HER2CLIMB-05 is a Phase 3 trial testing whether adding the HER2 tyrosine-kinase inhibitor tucatinib (Tukysa) to trastuzumab plus pertuzumab as first-line maintenance improves outcomes in HER2-positive metastatic breast cancer. Adding tucatinib improved median progression-free survival to 24.9 vs 16.3 months (HR 0.641; p<0.0001), with immature but favorable early overall-survival data. The first-line maintenance tucatinib regimen is investigational. Sponsor: Seagen (Pfizer).
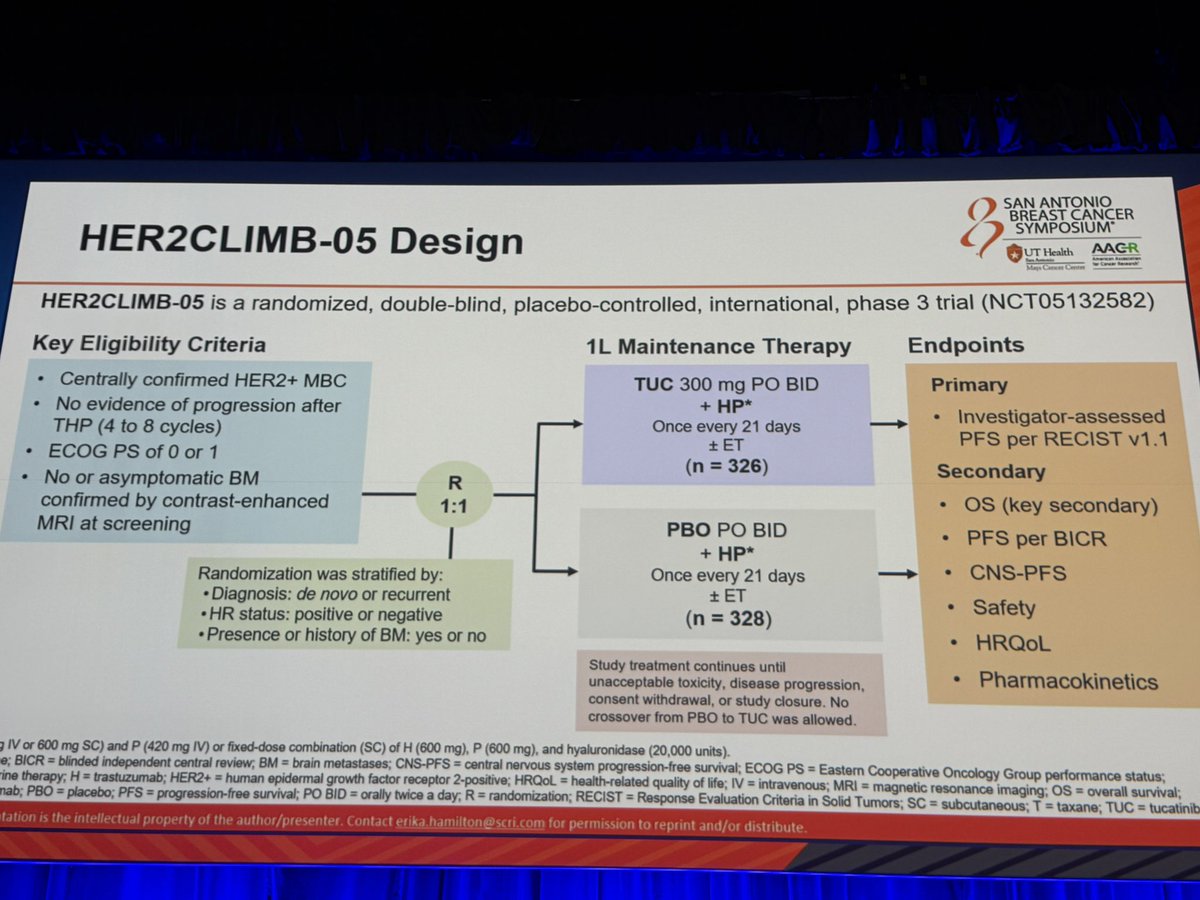
Discover KOL Sentiment on HER2CLIMB-05 →Design — Phase 3, randomized, double-blind; tucatinib (Tukysa) + trastuzumab + pertuzumab (HP) vs placebo + HP as 1L maintenance, HER2+ metastatic breast cancer (NCT05132582). (SABCS 2025)
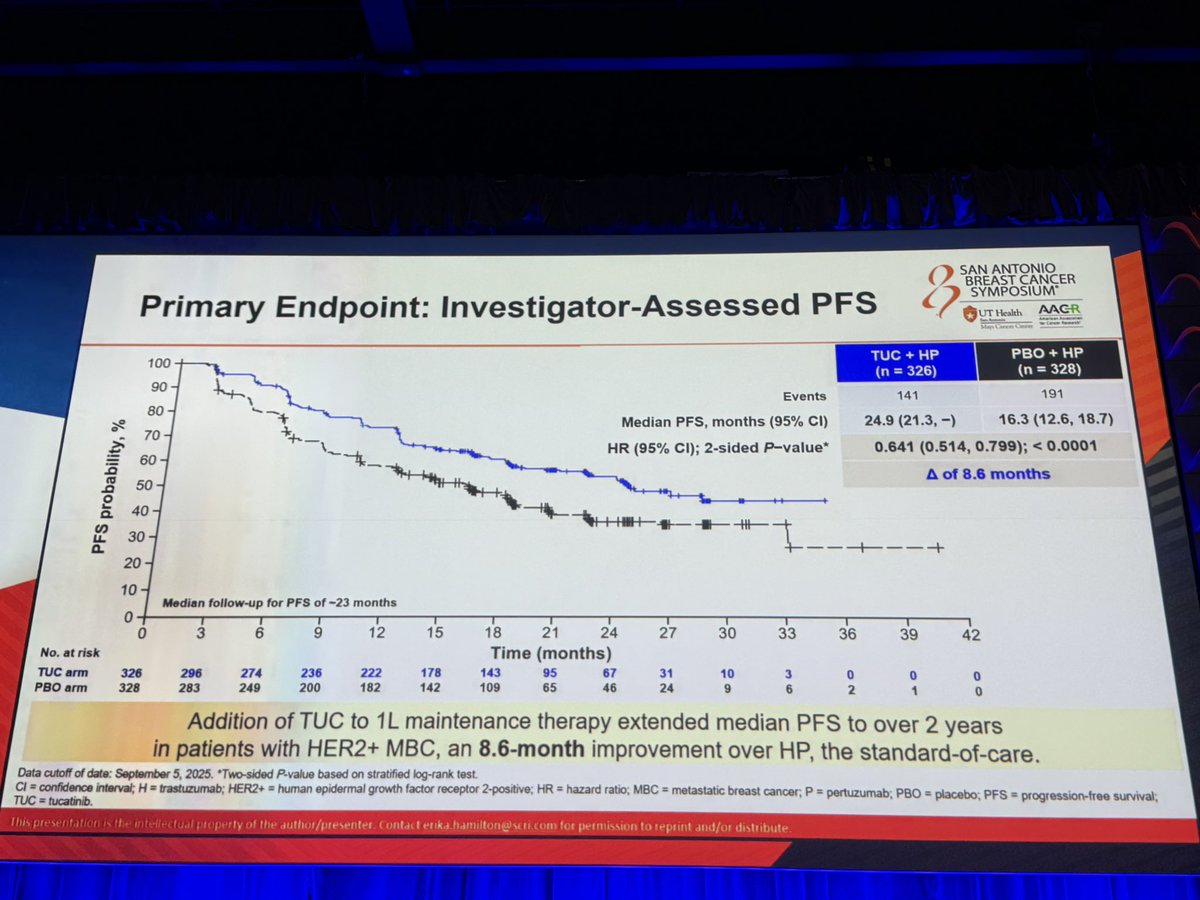
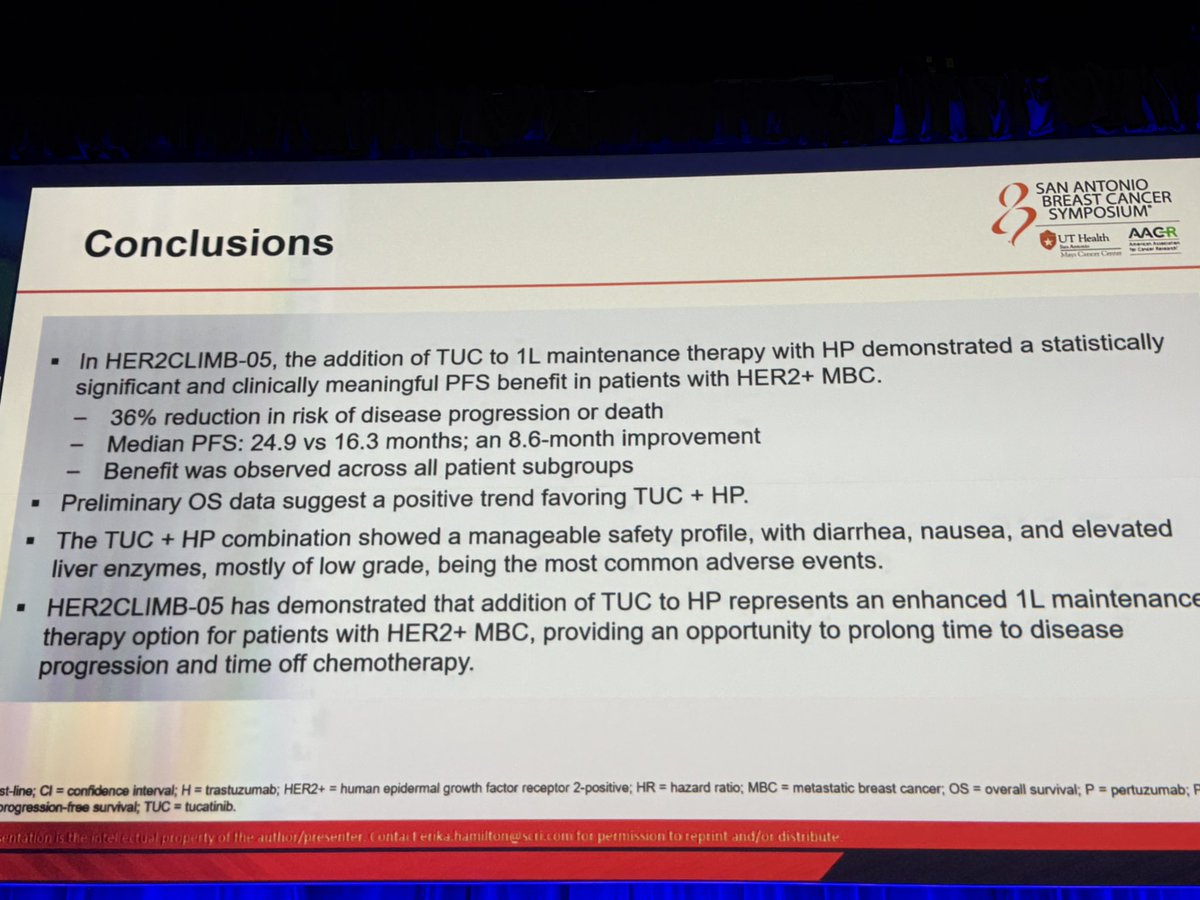
PFS (primary) — Median 24.9 vs 16.3 months at 23-month follow-up (HR 0.641; 95% CI 0.514-0.799; p<0.0001) — 8.6-month absolute improvement; consistent across HR subgroups. (SABCS 2025)
