[Slide 1]
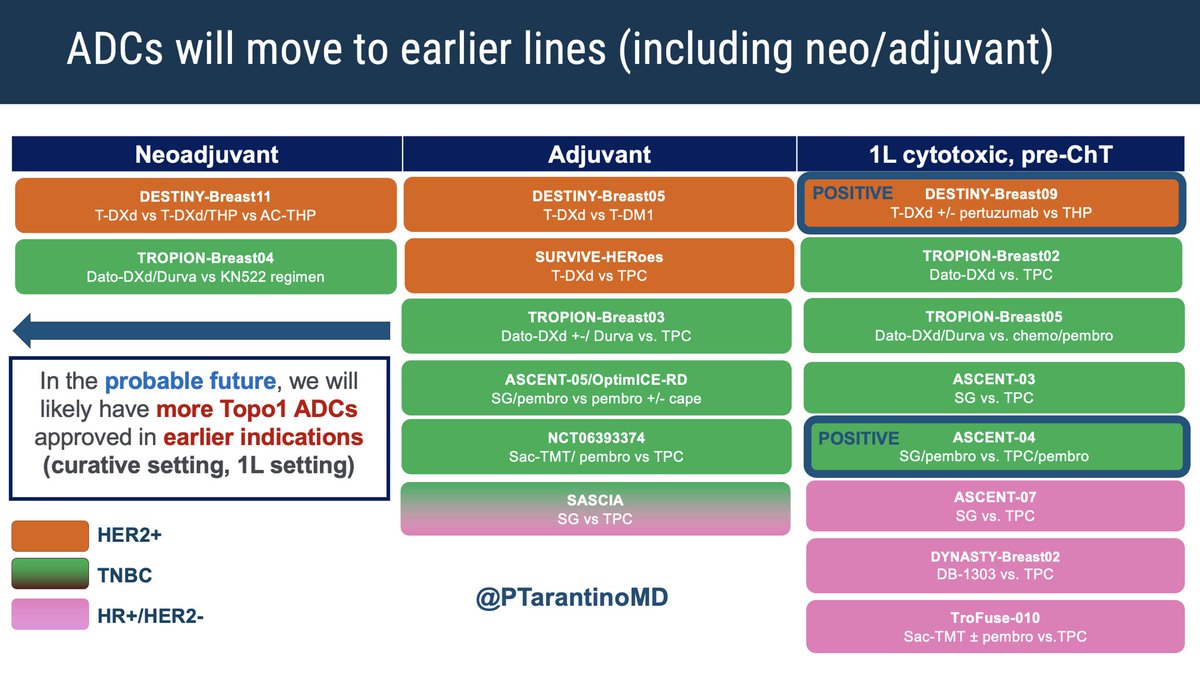
ADCs will move to earlier lines (including neo/adjuvant)
Neoadjuvant
Adjuvant
1L cytotoxic, pre-ChT
DESTINY-Breast11
DESTINY-Breast05
POSITIVE
DESTINY-Breast09
T-DXd vs T-DXd/THP vs AC-THP
T-DXd vs T-DM1
T-DXd +/- pertuzumab vs THP
TROPION-Breast04
SURVIVE-HERoes
TROPION-Breast02
Dato-DXd/Durva vs KN522 regimen
T-DXd vs TPC
Dato-DXd vs.TPC
TROPION-Breast03
TROPION-Breast05
Dato-DXd +-/Durvavs. TPC
Dato-DXd/Durva vs. chemo/pembro
In the probable future, we will
ASCENT-05/OptimICE-RD
ASCENT-03
SG/pembro vs pembro +/- cape
SG vs. TPC
likely have more Topo1 ADCs
approved in earlier indications
NCT06393374
POSITIVE
ASCENT-04
(curative setting, 1L setting)
Sac-TMT/ pembro vs TPC
SG/pembro vs. TPC/pembro
SASCIA
ASCENT-07
SG vs TPC
SG vs. TPC
HER2+
DYNASTY-Breast02
TNBC
DB-1303 vs. TPC
@PTarantinoMD
HR+/HER2-
TroFuse-010
Sac-TMT + pembro vs TPC
[Slide 1]
Summary:
T-DXd + P is a highly effective regimen in the 1L setting
Optimal sequencing remains unclear
Potential selection factors for 1L use of T-DXd + P:
Clinical: brain metastases, significant visceral disease, recent progression after (neo)adjuvant therapy
Biological: molecular markers of early progression (eg PIK3CAm), HER2 drivers (eg HER2DX
low/med ERBB2 score), dynamic markers (eg lack of early drop in ctDNA) - need to be further
validated
Patient preference
Could we achieve the same benefit with induction T-DXd + P till best response followed by
maintenance HP? -- paucity of data
Benefit of ET in maintenance phase in ER+ (PATINA)
Ongoing trials evaluating improving outcome with maintenance therapy - HER2CLIMB-05 (Tucatinib):
INAVO122 (Inavolisib for PIK3CAm)
2025
ASCO
#ASCO25
PRESENTED Claudine Isaacs MD FRCPC
ASCO
2025
ASCO
ANNUAL MEETING
[Slide 1]
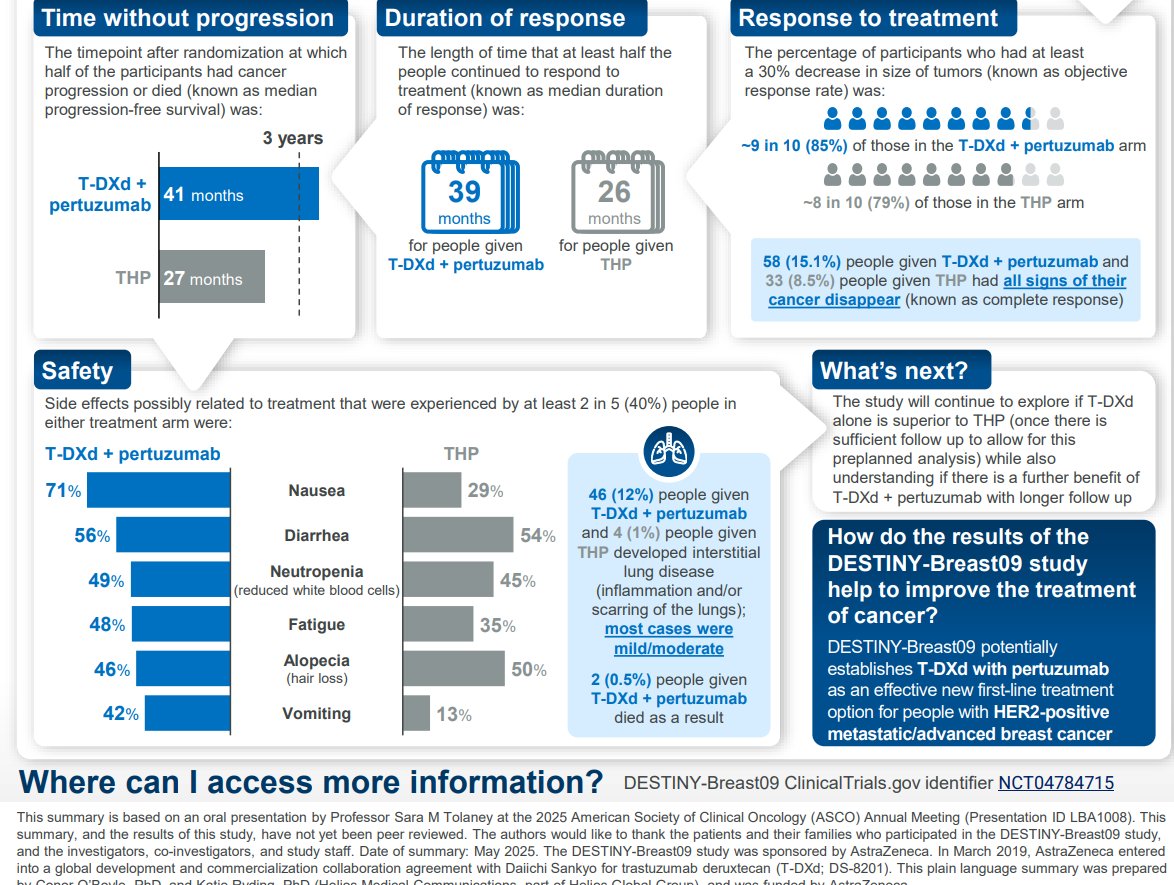
Time without progression
Duration of response
Response to treatment
The timepoint after randomization at which
The length of time that at least half the
The percentage of participants who had at least
half of the participants had cancer
people continued to respond to
a 30% decrease in size of tumors (known as objective
progression or died (known as median
treatment (known as median duration
response rate) was:
progression-free survival) was:
of response) was:
3 years
~9 in 10 (85%) of those in the T-DXd + pertuzumab arm
manan
T-DXd +
41 months
39
26
pertuzumab
~8 in 10 (79%) of those in the THP arm
months
months
for people given
for people given
T-DXd + pertuzumab
THP
58 (15.1%) people given T-DXd + pertuzumab and
THP
27 months
33 (8.5%) people given THP had all signs of their
cancer disappear (known as complete response)
Safety
What's next?
Side effects possibly related to treatment that were experienced by at least 2 in 5 (40%) people in
The study will continue to explore if T-DXd
either treatment arm were:
alone is superior to THP (once there is
T-DXd + pertuzumab
THP
OF
sufficient follow up to allow for this
preplanned analysis) while also
