DESTINY-Breast05 is a Phase 3 trial of adjuvant trastuzumab deruxtecan (T-DXd, Enhertu) versus T-DM1 in high-risk HER2-positive early breast cancer with residual invasive disease after neoadjuvant therapy. T-DXd reduced the risk of invasive recurrence or death by 53% (iDFS HR 0.47; p<0.0001), with 3-year iDFS 92.4% versus 83.7%, supporting FDA approval on May 15, 2026. Sponsor: AstraZeneca / Daiichi Sankyo.
HER2+ Early Breast Cancer · Residual DiseaseTrastuzumab Deruxtecan (Enhertu)SABCS 2025 · NEJM 2026 · NCT04622319✓ FDA APPROVED MAY 15 2026
Design — Phase 3, open-label; adjuvant T-DXd (Enhertu) vs T-DM1 (Kadcyla), high-risk HER2+ early BC with residual invasive disease after neoadjuvant therapy (NCT04622319). (AstraZeneca)
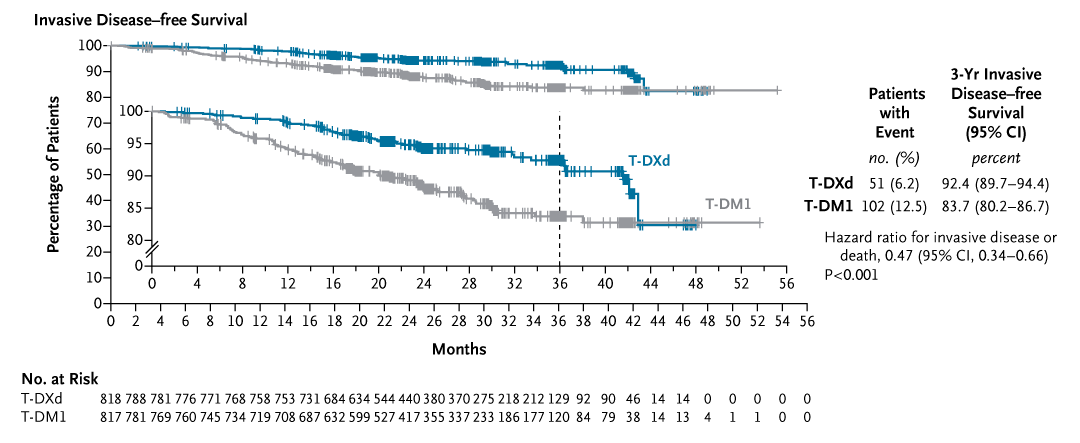
