TE-NDMM induction - Janssen
Discover KOL Sentiment on CASSIOPEIA →







Top 10 by impressions - click to view on X
A critical appraisal of the long-term follow-up of CASSIOPEIA trial, daratumumab maintenance, and maintenance in general. An educational thread. 1/🧵 #mmsm Non-paywalled link to...
Some considerations on long-term follow-up of the CASSIOPEIA randomised controlled phase 3 trial - The Lancet Oncology 1/x
I agree with most of this nice thread Super unethical to not give the control arm len The bar for maintenance has to be OS with appropriate post protocol therapy. There's a...
To dara or not to as maintenance? The Cassiopeia trial update is out! Among Dara-treated patients in induction, Dara maintenance offered some benefit over placebo with 6 years f/u. HR (0.76) is...
Almost all myeloma trials are bad. It's really astonishing how bad their control arms are and how bad their post-protocol therapy is You would think with all those ad boards...
PERSEUS➡️Important to note that NO signal for increased early mortality from toxicity with Dara-VRd compared to VRd. OS curves trending in the right direction (similar to CASSIOPEIA)! These data...
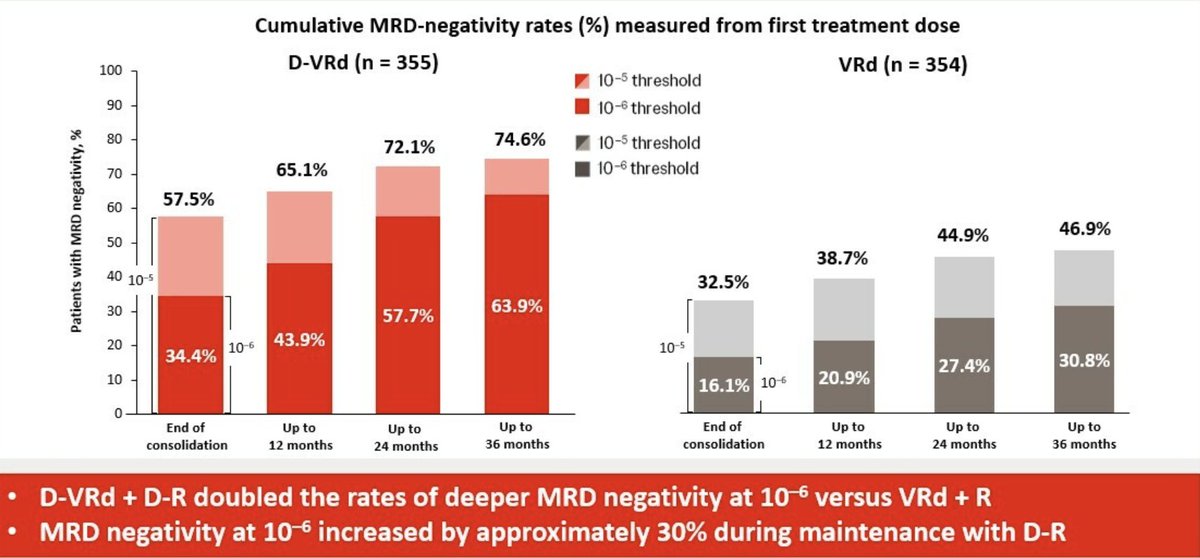
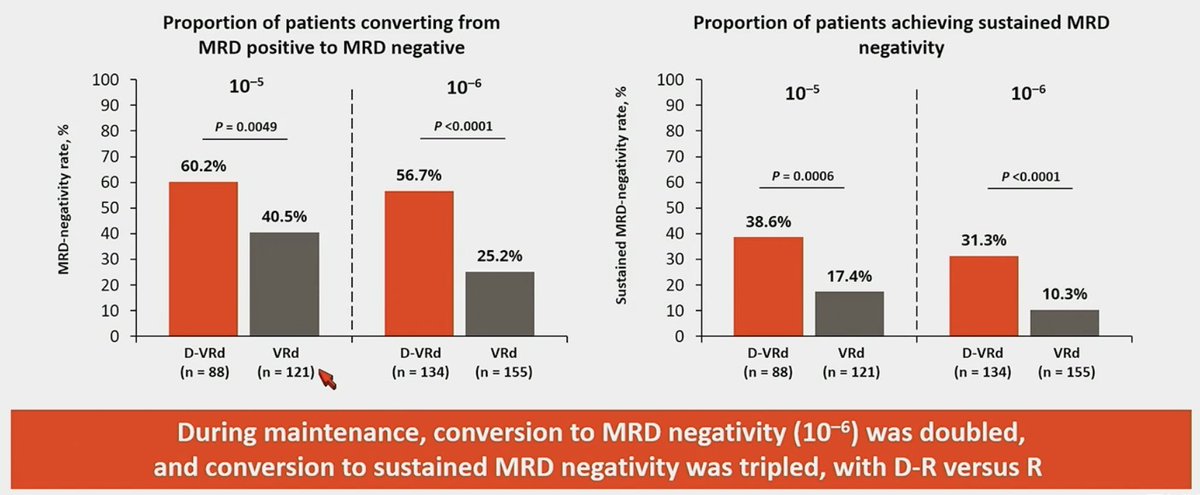
PERSEUS MRD Data: Maintenance upgraded MRD(-) responses up to 2-3 years later, and appears to be more profound with Dara-R maintenance. Dara-VRd/Dara-R doubled chances of reaching MRD negativity...