understanding if there is a further benefit of
71%
Nausea
29%
46 (12%) people given
T-DXd + pertuzumab with longer follow up
T-DXd + pertuzumab
56%
Diarrhea
54%
and 4 (1%) people given
How do the results of the
THP developed interstitial
49%
Neutropenia
lung disease
DESTINY-Breast09 study
45%
(reduced white blood cells)
(inflammation and/or
help to improve the treatment
scarring of the lungs);
of cancer?
48%
Fatigue
35%
most cases were
mild/moderate
DESTINY-Breast09 potentially
46%
Alopecia
50%
establishes T-DXd with pertuzumab
(hair loss)
2 (0.5%) people given
as an effective new first-line treatment
T-DXd + pertuzumab
42%
Vomiting
13%
died as a result
option for people with HER2-positive
metastatic/advanced breast cancer
Where can I access more information?
DESTINY-Breast09 ClinicalTrials.gov identifier NCT04784715
This
summary
is based on an oral presentation by Professor Sara M Tolaney at the 2025 American Society of Clinical Oncology (ASCO) Annual Meeting (Presentation ID LBA1008). This
summary, and the results of this study, have not yet been peer reviewed. The authors would like to thank the patients and their families who participated in the DESTINY-Breast09 study,
and the investigators, co-investigators, and study staff. Date of summary: May 2025. The DESTINY-Breast09 study was sponsored by AstraZeneca. In March 2019, AstraZeneca entered
into a global and commercialization collaboration agreement with Daiichi Sankyo deruxtecan (T-DXd; DS-8201). This plain language summary was prepared
---
[Slide 2]
What is the purpose of the DESTINY-Breast09 study?
DESTINY
Breast09
Trastuzumab deruxtecan (T-DXd) is a recommended treatment for
DESTINY-Breast09 is a clinical study of adults
people whose breast cancer has a high level of the human epidermal
who were given T-DXd alone, T-DXd + pertuzumab,
growth factor receptor 2 protein (known as 'HER2-positive') and if the
or THP as the first treatment for their HER2-positive
cancer cells cannot be completely removed with surgery and have spread
metastatic/advanced breast cancer.
from where they started (known as metastatic/advanced cancer).
T-DXd can currently only be given to these people if their breast cancer
The study was designed to find out how well T-DXd
has worsened (known as disease progression) while receiving the first
worked with or without pertuzumab in delaying disease
recommended treatment, which is a combination of a chemotherapy drug
progression as compared with THP. The study also
and two HER2-targeting drugs, known as THP (taxane + trastuzumab
assessed the side effects participants experienced when
+ pertuzumab).
receiving these treatments.
What did the study show?
This planned analysis of DESTINY-Breast09 showed that participants in the T-DXd + pertuzumab arm lived longer without their
disease
growing, spreading, or getting worse compared with participants in the THP (taxane + trastuzumab + pertuzumab) arm.
Side effects of the treatments were manageable and as expected based on results of previous studies.