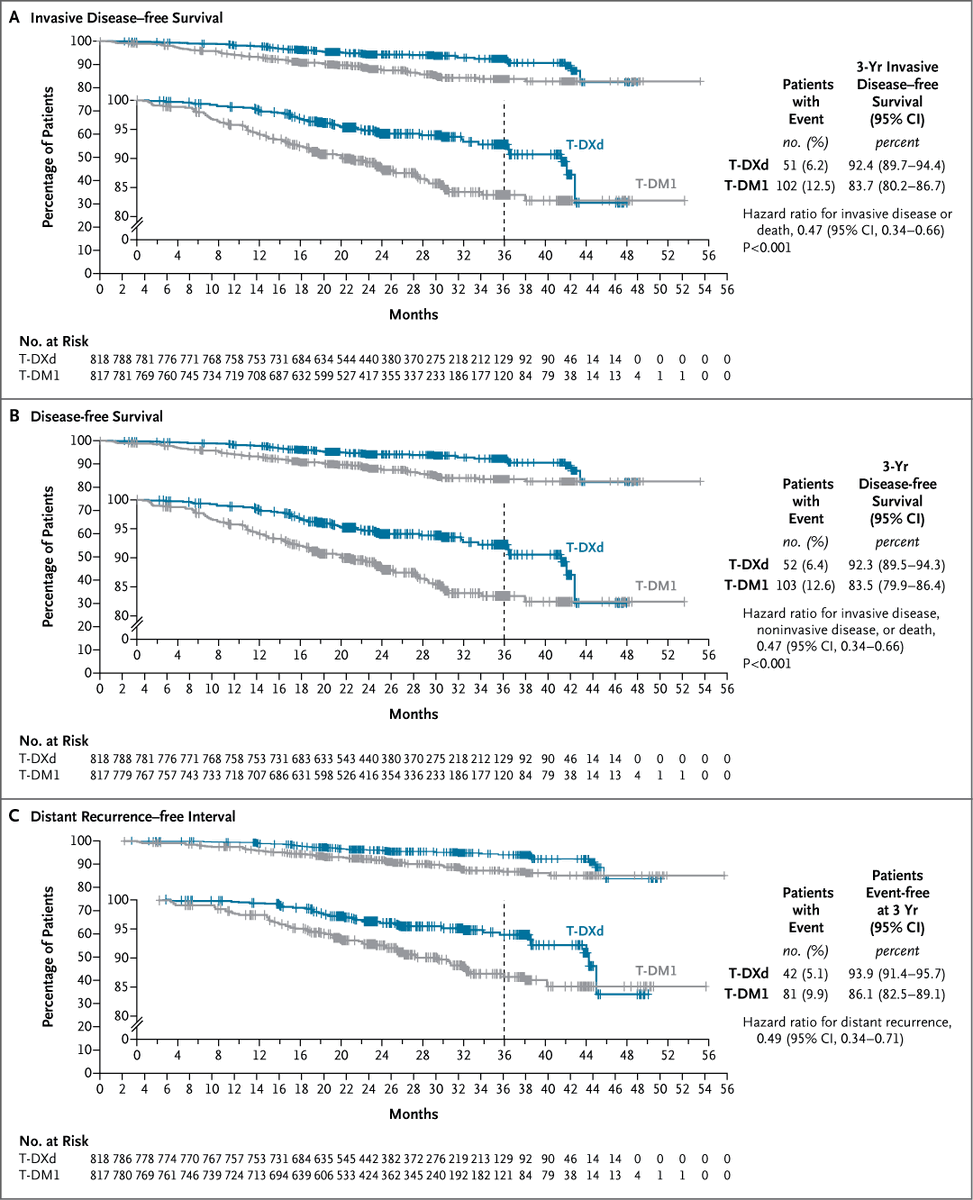
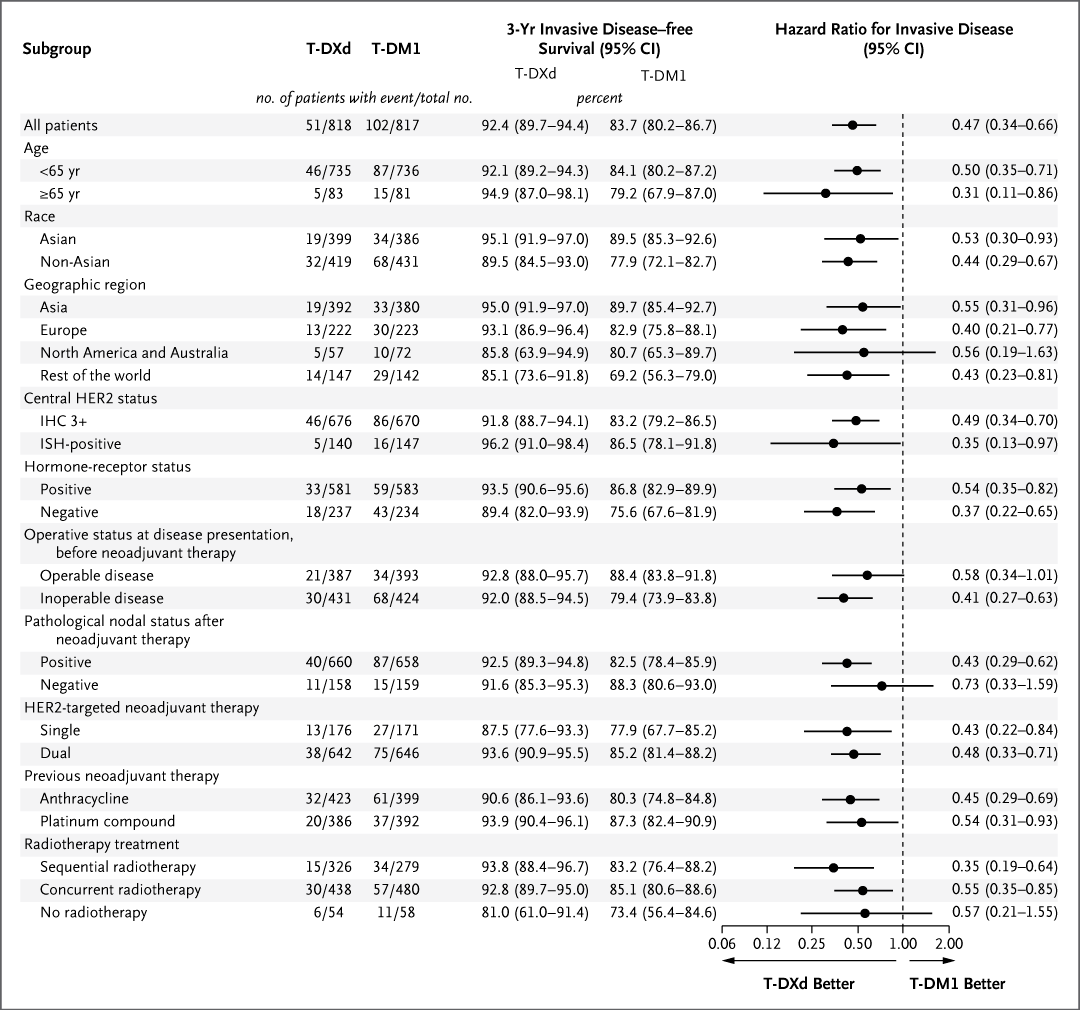
iDFS (primary) — HR 0.47 (95% CI 0.34-0.66; p<0.0001) — 53% reduction in invasive recurrence/death; median not reached; 3-year iDFS 92.4% vs 83.7%. (interim analysis)
Overall survival — Immature (2.9% maturity); OS HR 0.61 (95% CI 0.34-1.10); 3-year OS 97.4% vs 95.7%. (interim)
Safety — Grade >=3 AEs 50.6% vs 51.9%; adjudicated drug-related ILD/pneumonitis 9.6% with T-DXd (2 fatal events). (interim)
Regulatory — FDA approved May 15, 2026 via Project Orbis; dosing 5.4 mg/kg IV Q3W x14 cycles; boxed warning ILD & embryo-fetal toxicity. (FDA.gov)
Sponsor / Drug — AstraZeneca / Daiichi Sankyo; T-DXd (Enhertu), a HER2-directed antibody-drug conjugate. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.
Influence Leaders
Top KOL Voices on DESTINY-Breast 05
Santhosh Ambika
@RenoHemonc
12.5K impressions
Stephanie Graff, MD, FACP, FASCO
@DrSGraff
9.2K impressions
Abi Siva MD
@AbiSivaMD
7.3K impressions
Paolo Tarantino
@PTarantinoMD
6.4K impressions
Hope Rugo
@hoperugo
5.7K impressions
Oncology Brothers
@OncBrothers
4.2K impressions
Key Slides
SABCS 2025 / ESMO 2025 / NEJM 2026 Slides & Data
Conference slides shared by KOLs and presenters, with full OCR text available. All slides verified DESTINY-Breast 05 content.
[Slide 1]
16:30 - 18:15 Presidential Symposium |
CHAIRS: GIUSEPPE CURIGLIANO, BRIGETTE MA
FUTURE STUDIES NEEDED
HOW COULD WE INTEGRATE DB11 AND DB05?
Can we use a response-guided approach?