CASSIOPEIA is often criticized because of the q8 week maintenance schedule. If the q8 maintenance schedule was so insufficient, why did it so dramatically improve outcomes versus observation for...
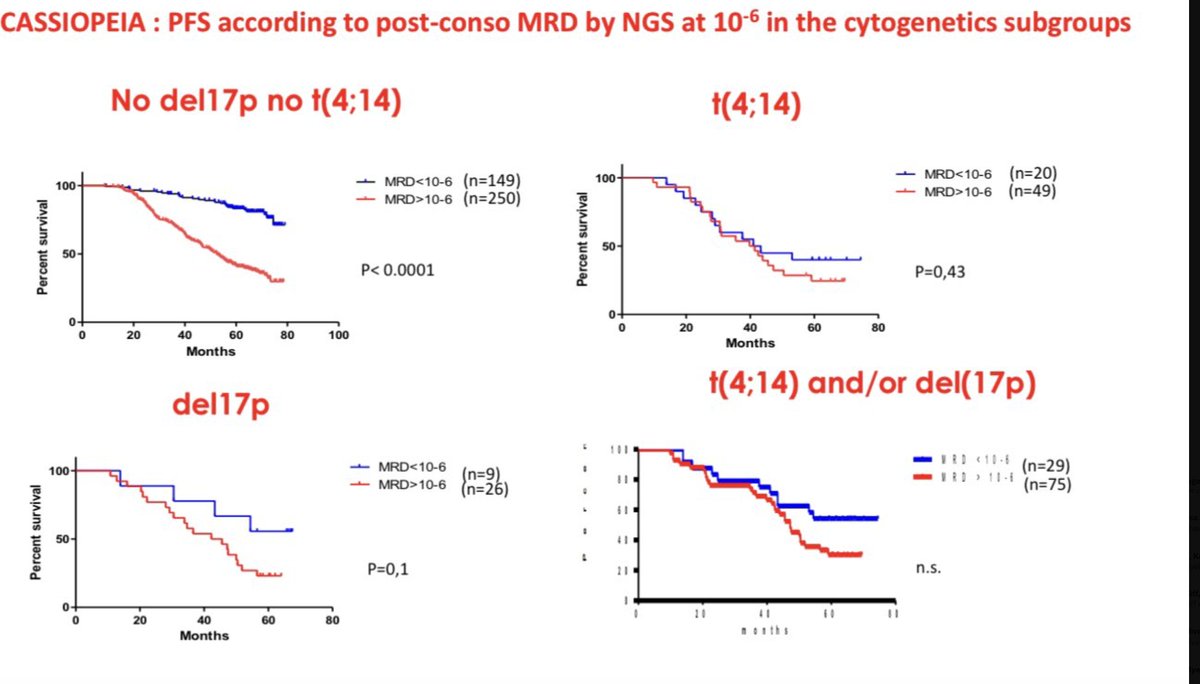
3) In a randomized trial (CASSIOPEIA), for those with high risk myeloma, outcomes were poor regardless of whether they achieved MRD negativity at 10-6 or not, indicating that single timepoint of MRD...
🔥 Tune in to our new episode on maintenance therapy in #MultipleMyeloma with @HiraSMian & @ManniMD1 ! We discuss a wide range of RCTs from CALGB to FORTE,...