How was the DESTINY-Breast09 study carried out?
Start of study
People included in the study had:
383 people were randomly assigned to
Metastatic/advanced breast cancer
T-DXd + pertuzumab
2 drugs
Start of
HER2+
HER2-positive tumors
treatment*
387 people were randomly assigned to
eeen
No prior chemotherapy or HER2-targeted
THP (taxane + trastuzumab + pertuzumab)
therapy for metastatic/advanced breast cancer
taxane options = paclitaxel or docetaxel
3 drugs
One prior endocrine-based therapy for
*At the time of this first analysis, the T-DXd alone arm remained blinded;
metastatic/advanced breast cancer (optional)
this will be evaluated at a subsequent analysis
[Slide 1]
DESTINY-Breast09
Conclusions
T-DXd + P demonstrated a statistically significant and clinically
meaningful PFS benefit by BICR vs THP, which was consistently
observed across subgroups
PFS by BICR
- Hazard ratio of 0.56 vs THP (P<0.00001)
- Median PFS was 40.7 months (T-DXd + P) vs 26.9 months (THP)
44%
Median DOR of >3 years with T-DXd + P. with CRs in 15.1% (T-DXd + P)
Reduction in risk of
vs 8.5% (THP)
disease progression
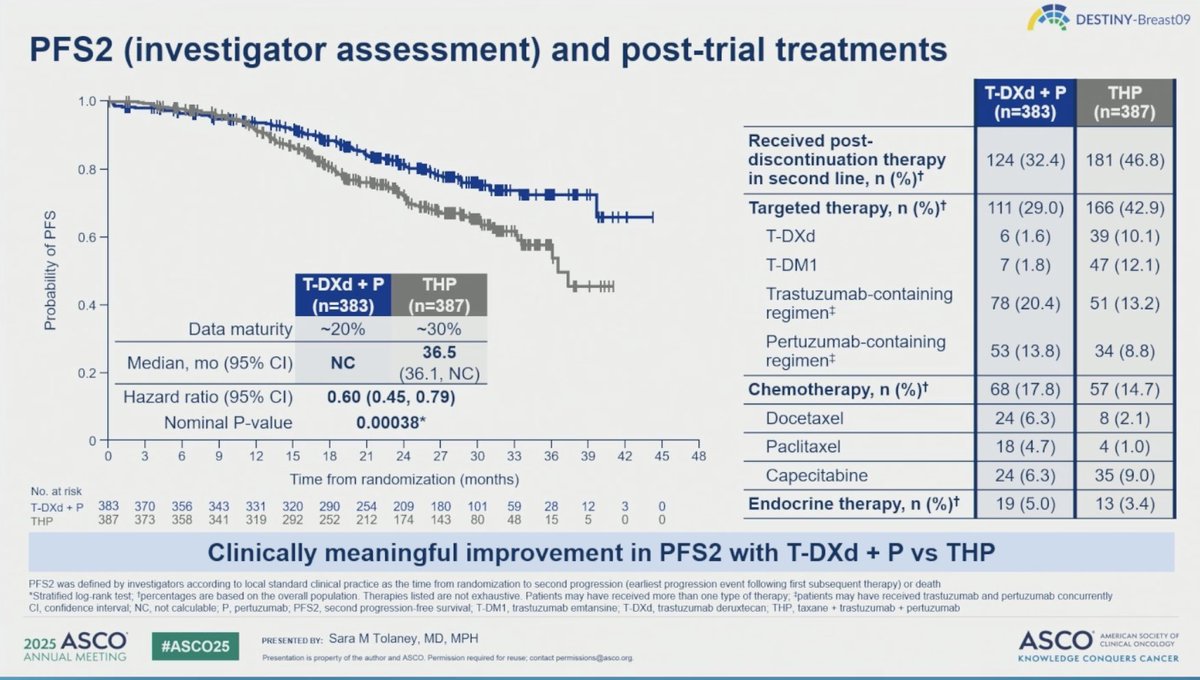
Early os data suggest a positive trend favoring T-DXd + P.
or death with
with a supportive hazard ratio of 0.60 for PFS2
T-DXd + P vs THP
T-DXd + P safety data were consistent with known profiles of
individual treatments
T-DXd + P demonstrated a statistically significant and clinically meaningful
PFS benefit vs THP and may represent a new first-line standard of care
for patients with HER2+ a/mBC
been
DICR
blended
DOR
duction
of
response
human
updermal
growth
factor
incapital
3
positive
os
perfurume
ASCO
Tolaney
MPH
2025
#ASCO25
ASCO
MEETING
KNOWLEDGE CONQUERS CANCER
2025
ASCO
ANNUAL MEETING
[Slide 1]
Enhertu plus pertuzumab
demonstrated highly
statistically significant
and clinically meaningful
improvement in
progression-free survival
US. THP as 1st-line
therapy for patients with
HER2-positive metastatic
breast cancer
---
[Slide 2]
DESTINY-Breast09 Phase III trial of
AstraZeneca and Daiichi Sankyo's
Enhertu is the first trial in more than a
decade to demonstrate superior efficacy
across a broad HER2-positive metastatic
patient population versus current 1st-line
standard of care
Positive high-level results from a planned interim
analysis of the DESTINY-Breast09 Phase III trial
showed Enhertu (trastuzumab deruxtecan) in
combination with pertuzumab demonstrated a highly
statistically significant and clinically meaningful
improvement in progression-free survival (PFS)
compared to a taxane, trastuzumab and pertuzumab
(THP) as a 1st-line treatment for patients with HER2-
positive metastatic breast cancer.
The PFS improvement was seen across all pre-
specified patient subgroups with Enhertu in
combination with pertuzumab. The key secondary
endpoint of overall survival (OS) was not mature at the
time of this planned interim analysis; however, interim
os data showed an early trend favouring the Enhertu
combination compared with THP.
The second arm assessing Enhertu monotherapy
versus THP remains blinded to patients and
investigators and will continue to the final PFS analysis.