HP
pCR
X 14 cycles
ctDNA
cT≥3 or cN+
THP
Breast MRI
undetectable
Surgery
TDXd
HER2+ BC
x12 wks
(at C2D1)
response
RD
x14 cycles
Any HR status
Sara Tolaney
Check ctDNA:
If no response
Baseline &
Baseline breast MRI
Cycle Day 1
HP
Invited Discussant LBA1
for all patients
ctDNA
pCR
T-DXd for 4
X 14 cycles
Baseline tumor-informed
detectable
cycles
Surgery
ultrasensitive ctDNA for
(at C2D1)
RCB2/3
all patients
RD
ACx4-T-DM1x
Plasma samples for serial ctDNA testing
14 cycles
RCB1
"
"
T-DM1 X 14 cycles
Baseline
C2d1
(week 0)
(week 3)
Side adapted from Bia Sequi/Ada Waks
BERLIN AUDITORIUM - HUB 27
[Slide 1]
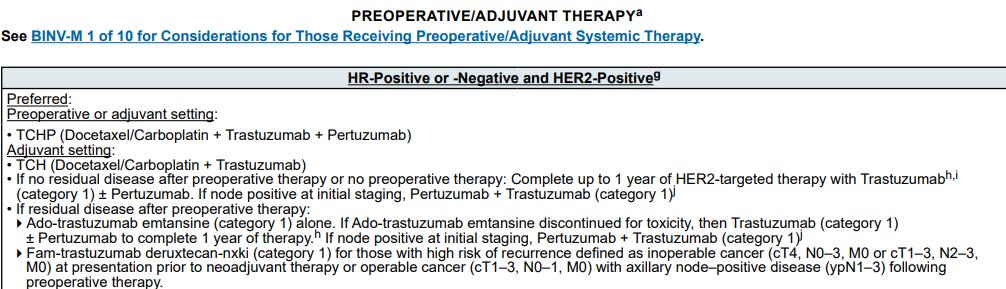
PREOPERATIVE/ADJUVANT THERAPY
See BINV-M 1 of 10 for Considerations for Those Receiving Preoperative/Adjuvant Systemic Therapy.
HR-Positive or -Negative and HER2-Positive9
Preferred:
Preoperative or adjuvant setting:
TCHP (Docetaxel/Carboplatin + Trastuzumab + Pertuzumab)
Adjuvant setting:
TCH (Docetaxel/Carboplatin + Trastuzumab)
If no residual disease after preoperative therapy or no preoperative therapy: Complete up to 1 year of HER2-targeted therapy with Trastuzumabh
(category 1) + Pertuzumab. If node positive at initial staging, Pertuzumab + Trastuzumab (category 1)
If residual disease after preoperative therapy:
Ado-trastuzumab emtansine (category 1) alone. If Ado-trastuzumab emtansine discontinued for toxicity, then Trastuzumab (category 1)
+ Pertuzumab to complete 1 year of therapy. If node positive at initial staging, Pertuzumab + Trastuzumab (category 1)J
Fam-trastuzumab deruxtecan-nxki (category 1) for those with high risk of recurrence defined as inoperable cancer (cT4, N0-3, M0 or cT1-3, N2-3,
M0) at presentation prior to neoadjuvant therapy or operable cancer (cT1-3, N0-1, M0) with axillary node-positive disease (ypN1-3) following
preoperative therapy.
[Slide 1]
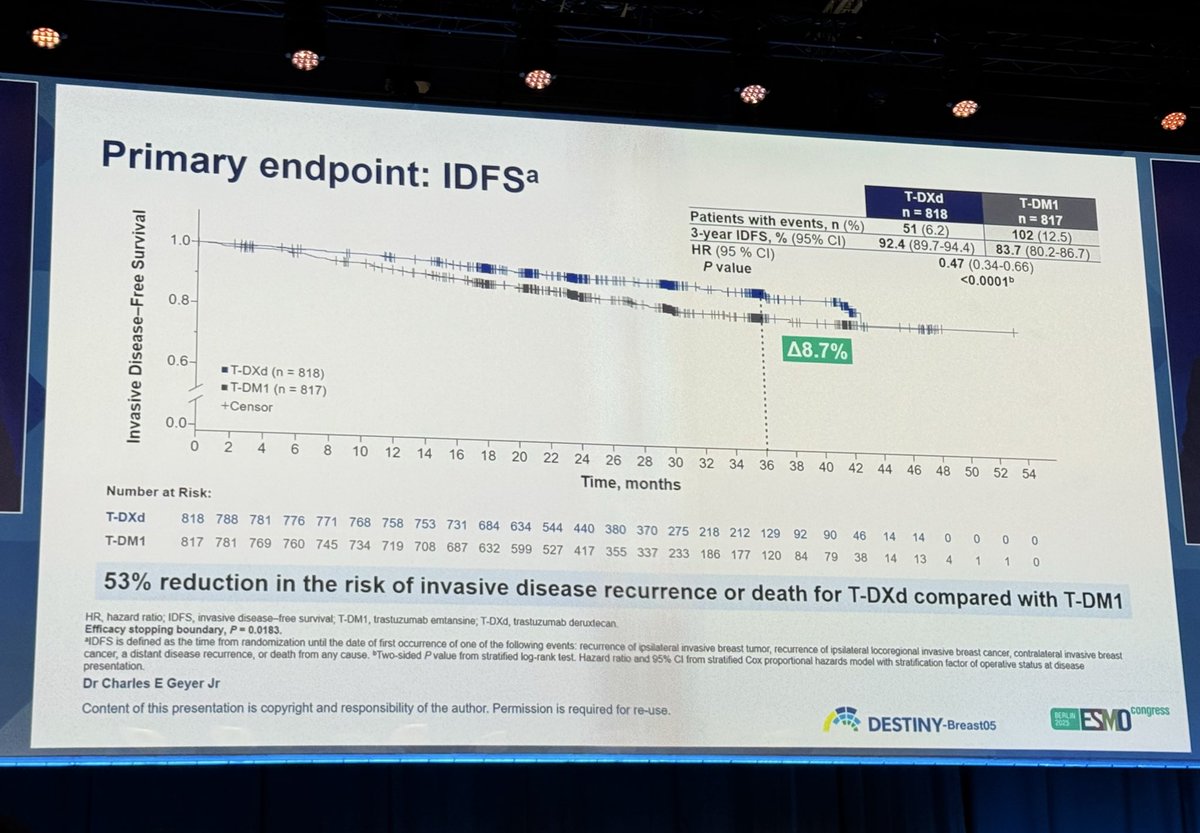
Primary endpoint: IDFSᵃ
T-DXd
T-DM1
n= 818
n= 817
Patients with events, n (%)
51 (6.2)
102 (12.5)
3-year IDFS, % (95% CI)
92.4 (89.7-94.4)
83.7 (80.2-86.7)
HR (95 % CI)
0.47 (0.34-0.66)
1.0
P value
<0.0001b
Invasive Disease-Free Survival
0.8
Д8.7%
0.6
T-DXd (n = 818)
T-DM1 (n = 817)
Censor
0.0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 54
