











Top 10 by impressions - click to view on X
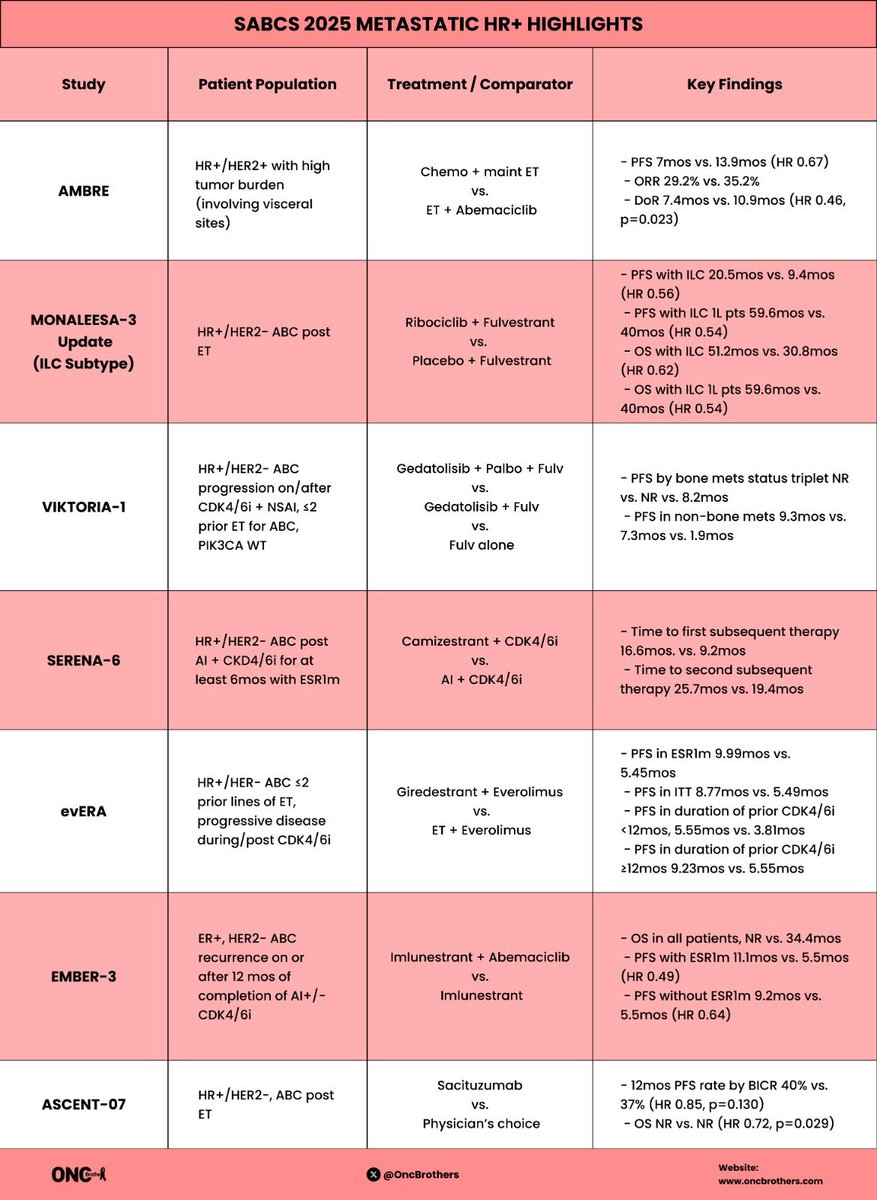
A lot was covered but summary of 7 main studies we touched on during Metastatic HR+ #BreastCancer #SABCS highlights w/ @hoperugo: ✅...