Overall survival — Immature (~20% of required events, 51 deaths); favorable early trend HR 0.539 (95% CI 0.303-0.957); median OS not reached in either arm. (SABCS 2025)
Brain metastases — Benefit reported across subgroups including patients with brain metastases, consistent with tucatinib's CNS activity. (SABCS 2025)
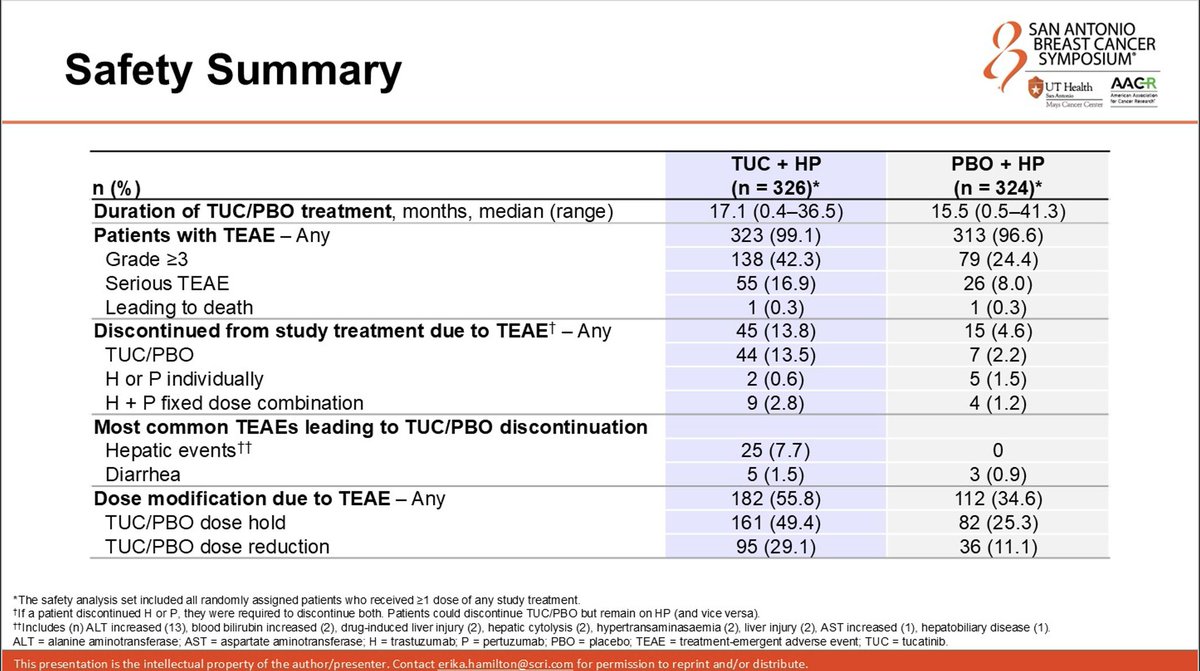
Safety — Grade 3+ TEAEs 42-43% (tucatinib) vs 24% (placebo); diarrhea 72.7% vs 51% any-grade (mostly low-grade); Grade 3+ ALT 13.5%. (SABCS 2025)
Regulatory / Sponsor — INVESTIGATIONAL — 1L maintenance tucatinib+HP is not FDA approved; Tukysa is approved (with trastuzumab + capecitabine) in later-line HER2+ mBC. Seagen/Pfizer. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.














Top 10 by impressions - click to view on X
June 2, 2026 — reactions to Erika Hamilton's ASCO 2026 subgroup presentation (data cut Sept 5, 2025).