Time, months
Number at Risk:
T-DXd 818 788 781 776 771 768 758 753 731 684 634 544 440 380 370 275 218 212 129 92 90 46 14 14 0 0 0 0
T-DM1 817 781 769 760 745 734 719 708 687 632 599 527 417 355 337 233 186 177 120 84 79 38 14 13 4 1 1 0
53% reduction in the risk of invasive disease recurrence or death for T-DXd compared with T-DM1
HR, hazard ratio; IDFS, invasive disease-free survival; T-DM1, trastuzumab emtansine; T-DXd, trastuzumab deruxtecan
Efficacy stopping boundary, P 0.0183.
MDFS is defined as the time from randomization until the date of first occurrence of one of the following events: recurrence of ipsilateral invasive breast tumor, recurrence of ipsilateral locoregional invasive breast cancer, contralateral invasive breast
cancer, a distant disease recurrence, or death from any cause. Two-sided Pvalue from stratified log-rank test. Hazard ratio and 95% CI from stratified Cox proportional hazards model with stratification factor of operative status at disease
presentation
Dr Charles E Geyer Jr
Content of this presentation is copyright and responsibility of the author. Permission is required for re-use.
BERLIN
DESTINY-Breast05
ESMO
congress
DESTINY-Breast 05 — Trastuzumab deruxtecan (T-DXd, Enhertu) vs. T-DM1 (Kadcyla)
DESTINY-Breast 05 is a phase 3, global, randomized, open-label trial evaluating T-DXd (Enhertu) vs. T-DM1 (Kadcyla) in adult patients with high-risk HER2-positive early breast cancer who have residual invasive disease following neoadjuvant therapy. The trial demonstrated a statistically significant and clinically meaningful improvement in invasive disease-free survival over T-DM1 (HR 0.47; 95% CI 0.34–0.66; P<0.0001). On May 15, 2026 — via FDA Project Orbis concurrent review — the FDA approved Enhertu in the adjuvant residual-disease setting (DB-05) and in the neoadjuvant setting for Stage II/III disease (DB-11), bringing T-DXd into the HER2+ curative-intent continuum. The FDA approval adds T-DXd as a new adjuvant option; T-DM1 retains its KATHERINE-based residual-disease indication on label. Investigators including Shanu Modi (MSK) describe T-DXd as a potential new standard of care in early-stage disease given its head-to-head superiority over T-DM1.