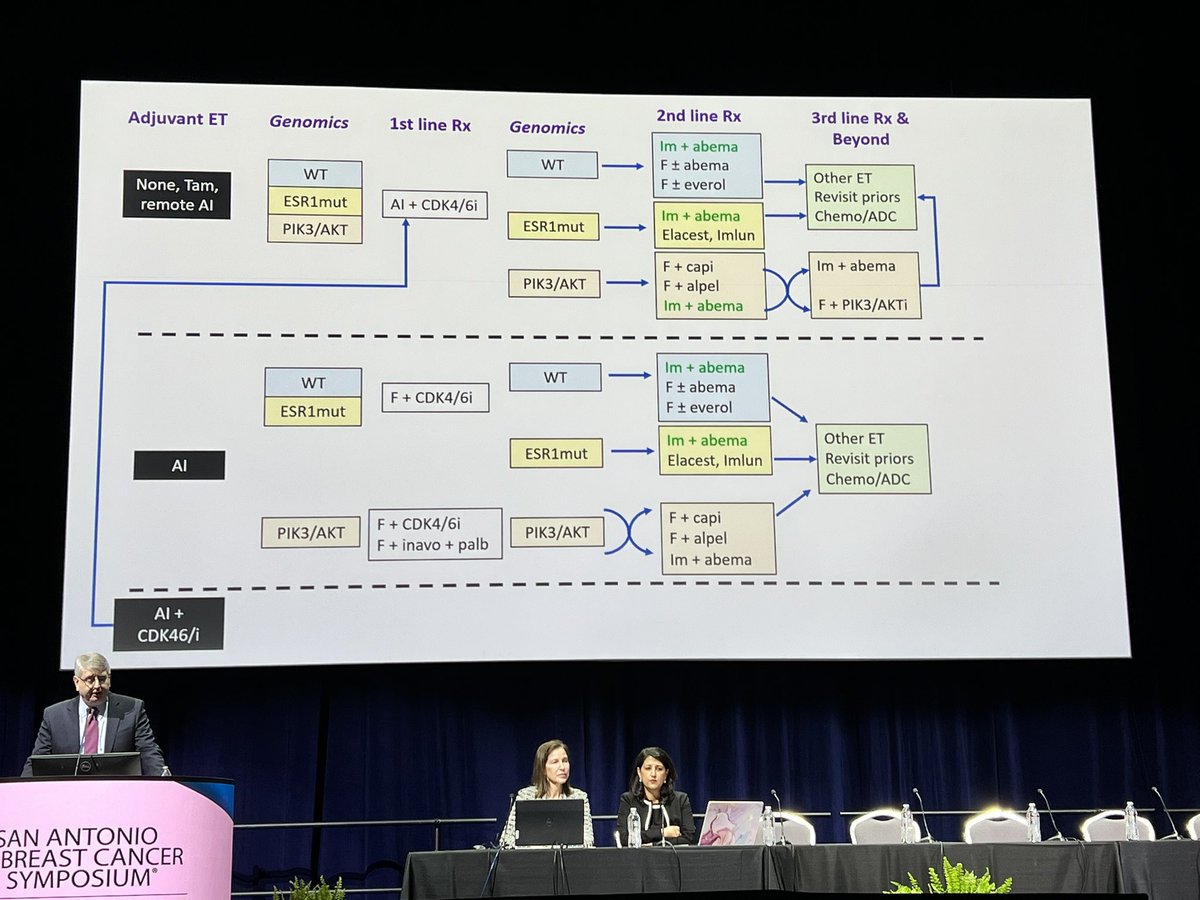
The new #Halgorithm for treating HR+/HER2- metastatic breast cancer @DrHBurstein @SABCSSanAntonio @DFCI_BreastOnc #bcsm...
Metastatic HR+ #BreastCancer #SABCS highlights w/ @hoperugo: ✅ #AMBRE ✅ #MONALEESA ✅ #VIKTORIA1 ✅...
#SABCS2025 Honored to present this exciting data. Efficacy seen regardless of mESR1 or mPIK3CA with ela+eve. Data immature for abema. EVERA also shows benefit with giredestrant/EVE...
#ESMOBreast25 is in 5 Days! One of the key upcoming presentations: EMBER-3 Subgroup Analysis 📌Imlunestrant + abema improved PFS after CDK4/6i (vs. Imlu) 📌No abema benefit after...
#SABCS24 Part 2: Highlights w/ @jamecancerdoc ✅ #EUROPA ✅ #TAILORx ✅ #PADMA ✅ #EMBER3 Full 📢: ...
