[Slide 1]
Benefit vs Overtreatment - MIBC Cohort
NIVOLUMAB
PLACEBO
Patients with
Patient is already
Recurred
cured
benefit from
Recurred
Patient is already cured
at 3 years
nivolumab =
adjuvant nivo
at 3 years
does not need treatment
overtreatment
Total
pts
53%
15%
32%
Total pts
68%
32%
281
279
ASCO Genitourinary
CHECKMATE 274 Milowsky et al. ASCO GU 2025
#GU25
ASCO
AMERICAN SOCIETY OF
PRESENTED BY:
Elizabeth Plimack, MD MS FASCO
CLINICAL ONCOLOGY
Cancers Symposium
Presentation * property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 2]
For Checkpoint inhibitors - persistent PD1 receptor occupancy suggests that
effects of NAC extend into the adjuvant period even without adjuvant dosing
300
100
100
80
80
[MDX-1106] (ug/mL)
200
60
10 mg/kg
(n = 10)
40
100
PD-1 Occupancy (%)
PD-1 Occupancy (%)
Pt. 4033
60
40
[MDX-1106] (ug/mL)
KX
PD-1 occupancy (%)
20
20
0
0
20
40
60
80
0
100
200
300
400
500
600
Time (days)
Time (days)
One dose of nivolumab saturates PD1 receptors out beyond 3 mo
With 3 doses of nivolumab
even as drug itself is cleared
PD1 receptors remain occupied (40%) at ~380 days from last dose
ASCO Genitourinary
Brahmer et al., Phase I study of single-agent anti-
#GU25
PRESENTED BY:
ASCO
AMERICAN SOCIETY OF
Elizabeth Plimack, MD MS FASCO
CLINICAL ONCOLOGY
Cancers Symposium
programmed death-1 (MDX-1106) in refractory
Presentation . property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
solid tumors. J Clin Oncol 28, 3167-3175 (2010)
---
[Slide 3]
NIAGARA in the context of currently available treatment options
NIAGARA
VESPER
COXEN
Durvalumab
90%
N=533
Durvalumab
Gem Cis X 4
Gem Cis x 4
R
Gem Cis
Cystectomy
x8mo
MIBC
R
1:1
N 437pts
Cystectomy
MIBC
R
MIBC
Gem Cis
ddMVAC X 6
N 227pts
Cystectomy
No treatment
ddMVAC X 4
N=530
91%
DGC "sandwich" VS GC
ddMVAC VS GC
ddMVAC VS GC
EFS benefit at 2 yrs: 8%
EFS benefit at 5 yrs: 9%
EFS benefit at 5 yrs: 4%
OS benefit at 2 yrs: 7%
OS benefit at 5 yrs: 9%
OS benefit at 5 yrs: 7%
Differences were not statistically significant
60%
55%
COXEN
52%
ddMVAC
46%
50%
VESPER
41%
41%
40%
37%
Age Range, Median
DurvaGC
NIAGARA
30%
20%
NIAGARA
10%
GC
COXEN
0%
VESPER
Rate of Grade 3/4 TRAE
ddMVAC
DurvaGC
GC
30
40
50
60
70
80
90
VESPER range provided by C Culine/VESPER team
Age (years)
NIAGARA
COXEN
VESPER
Age range was previously reported as 95% CI
ASCO Genitourinary
NIAGARA Galsky et al. ASCO GU 2025
#GU25
PRESENTED BY:
Elizabeth Plimack, MD MS FASCO
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
Cancers Symposium
Pfister et al. The Lancet Onc 25, 255-264 (2024).
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
Flaig et al. Eur Urol 84, 341-347 (2023).
