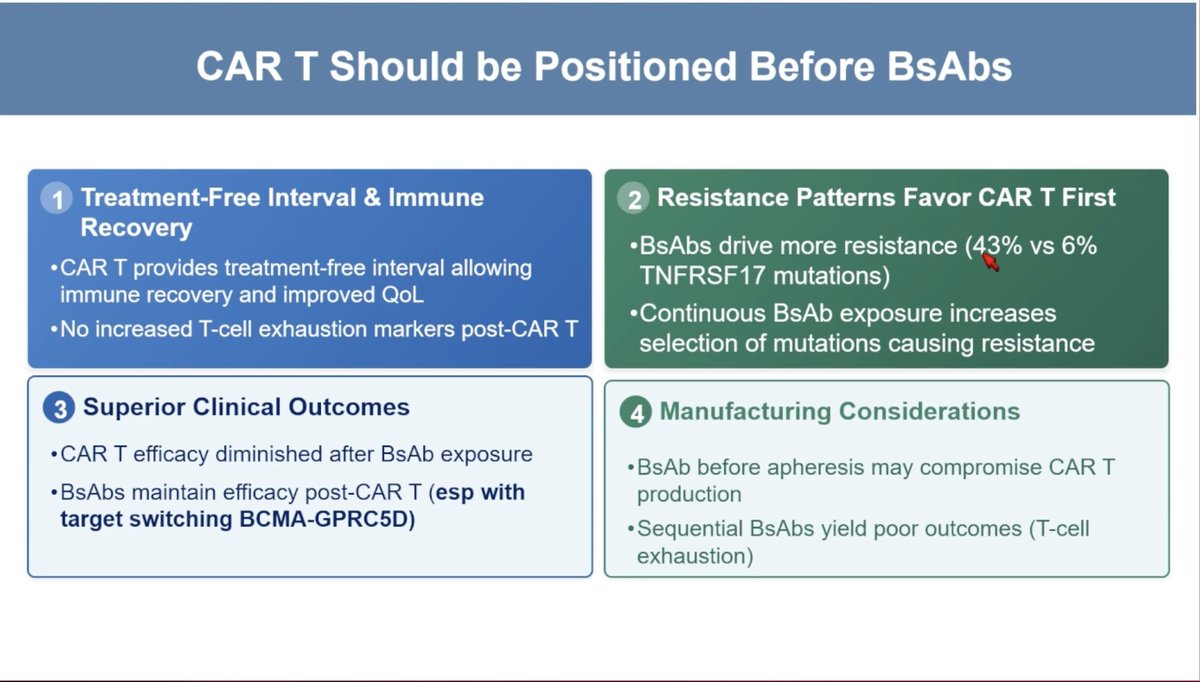
#ASH25 #mmsm @ASH_hematology Treatment Refinement in Multiple Myeloma @SLentzsch Reasons why CAR-T should be positioned before BsAbs

Two patients with refractory myeloma who had excellent antitumor responses to cilta-cel CAR T-cell therapy later had T-cell lymphomas that contained the lentivirus construct used to generate the CAR...
CARTITUDE-4 is a clinical trial evaluating Ciltacabtagene autoleucel (cilta-cel) in Lenalidomide-refractory multiple myeloma. Sponsored by Janssen / Legend Biotech. KOL discussion spans multiple conferences with 215 tracked posts from 62 oncology opinion leaders generating 519.3K total impressions.
Phase 3, randomized, open-label trial comparing a single infusion of ciltacabtagene autoleucel (cilta-cel) versus standard of care (PVd or DPd) in patients with relapsed and lenalidomide-refractory multiple myeloma after 1-3 prior lines of therapy.
Adults with relapsed or refractory multiple myeloma who received at least 1 prior line of therapy including a proteasome inhibitor and an immunomodulatory agent, and are refractory to lenalidomide.
Carvykti (ciltacabtagene autoleucel/cilta-cel), a BCMA-directed CAR-T cell therapy given as a single IV infusion, versus standard therapies of pomalidomide-bortezomib-dexamethasone (PVd) or daratumumab-pomalidomide-dexamethasone (DPd).
Primary: progression-free survival (PFS). Key secondary: overall survival (OS), overall response rate (ORR), MRD negativity rate, duration of response (DOR).
Cilta-cel demonstrated a 74% reduction in risk of progression or death. Median PFS not reached (95% CI: 34.5-NE) versus 11.8 months (HR 0.26; 95% CI 0.18–0.38; p<0.001). MRD negativity (10^-5): 62% versus 18.5%.
45% reduction in risk of death (HR 0.55; 95% CI: 0.39-0.79; p=0.0009). 30-month OS rates: 76% for cilta-cel versus 64% for standard care. First cell therapy with OS benefit in myeloma.
CRS in 78% (3% Grade 3-4). ICANS in 7% (0.5% Grade 3). Grade 3/4 cytopenias >50%. No new safety signals at 34-month follow-up.
FDA expanded approval April 5, 2024 — first BCMA-targeted therapy as early as first relapse. Long-term data suggest potential cure fraction in standard-risk patients (80.5% PFS at 2.5 years). Single infusion offers treatment-free period.
CARTITUDE-4 is a Phase 3 trial of ciltacabtagene autoleucel (cilta-cel, Carvykti), a BCMA-directed CAR-T therapy, versus standard-of-care regimens in adults with lenalidomide-refractory relapsed/refractory multiple myeloma who had received 1-3 prior lines of therapy (NCT04181827).
Yes. On April 5, 2024 the FDA expanded the approval of Carvykti (ciltacabtagene autoleucel) to adults with relapsed/refractory multiple myeloma who have received at least one prior line of therapy including a proteasome inhibitor and an immunomodulatory agent and are refractory to lenalidomide. CARTITUDE-4 supported this earlier-line expansion.
Cilta-cel reduced the risk of progression or death by 74% versus standard care — median PFS was not reached versus 11.8 months (HR 0.26; 95% CI 0.18–0.38; p<0.001). It also showed a statistically significant overall survival benefit (HR 0.55; 95% CI 0.39-0.79; p=0.0009), the first cell therapy to demonstrate an OS benefit in myeloma. MRD-negativity at 10⁻⁵ was 62% versus 18.5%.
Cytokine release syndrome occurred in 78% of patients (3% Grade 3-4) and immune effector cell-associated neurotoxicity (ICANS) in 7% (0.5% Grade 3). Grade 3/4 cytopenias occurred in more than half of patients. As a CAR-T therapy, Carvykti carries risks of CRS, neurologic toxicities, and delayed cytopenias.
Ciltacabtagene autoleucel (Carvykti) is developed by Janssen (Johnson & Johnson) and Legend Biotech. It is an autologous BCMA-directed CAR-T therapy given as a single infusion after lymphodepleting chemotherapy.