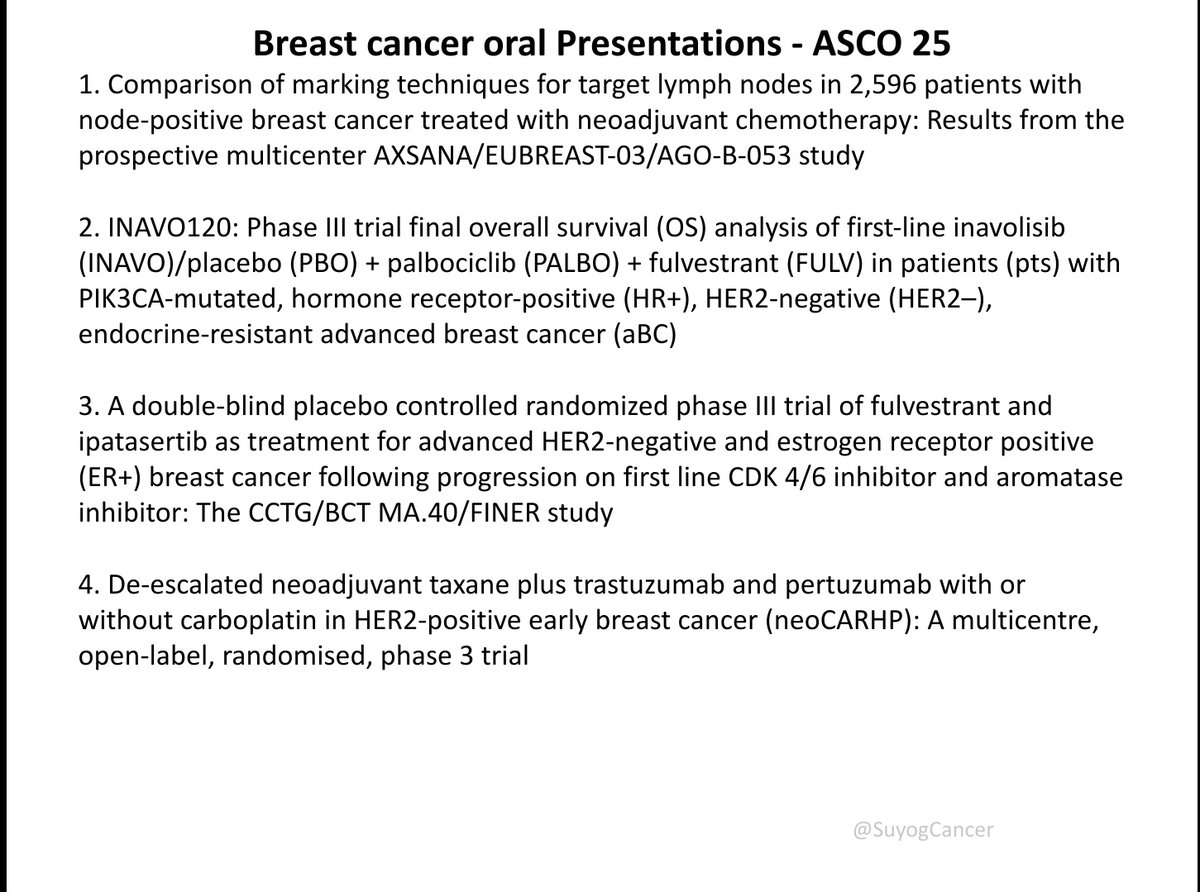
key oral abstracts in breast cancer from #ASCO25 Covering neoadjuvant, adjuvant & metastatic settings: INAVO120, EMBER-3, VERITAC-2, DESTINY-Breast06, AXSANA, I-SPY2...

Ember 3 updated results. Imlu maintaining benefit. Combo benefit similar to evera trial although here benefit regardless of esr1m. Would love to see the combo approved to allow us more options for...
#SABCS24 beautiful discussion by @DrHBurstein on EMBER3. One of the best!! A fabulous and well qualified accumulation of data attached. Wow. @OncoAlert

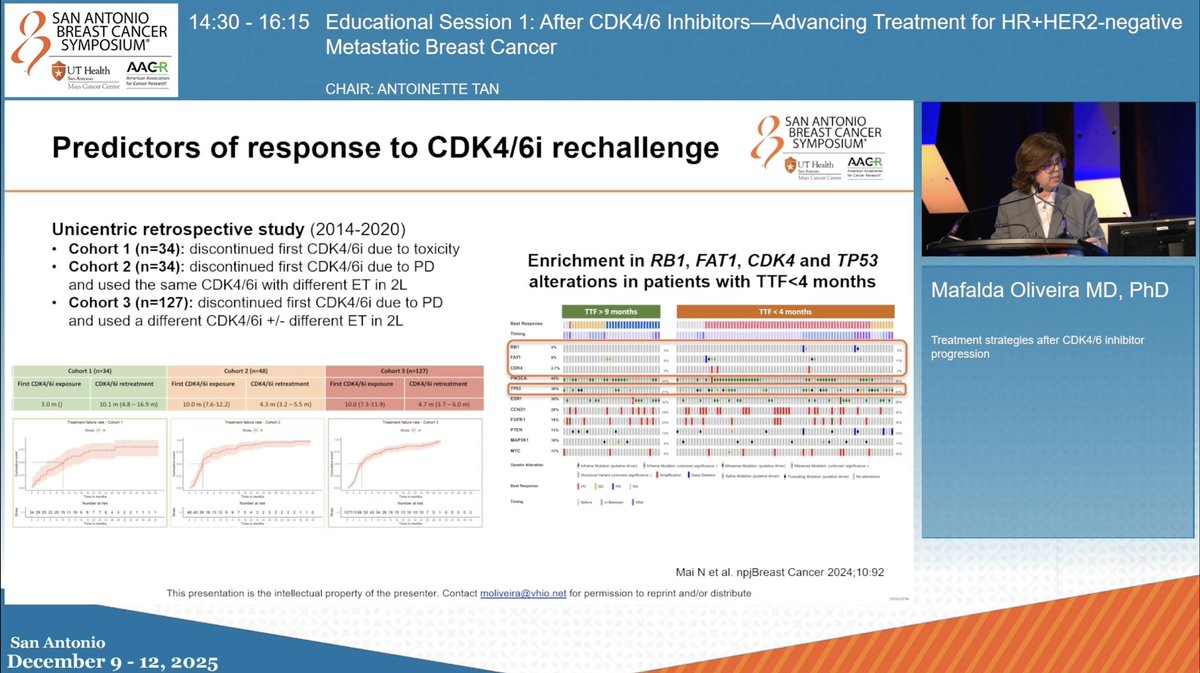
📌 Educational Session 1: After CDK4/6 Inhibitors-Advancing Treatment for HR+HER2-negative Metastatic Breast Cancer ✨Treatment strategies after CDK4/6 inhibitor progression Mafalda Oliveira at...
EMBER-3 is a Phase III, randomized, open-label trial that evaluated imlunestrant (Inluriyo), a next-generation oral selective estrogen receptor degrader (SERD), in patients with ER-positive, HER2-negative advanced or metastatic breast cancer previously treated with endocrine therapy. The trial randomized 874 patients 1:1:1 to imlunestrant monotherapy (400 mg daily), investigator's choice of endocrine therapy (fulvestrant or exemestane), or imlunestrant plus abemaciclib. Imlunestrant demonstrated a statistically significant PFS improvement in the ESR1-mutant subgroup, leading to FDA approval in September 2025 as the second oral SERD for ESR1-mutated advanced breast cancer.