HER2CLIMB05: The PFS benefit with tucatinib + HP maintenance was consistent across de novo/recurrent disease, HR+ and HR− tumors, and patients with or without brain metastases. Notably, among patients with baseline brain metastases, median PFS doubled from 4.2 to 8.5 months

Beautiful presentation by @ErikaHamilton9 on HER2CLIMB-05! Subset analysis of pts with HR+ dz by ET use highlights how critical it is to give ET to our HR+ HER2+ pts @OncoAlert #ASCO26

@ErikaHamilton9 beautifully presents additional efficacy and safety from HER2CLIMB05, at median follow up of 23 months mPFS was prolonged by 9 month. In HR- mPFS 12.6 mo improved to 24.9 mos, in HR+, mPFS improved from 18.1 mo to 25 mo, those with and without baseline brains mets

HER2CLIMB-05 subgroup analysis @ErikaHamilton9 Adding tucatinib to trastuzumab/pertuzumab maintenance therapy improved PFS across all major subgroups of HER2+ metastatic breast cancer, including HR-positive and HR-negative disease, patients with or without brain metastases,

Updates from HER2CLIMB-05: Tucatinib + HP Maintenance Significantly Extended PFS After THP Induction in 1L HER2+ Metastatic Breast Cancer #ASCO26 • Tucatinib + maintenance HP improved median PFS: 24.9 vs 16.3 months (HR 0.64) • Delivered an 8.6-month absolute PFS gain after
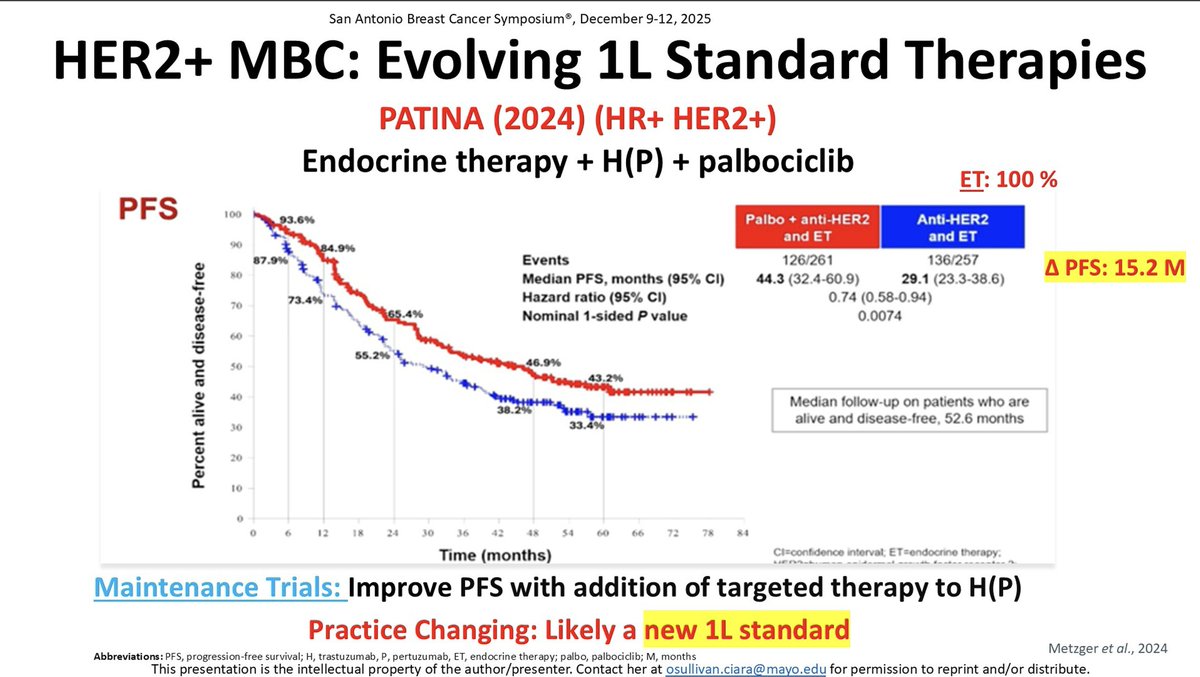
Among pts with ER+/HER2+ MBC, maintenance HP (control arm) had a PFS of: -29.1 mo in PATINA -16.3 mo in HER2CLIMB-05 The difference? In PATINA all pts also received ET (only 45% in...
T-DXd + pertuzumab approved for 1st L HER-2+ #bcsm! Now for the debates around induction length, maintenance, re-induction etc. My opinion: I'll induce to...
Nice table to put this rapidly evolving field in perspective #SABCS25
#SABCS25 ⏳️ After nearly a decade of therapeutic stagnation in the first-line treatment of HER2-positive breast cancer since the publication of CLEOPATRA, we suddenly find ourselves...
A new chemo free maintenance option for patients with HR+ & HR- HER-2 + disease in the 1st line setting post induction chemo that can provide a meaningful benefit in excess of 2 years is a...
DB-09, PATINA, HER2CLIMB-05. After been using the same 1L HER2+ MBC regimen for a decade, everything has changed within 1 single year. All guidelines to be rewritten, algorithms to be developed,...
HER2CLIMB-05 shows addition of tucatinib to maintenance HP, after median 6 cycles THP, improved mPFS 8.6 mos to 24.9 mos. Benefit more pronounced in HR-, but HR+ benefits as well....
#SABCS25 @ErikaHamilton9 presents HER2Climb05. Tucatinib prolonged PFS added to HP maintenance for HER2+ MBC. <50% of HR+ got ET! Why?? More toxicity but manageable....

#SABCS25 Recap #1 | HER2CLIMB-05 HER2CLIMB-05 showed that adding #tucatinib to maintenance HP after 4–6 cycles of THP improved mPFS to ~24 months...