---
[Slide 4]
NIAGARA in the context of currently available treatment options
NIAGARA
VESPER
COXEN
Durvalumab
90%
N=533
Durvalumab
Gem Cis X 4
Gem Cis X 4
R
Gem Cis
Cystectomy
X 8 mo
MIBC
R
1:1
N 437pts
Cystectomy
MIBC
R
MIBC
Gem Cis
ddMVAC X 6
N 227pts
Cystectomy
No treatment
ddMVAC X 4
N=530
91%
DGC "sandwich" VS GC
ddMVAC VS GC
ddMVAC VS GC
EFS benefit at 2 yrs: 8%
EFS benefit at 5 yrs: 9%
EFS benefit at 5 yrs: 4%
OS benefit at 2 yrs: 7%
OS benefit at 5 yrs: 9%
OS benefit at 5 yrs: 7%
Differences were not statistically significant
100%
100%
80%
80%
Path Complete Response
ypTONO rate
60%
2 year Overall Survival
60%
40%
2-year OS rate
40%
20%
20%
32%
42%
37%
28%
34%
36%
82%
83%
82%
75%
77%
78%
0%
0%
ddMVAC
DurvaGC
GC
ddMVAC
DurvaGC
GC
NIAGARA
COXEN
VESPER
NIAGARA
COXEN
VESPER
ASCO Genitourinary
NIAGARA Galsky et al. ASCO GU 2025
#GU25
PRESENTED BY:
Elizabeth Plimack, MD MS FASCO
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
Cancers Symposium
Pfister et al. The Lancet Onc 25, 255-264 (2024).
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
Flaig et al. Eur Urol 84, 341-347 (2023).
[Slide 1]
ASCO Genitourinary
Abstract 658
Cancers Symposium
Adjuvant nivolumab (NIVO) vs placebo (PBO) for high-risk muscle-invasive urothelial carcinoma
(MIUC): Additional efficacy outcomes including overall survival (OS) in patients (pts) with muscle-
invasive bladder cancer (MIBC) from CheckMate 274.
Authors: Matthew I. Milowsky & Matthew D. Galsky et al.
os Trends Favor NIVO vs. PBO
Background:
All MIBC: NR vs. 39.9 months (HR 0.70 [0.55-0.90])
CheckMate 274 showed adjuvant nivolumab (NIVO) improves DFS in
PD-L1 ≥ 1%: NR vs. 37.6 months (HR 0.48 [0.29-0.77])
high-risk muscle-invasive urothelial carcinoma (MIUC).
With prior NAC: 55.2 vs. 40.2 months (HR 0.74 [0.53-1.03])
*With 3-year median follow-up, further analyses explore overall
Without prior NAC: NR vs. 37.7 months (HR 0.67 [0.47-0.95])
survival (OS) in muscle-invasive bladder cancer (MIBC).
Safety Profile:
Objective: Assess DFS & os in MIBC patients, including PD-L1+ and
Consistent with prior data; no new safety signals.
prior NAC subgroups.
Conclusion:
Key Results (N=560 MIBC patients, Median FU: 36.1 months)
NIVO continues to demonstrate DFS and os benefit in MIBC,
Disease-Free Survival (DFS) Benefit with NIVO vs. Placebo (PBO)
including PD-L1+ and prior NAC subgroups.
All MIBC: 25.6 vs. 8.5 months (HR 0.63 [0.51-0.78])
These results reinforce adjuvant NIVO as the standard of care for
*With prior NAC: 19.6 vs. 8.3 months (HR 0.58 [0.43-0.79])
high-risk MIUC and MIBC.
Without prior NAC: 25.9 vs. 13.7 months (HR 0.69 [0.50-0.94])
Potentially curative option for patients post-radical surgery.