Phase III, global, open-label, 1:1:1 randomized trial in patients with ER+/HER2- locally advanced or metastatic breast cancer whose disease progressed on an aromatase inhibitor with or without a CDK4/6 inhibitor. ESR1 mutational status was determined by blood ctDNA analysis using the Guardant360 CDx assay. Randomization was stratified by prior CDK4/6 inhibitor use, presence of visceral metastases, and geographic region.
874 adult patients (men and pre/postmenopausal women) with ER+/HER2- advanced or metastatic breast cancer who progressed on prior aromatase inhibitor therapy with or without a CDK4/6 inhibitor. Approximately 37% had ESR1 mutations, 38% had PI3K pathway mutations, 60% had received prior CDK4/6 inhibitor therapy, 32% enrolled as first-line for metastatic disease, and 64% as second-line. Patients eligible for PARP inhibitors were excluded.
Imlunestrant 400 mg orally once daily versus investigator's choice of fulvestrant 500 mg IM or exemestane 25 mg daily. A third arm evaluated imlunestrant 400 mg daily plus abemaciclib 150 mg twice daily (added via protocol amendment).
Primary endpoints: investigator-assessed PFS of imlunestrant vs SOC in ESR1-mutant patients, imlunestrant vs SOC in all patients, and imlunestrant plus abemaciclib vs imlunestrant alone in all patients. Key secondary endpoint: overall survival (tested sequentially if PFS was significant). Other endpoints included ORR, time to chemotherapy, PFS2, and patient-reported outcomes.