HER2-positive metastatic breast cancer is an
aggressive disease driven by overexpression or
amplification of HER2 affecting 15-20% of patients with
metastatic breast cancer. 1 While HER2-targeted
therapies have improved outcomes, prognosis remains
poor, with most patients experiencing disease
progression within two years of 1st-line treatment with
THP, which has are for more
[Slide 1]
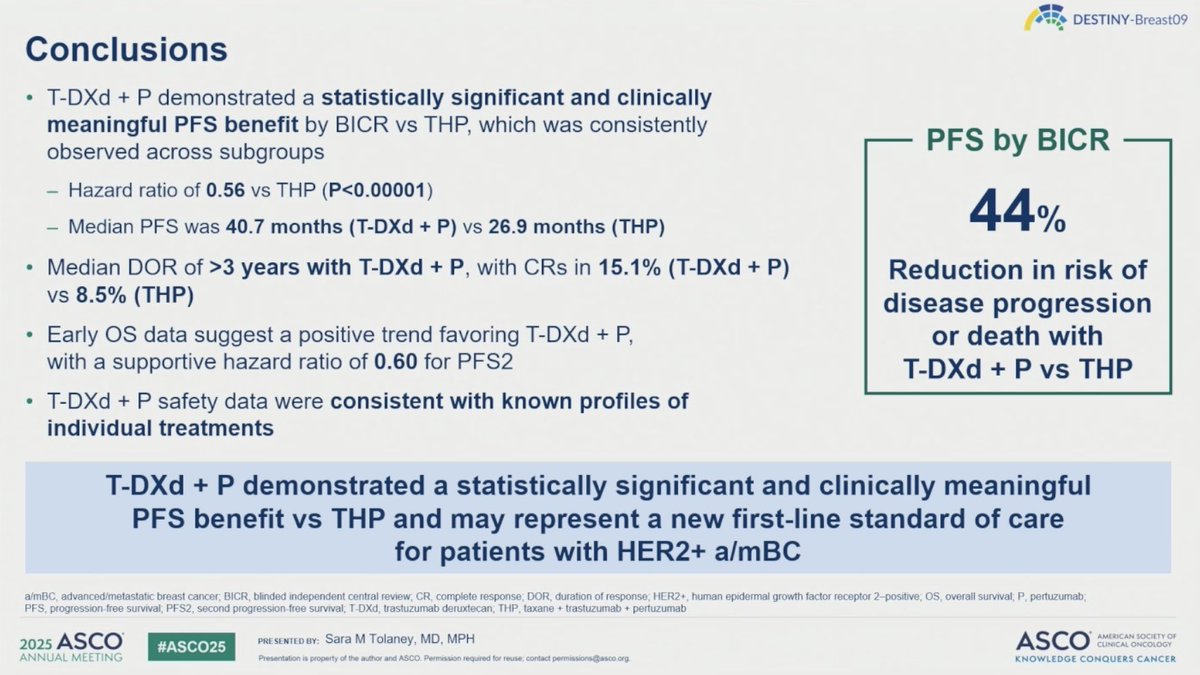
DESTINY-Breast09
Conclusions
T-DXd + P demonstrated a statistically significant and clinically
meaningful PFS benefit by BICR vs THP, which was consistently
observed across subgroups
PFS by BICR
- Hazard ratio of 0.56 vs THP (P<0.00001)
- Median PFS was 40.7 months (T-DXd + P) VS 26,9 months (THP)
44%
Median DOR of >3 years with T-DXd + P, with CRs in 15.1% (T-DXd + P)
Reduction in risk of
vs 8.5% (THP)
disease progression
Early os data suggest a positive trend favoring T-DXd + P,
or death with
with a supportive hazard ratio of 0.60 for PFS2
T-DXd + P vs THP
T-DXd + P safety data were consistent with known profiles of
individual treatments
T-DXd + P demonstrated a statistically significant and clinically meaningful
PFS benefit vs THP and may represent a new first-line standard of care
for patients with HER2+ a/mBC
a/mBC, advanced/molastatic breast cancer; BICR, blinded independent central review CR complete response DOR duration of response HER2 human epidermal growth factor reception 2-positive, OS, overall survival P. portuzumab
PFS, progression free survival PFS2, second progression-free survival, T-DXd, trashizumab deruxtecan, THP, laxane . trastuzumeb . partzzumab
2025 ASCO
PRESENTED OT Sara M Tolaney, MD, MPH
ASCO
MERICAN SOCIETY
#ASCO26
CLINICAL ONCOLO
ANNUAL MEETING
Preservation . property of the author and ASCO
KHCWLEDGE CONQUERS CANC