X
@nataliagandur
@drnataliagandur
GANDUR
[Slide 1]
2
---
[Slide 2]
pCR vs non-pCR OS data should not be extrapolated to support
contribution of adjuvant
1.0
pCR
95.5%
Absolute 2 year OS in
0.8
91.1%
pCR group - 4%
non-pCR
Probability of survival
0.6
Benefit may all be from
74.1%
durable receptor
04
68.9%
occupancy, or more
durable IO response to
the neoadjuvant
0.2
Durvalumab am
component compared
Comparator am
with GC alone
0
0
2
4
6
8
10
12
14
16
18
20
22
24
26
28
30
32
34
36
38
40
42
44
46
48
50
52
54
56
58
60
62
64
68
No of patients X nex
Time from randomization (months)
Dam
199
199
157
154
194
194
193
192
190
189
189
189
189
187
186
185
154
176
164
149
139
129
111
95
83
68
54
44
31
14
11
2
0
0
Cam
146
145
145
144
144
143
142
140
139
137
136
134
133
133
132
130
130
124
117
109
100
93
85
76
65
51
40
31
23
15
7
3
0
0
Dam
334
329
320
311
298
284
275
265
256
251
245
239
234
231
224
223
215
199
185
172
156
142
127
112
99
84
71
52
37
20
10
5
1
0
Cam
384
370
361
346
323
307
296
285
274
255
256
249
245
240
236
233
228
210
154
172
159
146
130
118
109
90
73
59
37
23
14
7
2
0
ASCO Genitourinary
NIAGARA Galsky et al. ASCO GU 2025
Cancers Symposium
#GU25
PRESENTED DY
Elizabeth Plimack, MD MS FASCO
ASCO
AMERICAN SOCIETY or
CUNICAL CHICOLOGY
Presentation . property IF the author and ASCO Permission required - - contact generag
KNOWLEDGE CONQUERS CANCER
---
[Slide 3]
CheckMate 274
OSᵃ: all randomized patients with MIBC
100
Median OS (95% CI), months
90
NIVO
NR (45.0-NE)
80
75.3%
PBO
39.9 (29.8-52.1)
HR (95% CI), 0.70 (0.55-0.90)
Overall survival probability (%)
70
64.2%
60
66.2%
50
53.7%
40
30
20
10
0
0
6
12
18
24
30
36
42
48
54
60
66
72
78
Months
No. at risk
NIVO
279
258
239
213
193
172
145
107
81
56
34
20
3
0
PBO
281
240
218
195
172
143
119
89
65
43
31
17
6
0
"Interim OS analysis.
Median follow-up of 36.1 months in the ITT population and 34.5 months in the MIBC population.
Galsky MD, et al. J Clin Oncol 2025;43:15-21.
---
[Slide 4]
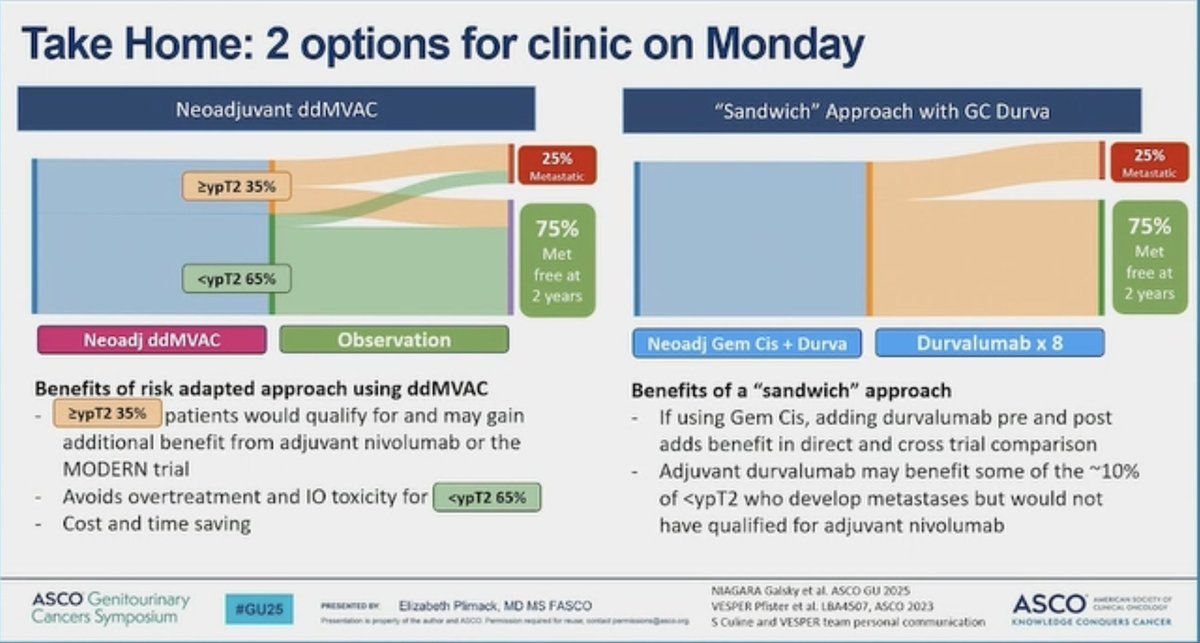
Take Home: 2 options for clinic on Monday
Neoadjuvant ddMVAC
"Sandwich" Approach with GC Durva