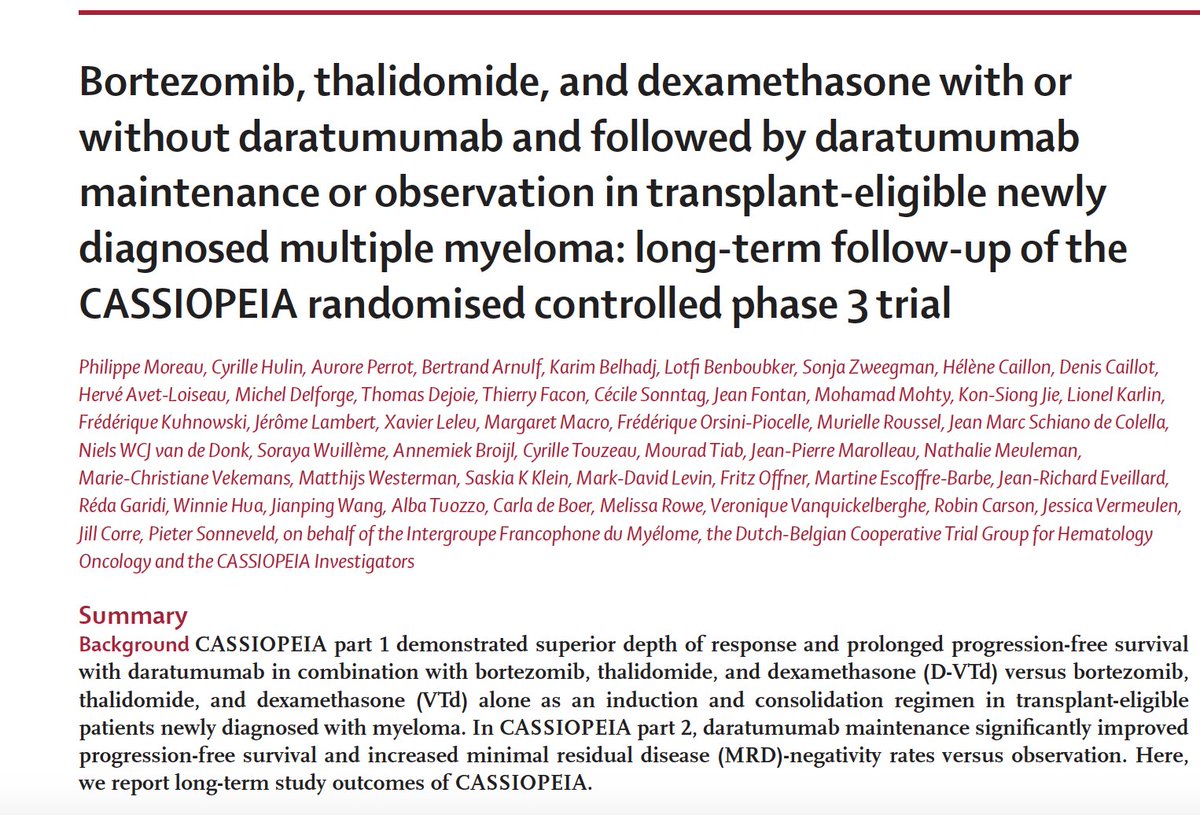
CASSIOPEIA is a landmark Phase III, open-label, randomized trial that established the addition of daratumumab (Darzalex) to bortezomib, thalidomide, and dexamethasone (D-VTd) as standard induction/consolidation therapy for transplant-eligible newly diagnosed multiple myeloma. The trial enrolled 1,085 patients across European centers in a unique two-part design: Part 1 evaluated D-VTd versus VTd as induction/consolidation around autologous stem cell transplant (ASCT), while Part 2 re-randomized responders to daratumumab maintenance versus observation for up to 2 years. With over 80 months of follow-up, CASSIOPEIA demonstrated that daratumumab-based therapy across the treatment continuum produces the deepest and most durable MRD negativity, translating to superior long-term PFS and OS outcomes.
Phase III, European multicenter, open-label, 1:1 randomized trial with a two-part design. Part 1: D-VTd vs VTd induction (4 cycles) and consolidation (2 cycles) around single ASCT. Part 2: re-randomization of patients achieving at least partial response to daratumumab maintenance (16 mg/kg IV q8w) vs observation for up to 2 years. No companion diagnostic required.
Adults with newly diagnosed multiple myeloma eligible for high-dose therapy and autologous stem cell transplant, aged 18-65 years. A total of 1,085 patients were randomized between September 2015 and August 2017 (543 to D-VTd, 542 to VTd). For Part 2, 886 patients were re-randomized (442 to daratumumab maintenance, 444 to observation).
Part 1: Daratumumab 16 mg/kg IV combined with bortezomib, thalidomide, and dexamethasone (D-VTd) versus VTd alone for 4 induction cycles pre-ASCT and 2 consolidation cycles post-ASCT. Part 2: Daratumumab 16 mg/kg IV every 8 weeks maintenance versus observation for up to 2 years.
Part 1 primary endpoint: stringent complete response (sCR) rate at Day 100 post-ASCT. Part 2 primary endpoint: progression-free survival (PFS) from second randomization. Secondary endpoints included overall survival (OS), MRD negativity rates at predefined sensitivity thresholds (10^-5 and 10^-6), and safety.