[Slide 1]
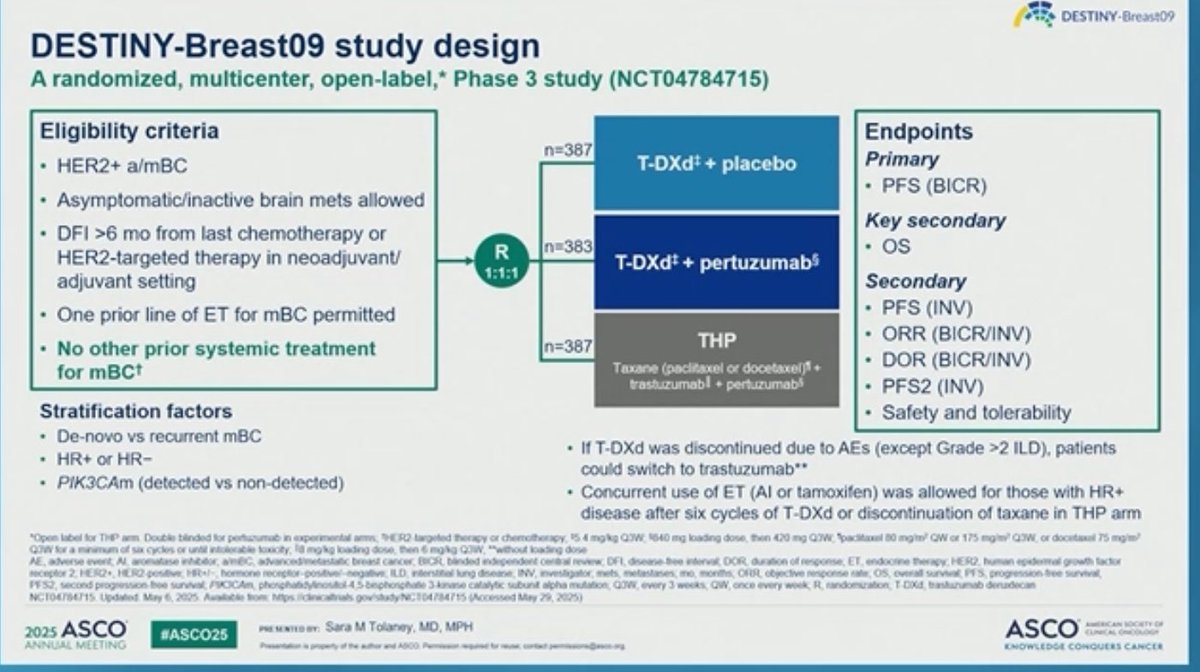
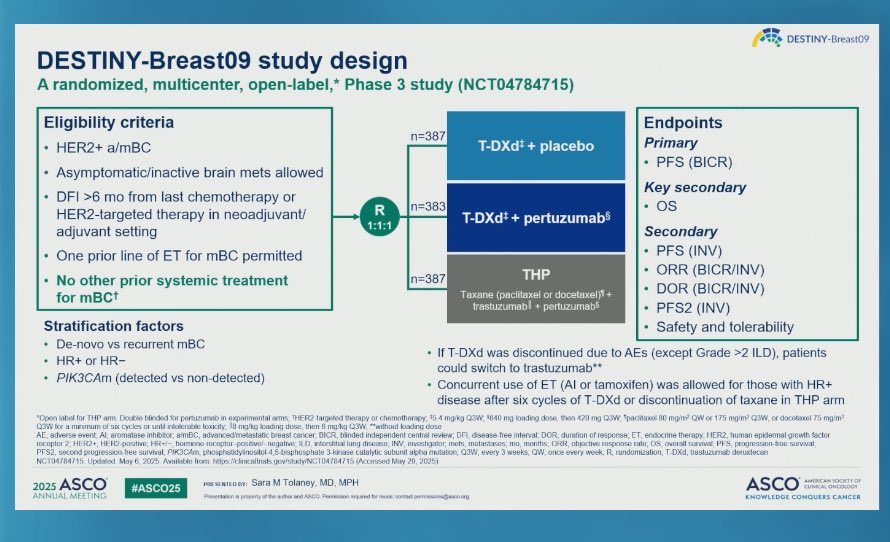
DESTINY-Breast09
DESTINY-Breast09 study design
A randomized, multicenter, open-label,* Phase 3 study (NCT04784715)
Eligibility criteria
Endpoints
n=387
HER2+ a/mBC
T-DXd + placebo
Primary
PFS (BICR)
Asymptomatic/inactive brain mets allowed
Key secondary
DFI >6 mo from last chemotherapy or
R
n=383
os
HER2-targeted therapy in neoadjuvant/
adjuvant setting
1:1:1
T-DXd + pertuzumab
Secondary
One prior line of ET for mBC permitted
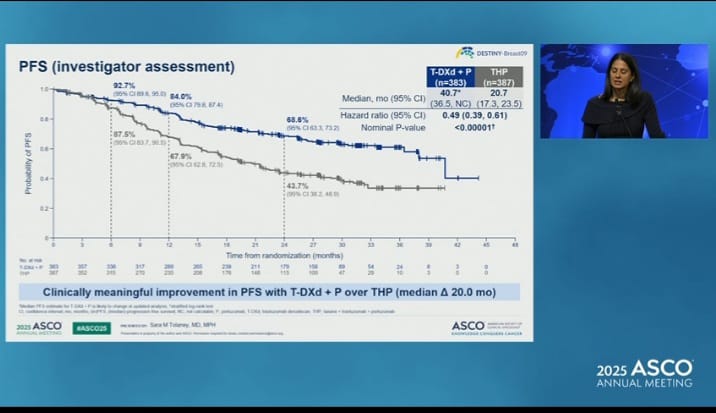
PFS (INV)
No other prior systemic treatment
THP
ORR (BICR/INV)
n=387
for mBC
Taxane (paclitaxel or docetaxel)
DOR (BICR/INV)
trastuzumabl + pertuzumabl
PFS2 (INV)
Stratification factors
Safety and tolerability
De-novo vs recurrent mBC
HR+ or HR-
If T-DXd was discontinued due to AEs (except Grade >2 ILD), patients
could switch to trastuzumab**
PIK3CAm (detected vs non-detected)
Concurrent use of ET (AI or tamoxifen) was allowed for those with HR+
disease after six cycles of T-DXd or discontinuation of taxane in THP arm
"Open THP arm Double blinded for pertuzumeb experimental arms THER2 targeted therapy chemotherapy 4 mgkg Q3W 1840 mg loading dose then 420 mg Q3W pacitaxel 80 mg/m? ow or 175 mg/m2 Q3W or docetaxel 75 mg/m2
Q3W
of
SDX
cycles
or
until
lg
loading
dose
then
dose
AE
DEL disease free interval DOR duration of response ET. endocrine therapy HER2 human epidemal growth factor
mets metastases mo months ORR objective response rate OS overall survival PFS progression froo survival
Q3W. every 3 weeks QW. once every week R randomization T-DXd. trastuzumab deruxlecan
NCT04784715 Updated Mar 6 2025 Available from helps 2025)
2025 ASCO
#ASCO25
Sara M Tolaney MD MPH
ASCO
AMERICAN SOCIETY or
CLINICAL ONCOLDON
ANNUAL MEETING
.