25%
25%
Metastatic
Metastatic
ZypT2 35%
75%
75%
Met
Met
<ypT2 65%
free at
free at
2 years
2 years
Neoadj ddMVAC
Observation
Neoadj Gem Cis + Durva
Durvalumab X 8
Benefits of risk adapted approach using ddMVAC
Benefits of a "sandwich" approach
-
ZypT2 35% patients would qualify for and may gain
- If using Gem Cis, adding durvalumab pre and post
additional benefit from adjuvant nivolumab or the
adds benefit in direct and cross trial comparison
MODERN trial
- Adjuvant durvalumab may benefit some of the ~10%
-
Avoids overtreatment and IO toxicity for
<ypT2 65%
of <ypT2 who develop metastases but would not
- Cost and time saving
have qualified for adjuvant nivolumab
NIAGARA Galsky et at. ASCO GU 2025
ASCO Genitourinary
#GU25
PRESENTED EX
Elizabeth Plimack, MD MS FASCO
VESPER Pfister et at. LBA4507, ASCO 2023
ASCO
AMERICAN SOCIETY OF
CLINICAL CHICOLOGY
Cancers Symposium
Presentation . property of the author and ASCO Permission request Rar - contact permissions@amin.org
S Culine and VESPER team personal communication
KNOWLEDGE CONQUERS CANCER
[Slide 1]
08:15 - 08:25 GMT-8
+
ABSTRACT PRESENTATION 1
Adjuvant nivolumab (NIVO) vs placebo (PBO)
for high-risk muscle-invasive urothelial
carcinoma (MIUC): Additional efficacy
outcomes including overall survival (OS) in
patients (pts) with muscle-invasive bladder
cancer (MIBC) from CheckMate 274.
Abstract 658
Matthew I. Milowsky, MD,
FASCO
University of North Carolina School of
Medicine
---
[Slide 2]
Results:
Of 709 randomized pts (ITT), 560 (79%) had MIBC
(NIVO, n = 279; PBO, n = 281); 284 (51%) of MIBC
pts had prior NAC. With median follow-up of 36.1
mo (ITT), DFS improvement with NIVO vs PBO was
consistent between all pts with MIBC (hazard ratio
[HR] 0.63) and those with (HR 0.58) and without
prior NAC (HR 0.69; Table). For OS, HRs favored
NIVO vs PBO in all pts with MIBC (HR 0.70) and
the tumor PD-L1 ≥ 1% subgroup (HR 0.48), as well
as in pts with MIBC with (HR 0.74) and without
prior NAC (HR 0.67). Safety was consistent with
previous data in ITT pts; no new safety signals
were identified.