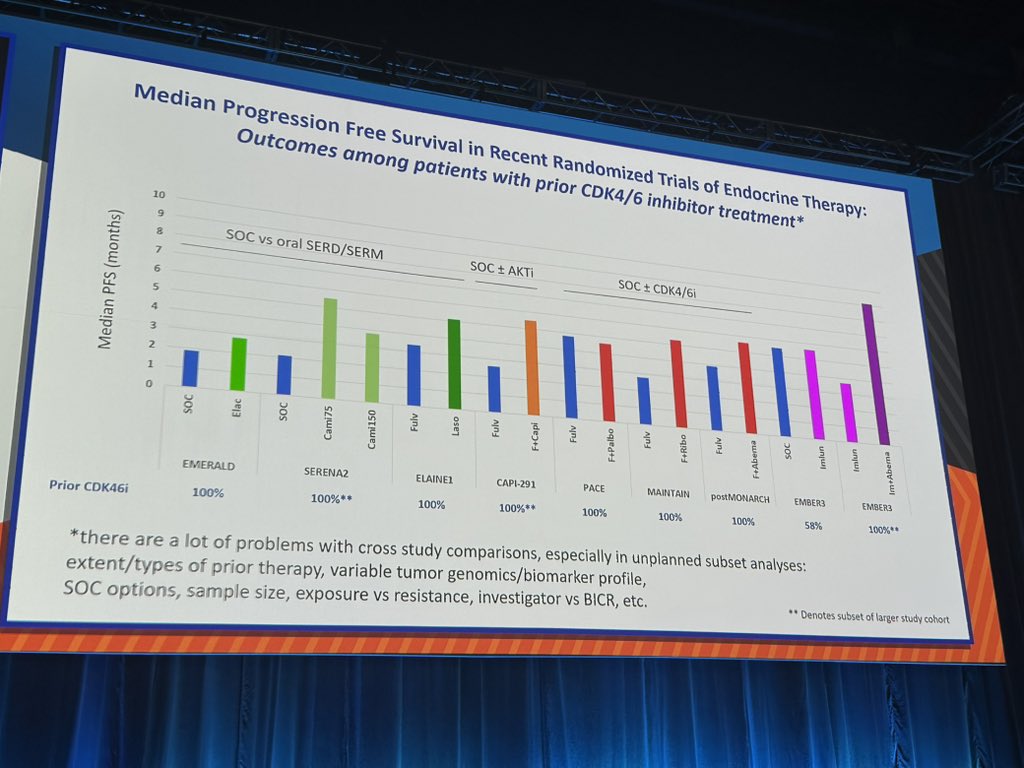
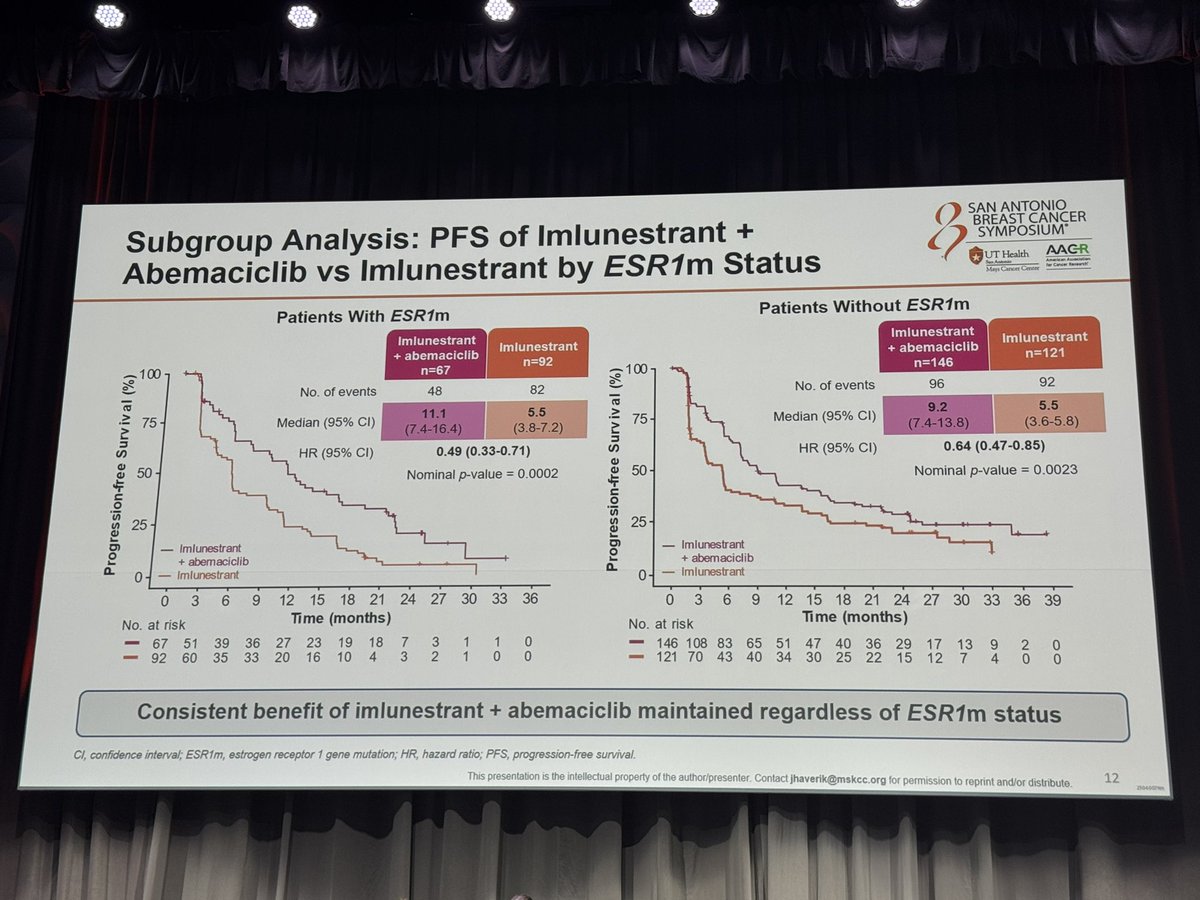
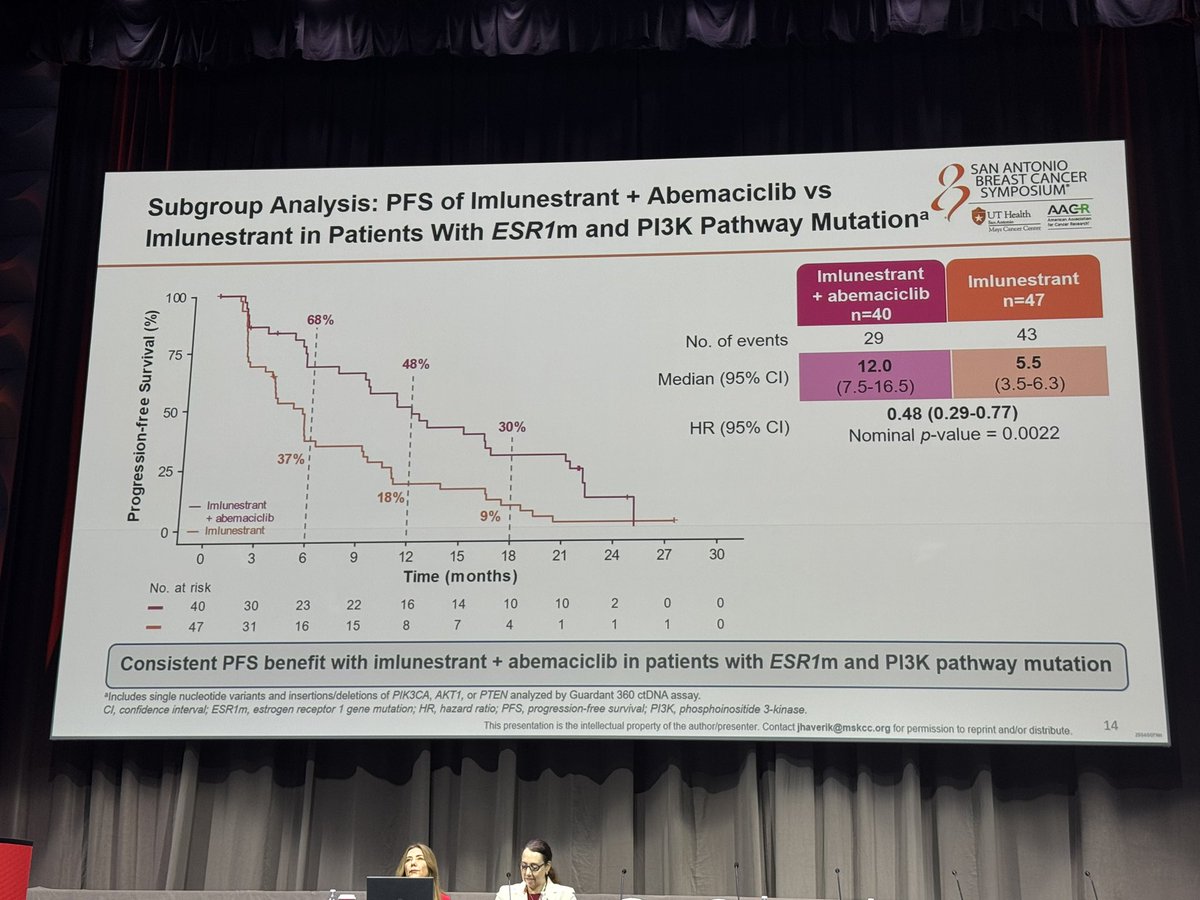
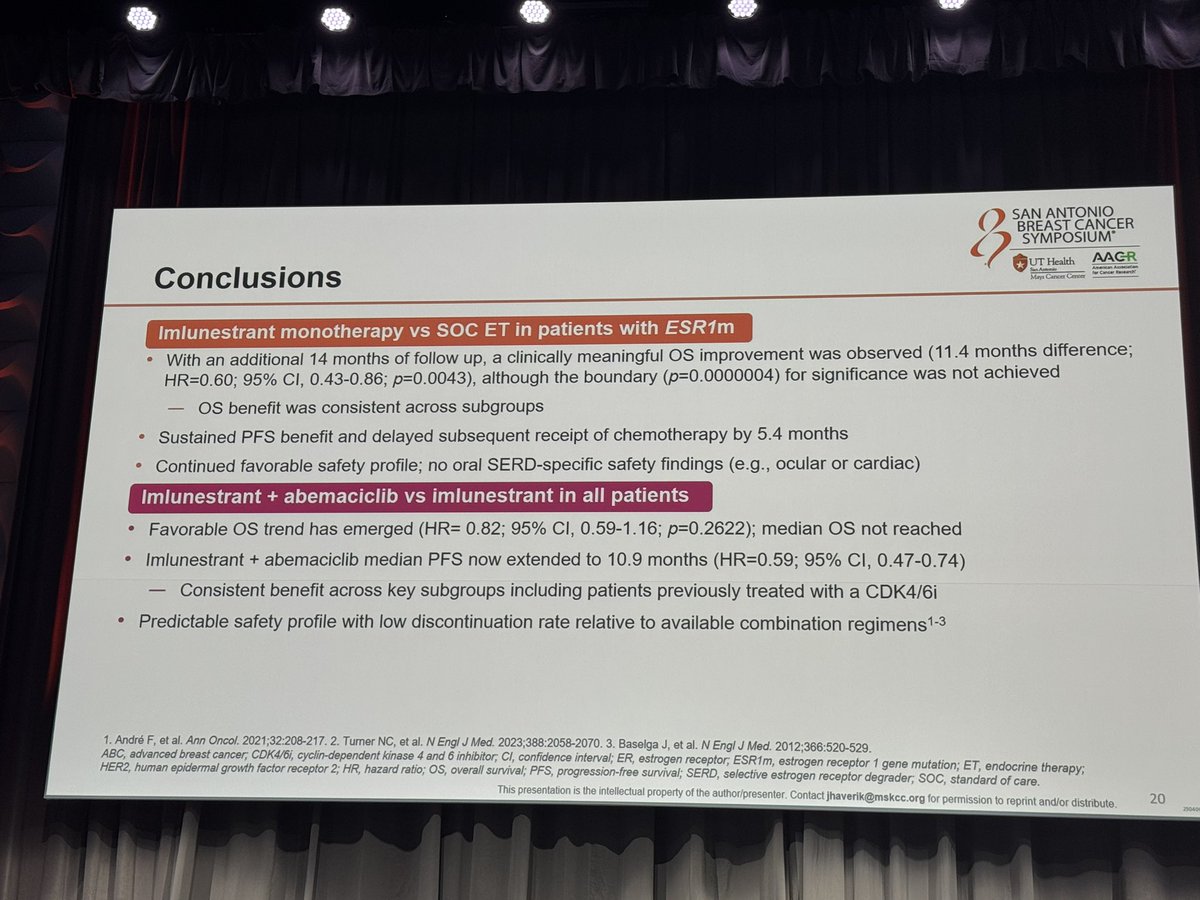
In the ESR1-mutant population (n=256), imlunestrant demonstrated median PFS of 5.5 months (95% CI: 3.9-7.4) vs 3.8 months (95% CI: 3.7-5.5) for physician's choice, with HR 0.62 (95% CI: 0.46-0.82; p=0.0008), a 38% reduction in risk of progression or death. PFS in the ITT overall population was not statistically significant. The imlunestrant plus abemaciclib combination achieved median PFS of 10.9 months vs 5.5 months for imlunestrant alone (updated HR 0.59; 95% CI: 0.47-0.74; p<0.0001), with benefit regardless of ESR1 status.