KNOWLEDGE CONQUERS CANCER
---
[Slide 2]
DESTINY-Brea
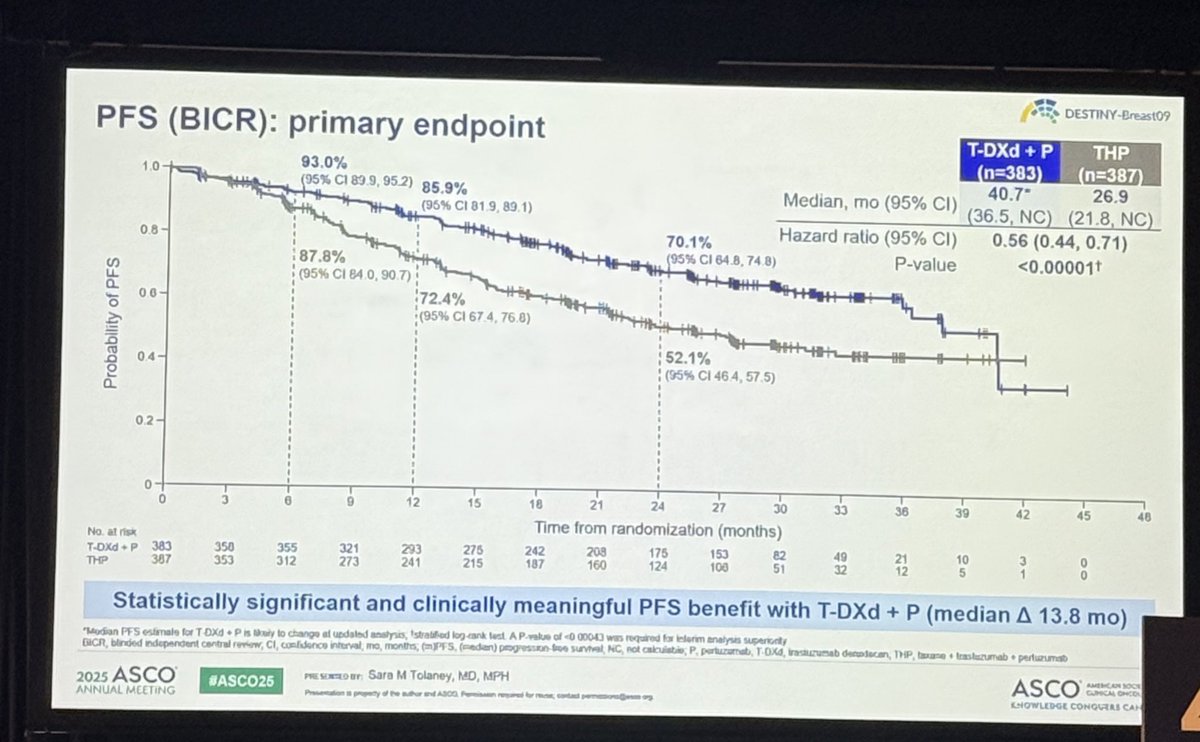
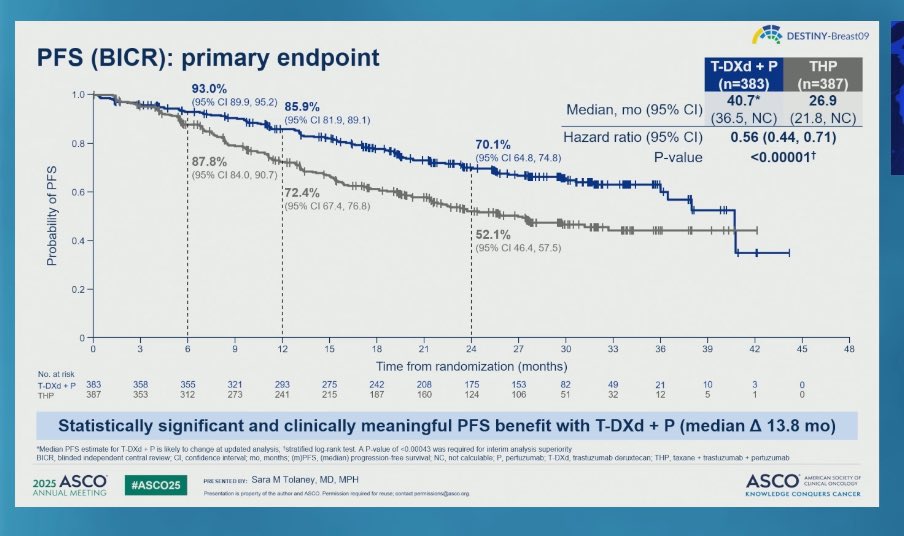
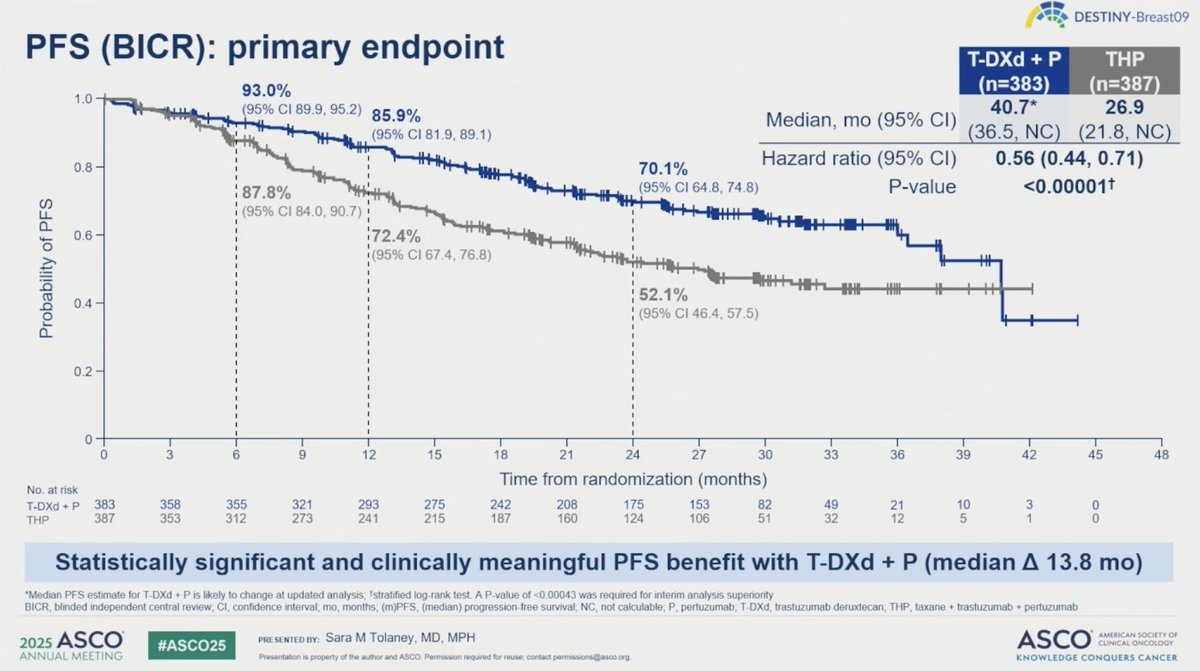
PFS (BICR): primary endpoint
T-DXd + P
THP
93.0%
(n=383)
(n=387)
1.0
-
(95% CI 89.9 95.2)
85.9%
40.7*
26.9
Median, mo (95% CI)
(95% CI 81.9. 89.1)
(36.5, NC)
(21.8, NC
0.8
70.1%
Hazard ratio (95% CI)
0.56 (0.44, 0.71)
87.8%
(95% CI 64.8, 74.8)
P-value
<0.00001
(95% CI 84.0. 90.7)
0.6
72.4%
(95% CI 67.4 76.8)
+
52.1%
0.4
(95% CI 46.4, 57.5)
0.2
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
Time from randomization (months)
No. at risk
T-DXd
383
358
355
321
293
275
242
208
175
153
82
49
21
10
3
0
THP
387
353
312
273
241
215
187
160
124
106
51
32
12
5
1
0
Statistically significant and clinically meaningful PFS benefit with T-DXd + P (median A 13.8 mo)
"Median PFS estimate for T-DXd P is likely to change at updated analysis 'stratified log rank test A P value of <0.00043 was required for interim analysis superiority
BICR blinded independent central review CI confidence interval mo months (mJPFS (median) progression tree survival NG, not calculable T DXd trastuzumati deruxtecan THP taxane . trastuzumat . partuzumab
2025 ASCO
Pid
SENTED
#ASCO25
Sara M Tolaney MD. MPH
ASCO
AMERICAN SOCIETY
CUNICAL ONCOLD
ANNUAL MEETING
Presentation
.