---
[Slide 3]
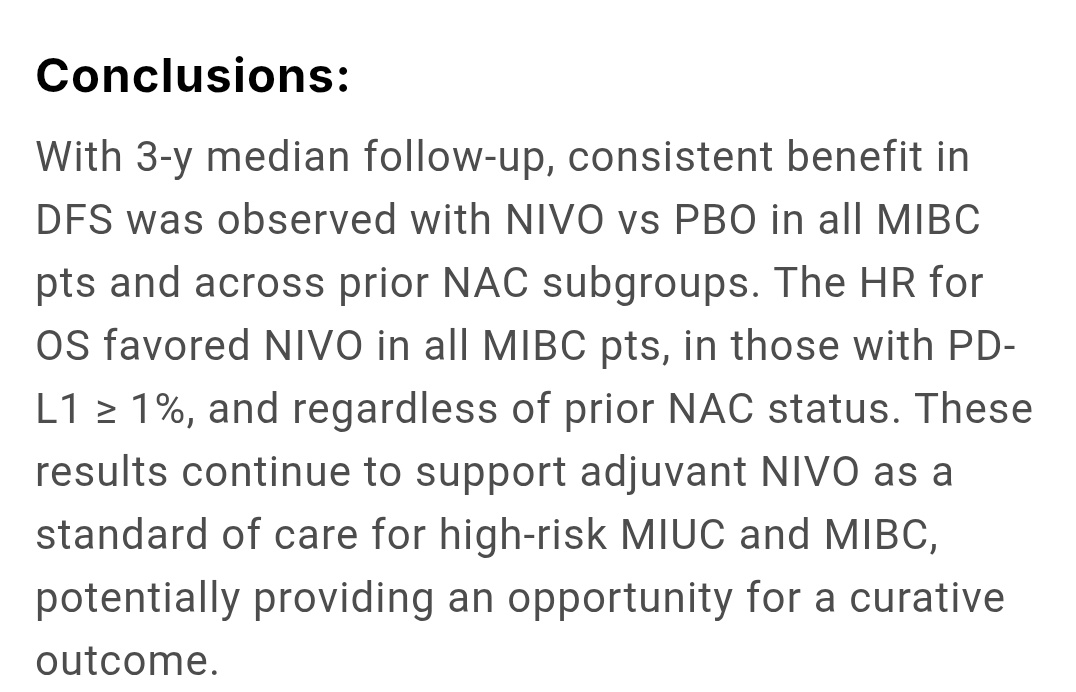
Conclusions:
With 3-y median follow-up, consistent benefit in
DFS was observed with NIVO vs PBO in all MIBC
pts and across prior NAC subgroups. The HR for
os favored NIVO in all MIBC pts, in those with PD-
L1 ≥ 1%, and regardless of prior NAC status. These
results continue to support adjuvant NIVO as a
standard of care for high-risk MIUC and MIBC,
potentially providing an opportunity for a curative
outcome.
Established adjuvant nivolumab as SOC for high-risk MIUC post-radical surgery. With NIAGARA now showing OS benefit with perioperative durvalumab in cisplatin-eligible MIBC, field is shifting to perioperative approach; CheckMate-274 remains relevant for cisplatin-ineligible patients, upper tract disease, or when neoadjuvant was declined/not feasible.
ITT population (primary analysis, NEJM 2021): median DFS 20.8 mo with nivolumab vs. 10.8 mo with placebo (HR 0.7, 98.22% CI 0.55-0.90, P<0.001). PD-L1 ≥1% subgroup: 55.5 vs. 8.4 mo (HR 0.55). 5-year update (Annals of Oncology 2026): median DFS 21.9 vs. 11.0 mo, HR 0.74 (95% CI 0.61-0.90).
First overall survival data from the 5-year follow-up (Galsky/Bajorin, Annals of Oncology, January 2026): median OS 75.0 months with nivolumab (95% CI 56.7-NE) vs. 50.1 months with placebo (38.0-72.1); HR 0.83 (95% CI 0.67-1.02). The 95% CI crosses unity — OS improvement is clinically meaningful (nearly 25 months absolute difference in medians) but did not reach conventional statistical significance in the hierarchical testing framework. DFS benefit remained durable alongside this OS signal.
Adverse events significant but manageable; consistent with the established nivolumab safety profile. Most common AEs: rash, fatigue, diarrhea, pruritus, musculoskeletal pain, urinary tract infection.
✅ Established adjuvant SOC for high-risk MIUC. Established adjuvant nivolumab as SOC for high-risk MIUC post-radical surgery. With NIAGARA now showing OS benefit with perioperative durvalumab in cisplatin-eligible MIBC, field is shifting to perioperative approach; CheckMate-274 remains relevant for cisplatin-ineligible patients, upper tract disease, or when neoadjuvant was declined/not feasible.