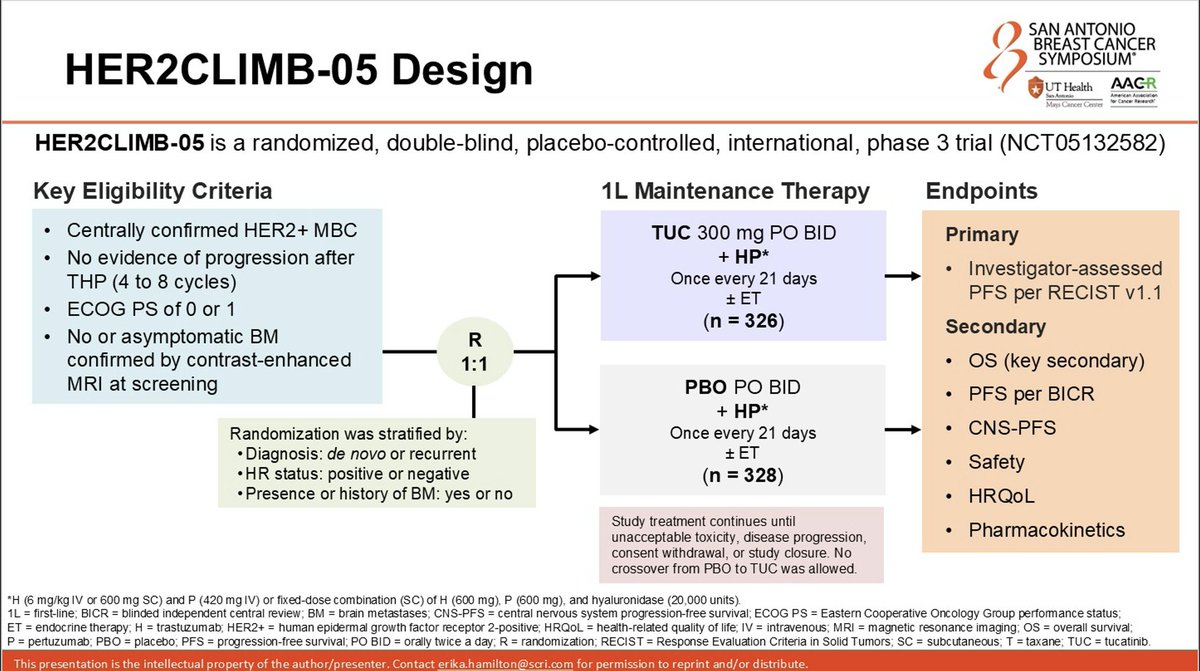
HER2CLIMB-05 is a Phase III, randomized, double-blind, placebo-controlled trial evaluating the addition of tucatinib (Tukysa) to trastuzumab and pertuzumab as first-line maintenance therapy in patients with HER2-positive metastatic breast cancer. The trial enrolled 654 patients who had completed 4-8 cycles of taxane-based induction chemotherapy with trastuzumab and pertuzumab without disease progression. HER2CLIMB-05 demonstrated that adding a selective HER2 tyrosine kinase inhibitor to dual antibody maintenance significantly prolongs time off chemotherapy, representing the first positive Phase III trial of enhanced first-line maintenance in HER2+ mBC.
Phase III, international, randomized (1:1), double-blind, placebo-controlled trial (NCT05132582). Patients received tucatinib 300 mg orally twice daily or placebo alongside trastuzumab plus pertuzumab every 21 days. Endocrine therapy was permitted for HR-positive tumors. Stratified by disease status (de novo vs. recurrent), hormone receptor status, and brain metastases.
Adults with centrally confirmed HER2-positive metastatic breast cancer, ECOG PS 0-1, who had no disease progression after 4-8 cycles of first-line taxane-based induction with trastuzumab and pertuzumab. Patients with asymptomatic brain metastases were allowed; 12.2% had baseline brain metastases. Median age 54 years.
Tucatinib 300 mg orally twice daily plus trastuzumab and pertuzumab (HP) every 21 days versus placebo plus HP, administered as maintenance therapy until disease progression or unacceptable toxicity.
Primary endpoint: investigator-assessed progression-free survival (PFS) per RECIST 1.1. Key secondary endpoints: overall survival (OS), BICR-assessed PFS, CNS-PFS, safety, health-related quality of life, and pharmacokinetics.