KNOWLEDGE CONQUERS CANC
---
[Slide 3]
DESTINY-Breast09
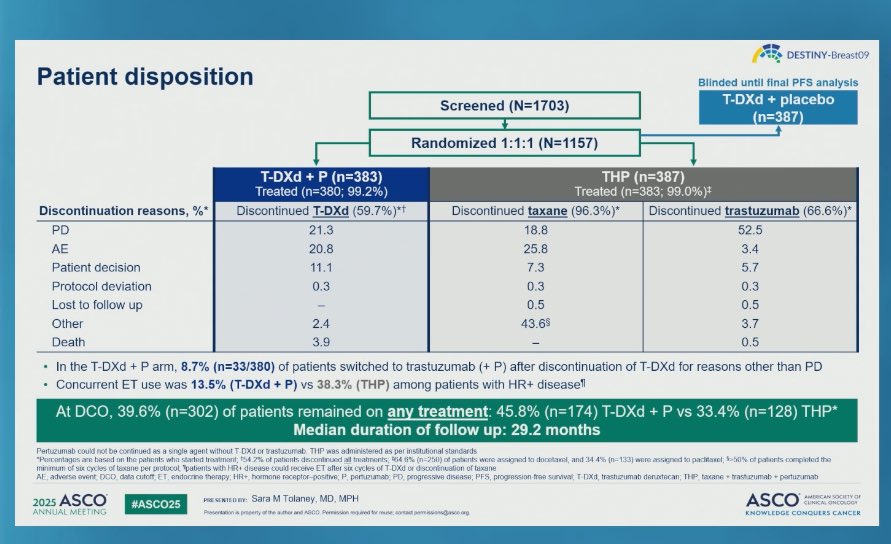
Patient disposition
Blinded until final PFS analysis
Screened (N=1703)
T-DXd + placebo
(n=387)
,
Randomized 1:1:1 (N=1157)
T-DXd + P (n=383)
THP (n=387)
Treated (n=380; 99.2%)
Treated (n=383; 99.0%)
Discontinuation reasons, %*
Discontinued T-DXd (59.7%)*
Discontinued taxane (96.3%)*
Discontinued trastuzumab (66.6%)*
PD
21.3
18.8
52.5
AE
20.8
25.8
3.4
Patient decision
11.1
7.3
5.7
Protocol deviation
0.3
0.3
0.3
Lost to follow up
-
0.5
0.5
Other
2.4
43,6
3.7
Death
3.9
-
0.5
In the T-DXd + P arm, 8.7% (n=33/380) of patients switched to trastuzumab (+ P) after discontinuation of T-DXd for reasons other than PD
Concurrent ET use was 13.5% (T-DXd + P) vs 38.3% (THP) among patients with HR+ disease"
At DCO, 39.6% (n=302) of patients remained on any treatment: 45.8% (n=174) T-DXd + P vs 33.4% (n=128) THP*
Median duration of follow up: 29.2 months
Pertuzumab could not be continued as a single agent without T DX4 or trastuzumab THP was administered as per institutional standards
"Percentages are based on the patients who started treatment 154 2% of patients discontinued all treatments 964 0% (n=250) of patients were assigned to docetaxol and 34 4% (n=133) were assigned to pacificate) 15-50% of patients completed the
minimum of Six cycles of texase per protocol patients with HR+ disease could receive ET after Six cycles of T-DXd of discontinuation of tuxune
AE adverse event DCD data outoff ET endocrine therapy HR+ hormone receptor-positive P. pertuzumab PD progressive disease; PFS progression from survival T DXd trastuzumati denutecan THP taxane trastuzumab pertuzumati
2025 ASCO
PRE SENTED
#ASCO25
Sara M Tolaney MD. MPH
ASCO
AMERICAN SOCIETY or
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation . property of the author and A800 Permission required to reuse contact permissions@asco.or
KNOWLEDGE CONQUERS CANCER
[Slide 1]
DESTINY-Breast09
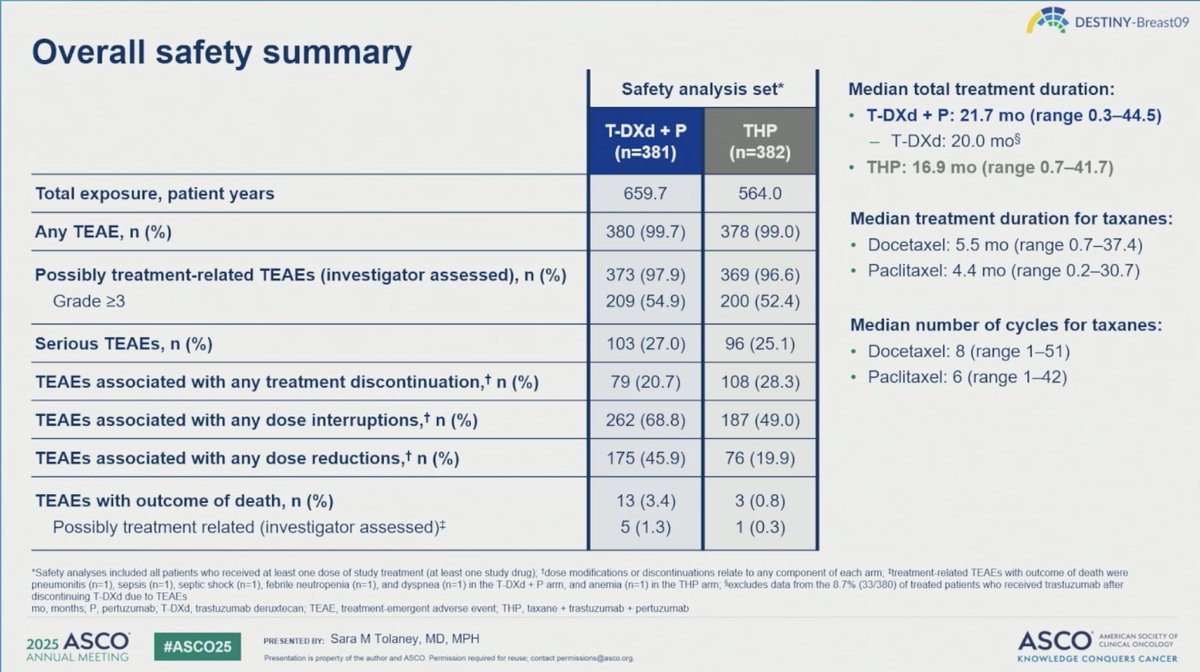
Overall safety summary
Safety analysis set*
Median total treatment duration:
T-DXd + P: 21.7 mo (range 0.3-44.5)
T-DXd + P
THP
- T-DXd: 20.0 mos
(n=381)
(n=382)
THP: 16.9 mo (range (0.7-41.7)
Total exposure, patient years
659,7
564.0
Median treatment duration for taxanes:
Any TEAE, n (%)
380 (99.7)
378 (99.0)
Docetaxel: 5.5 mo (range (0.7-37.4)
Possibly treatment-related TEAEs (investigator assessed), n (%)
373 (97.9)
369 (96.6)
Paclitaxel: 4.4 mo (range 0.2-30.7)
Grade >3
209 (54.9)
200 (52.4)
Median number of cycles for taxanes:
Serious TEAEs, n (%)
103 (27.0)
96 (25.1)
Docetaxel: 8 (range 1-51)
TEAEs associated with any treatment discontinuation, n (%)
79 (20.7)
108 (28.3)
Paclitaxel: 6 (range 1-42)
TEAEs associated with any dose interruptions, n (%)