Enhertu (fam-trastuzumab deruxtecan-nxki) — approved May 15, 2026 — As adjuvant treatment of adult patients with HER2-positive (IHC 3+ or ISH+) breast cancer who have residual invasive disease following neoadjuvant trastuzumab (with or without pertuzumab) and taxane-based treatment.
Dosing: 5.4 mg/kg IV every 3 weeks for 14 cycles. Black-box warning: interstitial lung disease / pneumonitis and embryo-fetal toxicity.
✅ FDA-approved: DESTINY-Breast 05 adds T-DXd (Enhertu) as a new adjuvant option for adult patients with HER2-positive (IHC 3+ or ISH+) early breast cancer with residual invasive disease following neoadjuvant trastuzumab (±pertuzumab) plus taxane therapy. T-DM1 (Kadcyla) retains its existing KATHERINE-based indication on label; T-DXd does not formally replace it, but did demonstrate head-to-head superiority on iDFS in DB-05 and is positioned by investigators as a potential new standard of care. ✅ Companion approval: Via DESTINY-Breast 11 (same May 15, 2026 FDA action under Project Orbis), T-DXd → THP is also approved in the neoadjuvant setting for Stage II/III HER2+ disease. Together the two indications extend T-DXd across the HER2+ curative-intent continuum.
Study Design
Trial Methodology & Results
Study Design
Phase 3, randomized, open-label, multicenter, global trial; 1,635 patients randomized 1:1 to 14 cycles of either T-DXd or T-DM1.
Population
Adult patients with centrally confirmed HER2-positive (IHC 3+ or ISH+) early breast cancer with residual invasive disease in the breast and/or axillary nodes after neoadjuvant chemotherapy plus HER2-directed therapy — a high-risk-of-recurrence population.
Interventions
Intravenous T-DXd at 5.4 mg/kg every 3 weeks for 14 cycles versus intravenous T-DM1 at 3.6 mg/kg every 3 weeks for 14 cycles.
Median iDFS was NOT REACHED in both arms at interim analysis. T-DXd reduced the risk of invasive disease recurrence or death by 53% — HR 0.47 (95% CI 0.34–0.66; P<0.0001). The 3-year iDFS rate was 92.4% (T-DXd) vs. 83.7% (T-DM1). Distant disease recurrence risk fell 51% and brain metastasis risk fell 36% with T-DXd.
✓ iDFS HR 0.47 — 53% reduction in invasive recurrence/death
OS data was immature at the interim analysis (2.9% data maturity). OS hazard ratio was 0.61 (95% CI 0.34–1.10), 3-year OS 97.4% (T-DXd) vs. 95.7% (T-DM1). Final OS analysis pending.
DESTINY-Breast05 is a Phase 3, global, randomized, open-label trial (NCT04622319) of adjuvant trastuzumab deruxtecan (T-DXd, Enhertu) versus T-DM1 (Kadcyla) in adults with high-risk HER2-positive early breast cancer who have residual invasive disease after neoadjuvant therapy.
Is adjuvant T-DXd (Enhertu) FDA approved for HER2+ early breast cancer?
Yes. On May 15, 2026 the FDA approved Enhertu as adjuvant treatment of adults with HER2-positive (IHC 3+ or ISH+) breast cancer who have residual invasive disease following neoadjuvant trastuzumab (with or without pertuzumab) and taxane-based treatment, based on DESTINY-Breast05.
What were the DESTINY-Breast05 iDFS results?
Adjuvant T-DXd reduced the risk of invasive disease recurrence or death by 53% versus T-DM1 (invasive disease-free survival HR 0.47; 95% CI 0.34-0.66; p<0.0001). Median iDFS was not reached in either arm at interim analysis, and the 3-year iDFS rate was 92.4% with T-DXd versus 83.7% with T-DM1.
Is overall survival data mature in DESTINY-Breast05?
No. Overall survival data were immature at the interim analysis (about 2.9% maturity), with an OS hazard ratio of 0.61 (95% CI 0.34-1.10) and 3-year OS of 97.4% versus 95.7%. The final OS analysis is pending.
How is adjuvant Enhertu dosed and what are its warnings?
In DESTINY-Breast05 and the approved adjuvant indication, Enhertu is given at 5.4 mg/kg intravenously every 3 weeks for 14 cycles. It carries a boxed warning for interstitial lung disease/pneumonitis and embryo-fetal toxicity.