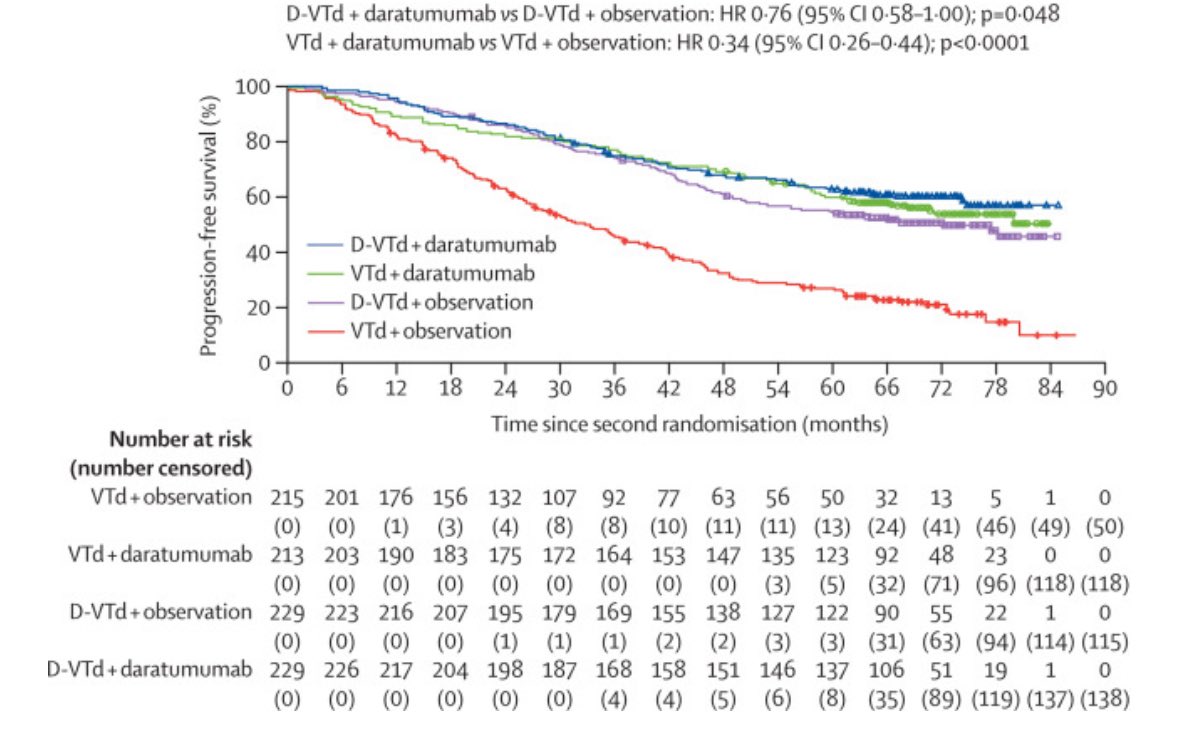
In Part 1, D-VTd reduced the risk of progression or death by 53% versus VTd (HR 0.47; 95% CI: 0.33-0.67; p<0.0001) at a median follow-up of 18.8 months. At the long-term follow-up of 80.1 months, median PFS was 83.7 months in the D-VTd arm versus 52.8 months in the VTd arm (HR 0.61; p<0.0001). In Part 2, daratumumab maintenance significantly improved PFS versus observation (median not reached vs 45.8 months; HR 0.49; 95% CI: 0.40-0.59; p<0.0001). The benefit was most pronounced in the VTd-to-daratumumab group (HR 0.34) compared with D-VTd-to-daratumumab (HR 0.76).
At the 80-month follow-up, D-VTd induction/consolidation significantly improved overall survival compared with VTd alone. Estimated 72-month OS rates were 86.7% in the D-VTd group versus 77.7% in the VTd group, with median OS not reached in either arm. D-VTd followed by daratumumab maintenance produced the best long-term survival outcomes across all treatment subgroups.
The most frequent adverse events (occurring in 20% or more of patients) with D-VTd were infusion reactions, peripheral sensory neuropathy, constipation, asthenia, nausea, peripheral edema, neutropenia, thrombocytopenia, pyrexia, and paresthesia. Adverse events occurring at 5% or greater frequency in D-VTd versus VTd included infusion reactions, nausea, neutropenia, thrombocytopenia, lymphopenia, and cough. There were no significant differences in the number or type of serious adverse events between the two arms. Peripheral neuropathy led to thalidomide-to-lenalidomide switches in 2.3% of D-VTd patients during consolidation.
CASSIOPEIA established D-VTd as a standard induction/consolidation regimen for transplant-eligible NDMM and demonstrated the value of daratumumab maintenance post-transplant. The trial showed that continuous daratumumab exposure across induction, consolidation, and maintenance produces the deepest MRD negativity (77.3% at 10^-5, 60.7% at 10^-6) and best long-term PFS. A key clinical debate remains: the D-VTd (thalidomide) backbone from CASSIOPEIA has been largely supplanted by D-VRd (lenalidomide) based on the PERSEUS and GRIFFIN trials, though CASSIOPEIA long-term data continue to inform treatment sequencing and MRD-guided strategies.