262 (68.8)
187 (49.0)
TEAEs associated with any dose reductions, n (%)
175 (45.9)
76 (19.9)
TEAEs with outcome of death, n (%)
13 (3.4)
3 (0.8)
Possibly treatment related (investigator assessed)
5 (1.3)
1 (0.3)
"Safety analyses included all patients who received at least one dose of study treatment (at least one study drug); 'dose modifications or discontinuations relate to any component of each arm. Itreatment-related TEAEs with outcome of death were
pneumonitis (n=1), sepsis (n=1), septic shock (n=1), febrile neutropenia (n=1), and dyspnea (n=1) in the T-DXd P arm, and anemia (n=1) in the THP arm excludes data from the 8.7% (33/380) of treated patients
who
received
trastuzumab
after
discontinuing T-DXd due to TEAEs
mo months P. pertuzumab; T-DXd. trastuzumab deruxtecan; TEAE treatment-emergent adverse event THP, taxane + trastuzumab . pertuzumab
2025 ASCO
PRE SENTED
BY: Sara M Tolaney, MD. MPH
ASCO
AMERICAN SOCIETY OF
#ASCO25
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse contact permissions@asco.
KNOWLEDGE CONQUERS CANCER
DESTINY-Breast09 is a clinical trial evaluating Trastuzumab deruxtecan (T-DXd) + pertuzumab in 1L HER2+ metastatic breast cancer. Sponsored by Daiichi Sankyo / AstraZeneca. KOL discussion spans multiple conferences with 106 tracked posts from 54 oncology opinion leaders generating 504.4K total impressions.
FDA APPROVED Enhertu (fam-trastuzumab deruxtecan-nxki) + Perjeta (pertuzumab) — First-line treatment of adults with unresectable or metastatic HER2-positive (IHC 3+ or ISH+) breast cancer
On December 15, 2025, the FDA approved fam-trastuzumab deruxtecan-nxki (Enhertu) in combination with pertuzumab for 1L HER2+ metastatic breast cancer. Approval based on DESTINY-Breast09 (NCT04784715) demonstrating PFS HR 0.56, median PFS 40.7 vs 26.9 months (p<0.0001). FDA also co-approved the PATHWAY anti-HER-2/neu (4B5) Rabbit Monoclonal Primary Antibody as companion diagnostic.
Phase 3, randomized (1:1:1), three-arm, multicenter trial comparing T-DXd (5.4 mg/kg) plus pertuzumab versus taxane plus trastuzumab plus pertuzumab (THP) in treatment-naive HER2-positive advanced/metastatic breast cancer.
Population
Adults with HER2-positive (IHC 3+ or ISH+) unresectable or metastatic breast cancer with no prior chemotherapy or HER2-targeted therapy for advanced disease. A single prior line of endocrine therapy was permitted.
Interventions
Fam-trastuzumab deruxtecan-nxki (Enhertu) 5.4 mg/kg IV every 3 weeks plus pertuzumab versus taxane (docetaxel or paclitaxel) plus trastuzumab plus pertuzumab (THP).
Primary Endpoints
Primary: progression-free survival (PFS) by blinded independent central review (BICR). Key secondary: overall survival (OS), confirmed objective response rate (ORR).