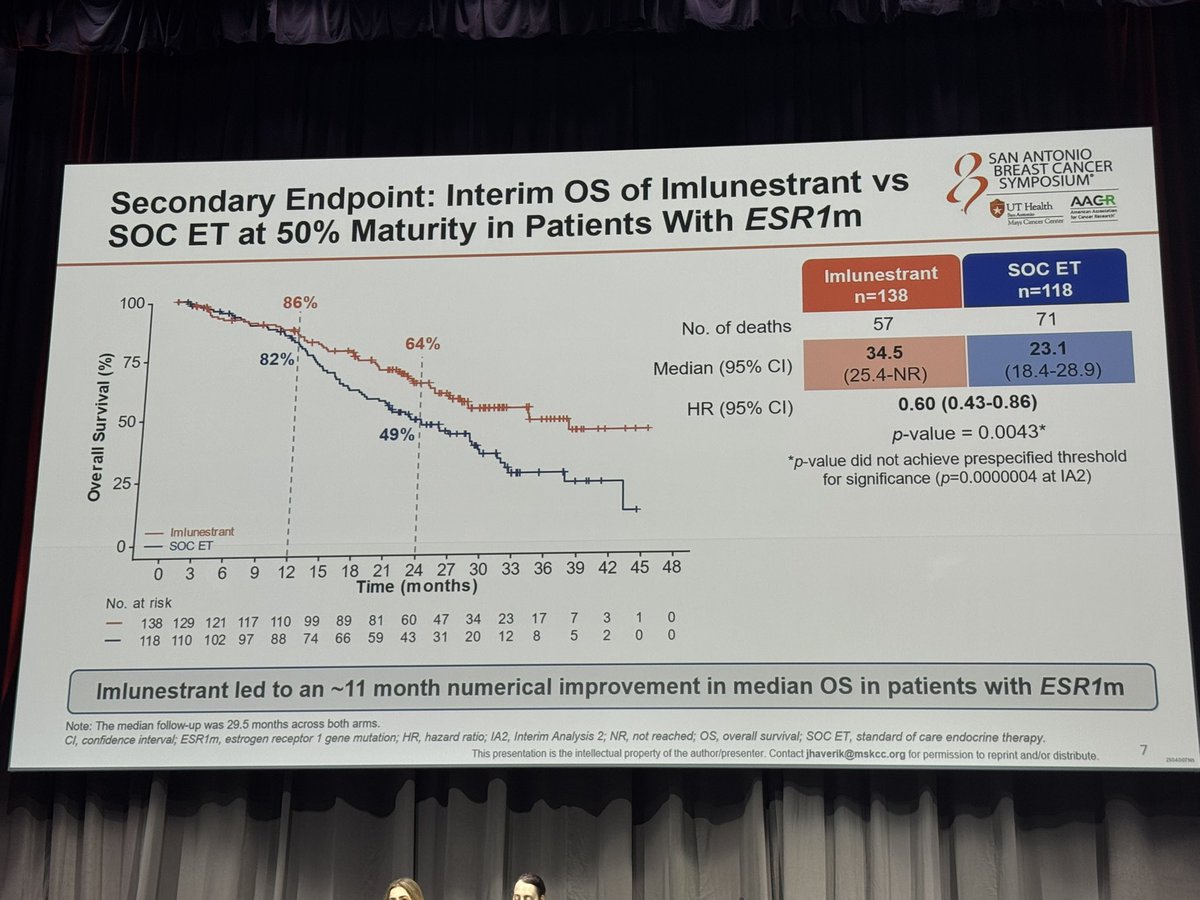
Updated OS data (median follow-up 28.5 months) showed median OS of 34.5 months with imlunestrant vs 23.1 months with SOC in ESR1-mutant patients (HR 0.60; 95% CI: 0.43-0.86; p=0.0043), an 11.4-month improvement, although this did not meet the prespecified boundary for statistical significance. The combination showed a favorable OS trend (HR 0.82; 95% CI: 0.59-1.16). ORR was 14.3% for imlunestrant vs 7.7% for SOC in ESR1-mutant patients.
Imlunestrant monotherapy had a favorable safety profile consistent with endocrine therapy. Grade 3/4 AEs occurred in 17% (vs 21% for SOC). Most common AEs were fatigue (23%), diarrhea (22%), and nausea (17%), predominantly grade 1. Treatment discontinuation due to AEs was only 4%. No cardiac or ocular toxicity signals (no bradycardia or photopsia). The combination with abemaciclib showed expected CDK4/6i toxicity: diarrhea (86%/8% G3), nausea (49%/2% G3), neutropenia (48%/20% G3), with 6% discontinuation rate.
EMBER-3 established imlunestrant as a well-tolerated oral alternative to fulvestrant for ESR1-mutated ER+/HER2- advanced breast cancer, with the key advantage of oral administration eliminating injection-site reactions reported by 72% of fulvestrant patients. The monotherapy benefit is strictly biomarker-gated to ESR1-mutant tumors, mandating Guardant360 CDx liquid biopsy testing. The combination with abemaciclib extends benefit to all patients regardless of ESR1 status, supporting continued CDK4/6 inhibition beyond progression. Key debates include monotherapy vs. combination (QoL advantage of mono vs. PFS advantage of combo), competition with elacestrant and camizestrant in the oral SERD space, and the role of ESR1 testing infrastructure in clinical workflow.