At a median follow-up of 23 months, tucatinib plus HP significantly improved PFS versus placebo plus HP. Median PFS was 24.9 months (95% CI: 21.3-NR) versus 16.3 months (95% CI: 12.6-18.7), representing an absolute improvement of 8.6 months (HR 0.641; 95% CI: 0.514-0.799; p<0.0001). In HR-negative patients, PFS HR was 0.554 (24.9 vs. 12.6 months). In HR-positive patients, PFS HR was 0.725 (25.0 vs. 18.1 months). Among patients with baseline brain metastases, median CNS-PFS nearly doubled from 4.3 to 8.5 months. At ASCO 2026 (June 2, 2026; data cut Sept 5, 2025), a subgroup analysis by disease history showed the benefit held across presentations: in de novo disease, median PFS was 28.9 versus 16.8 months (HR 0.621; 95% CI: 0.475-0.813; p=0.0005), and in recurrent disease, 21.3 versus 12.7 months (HR 0.671; 95% CI: 0.457-0.986; p=0.0410) — ASCO 2026, Hamilton, DCO Sept 5 2025.
Overall survival data were immature at the time of analysis, with only 20% of required events (51 deaths) having occurred. Despite this, a positive numerical trend favoring tucatinib was observed: OS HR 0.539 (95% CI: 0.303-0.957; p=0.0320). Median OS was not reached in either arm.
The tucatinib and HP combination showed a manageable safety profile. Grade 3+ TEAEs occurred in 42-43% of tucatinib patients versus 24% with placebo. The most common AEs were diarrhea (72.7% vs. 51% any-grade, mostly low-grade), nausea, and elevated liver enzymes. Grade 3+ ALT elevation occurred in 13.5% and AST in 7.1%, generally asymptomatic and reversible. Hepatic events were the leading cause of tucatinib discontinuation (7.7%). Overall discontinuation of tucatinib due to AEs was 13.5% versus 2.2% for placebo. Dose modifications were required in 55.8% versus 34.6%.
HER2CLIMB-05 establishes tucatinib plus HP as a new enhanced first-line maintenance option for HER2+ mBC, offering patients over 2 years of chemotherapy-free disease control. The trial is notable for consistent benefit across HR subgroups and in patients with brain metastases. Key clinical questions include how this regimen compares or sequences with the newly approved DESTINY-Breast09 (T-DXd + pertuzumab) regimen, and whether OS benefit will be confirmed with further follow-up. Regulatory submissions are anticipated based on these data.
HER2CLIMB-05 (NCT05132582) is a Phase 3, randomized, double-blind trial testing whether adding the HER2 tyrosine-kinase inhibitor tucatinib (Tukysa) to trastuzumab plus pertuzumab as first-line maintenance therapy improves outcomes in HER2-positive metastatic breast cancer, compared with placebo plus trastuzumab and pertuzumab. It was sponsored by Seagen, a Pfizer company.
At a median follow-up of 23 months, adding tucatinib significantly improved progression-free survival: median 24.9 versus 16.3 months (HR 0.641; 95% CI 0.514-0.799; p<0.0001), an 8.6-month absolute gain. Overall survival was immature (about 20% of required events) but showed a favorable early trend (HR 0.539), with median OS not reached in either arm.
No. The first-line maintenance regimen of tucatinib added to trastuzumab and pertuzumab studied in HER2CLIMB-05 is investigational and not FDA approved. Tucatinib (Tukysa) is separately FDA approved, with trastuzumab and capecitabine, for later-line advanced or metastatic HER2-positive breast cancer (including brain metastases) after one or more prior anti-HER2 regimens.
The trial reported consistent progression-free survival benefit across subgroups, including patients with brain metastases, which is notable given tucatinib's known central nervous system activity. This CNS activity was a defining feature of the original HER2CLIMB trial that supported tucatinib's approval.
Adding tucatinib increased toxicity: Grade 3 or higher treatment-emergent adverse events occurred in about 42-43% of tucatinib patients versus 24% with placebo. Diarrhea was the most common event (72.7% versus 51% any-grade, mostly low-grade), and Grade 3 or higher ALT elevation occurred in about 13.5%, requiring liver-enzyme monitoring.















