Perioperative resectable NSCLC - AstraZeneca
Discover KOL Sentiment on AEGEAN →













Top 10 by impressions - click to view on X
#AACR23 Is #AEGEAN a practice-changing study by @DrRoyHerbstYale? - with similar outcomes to CM816, AEGEAN represents a new option of periop chemo-IO + 1...
Impressive data from #AEGEAN at #AACR23 from Dr. John Heymach and colleagues. This is the first of several phase III peri-operative IO studies in resectable NSCLC...

Based on the CM 816, Aegean and now KN 671, for stage 2/3 resectable NSCLC with no genomic alterations, do you give: #ASCO23
For patients with resectable, early-stage NSCLC, surgery remains the primary curative-intent treatment; however, many patients have tumor recurrence within 5 years after surgery. Full AEGEAN trial...
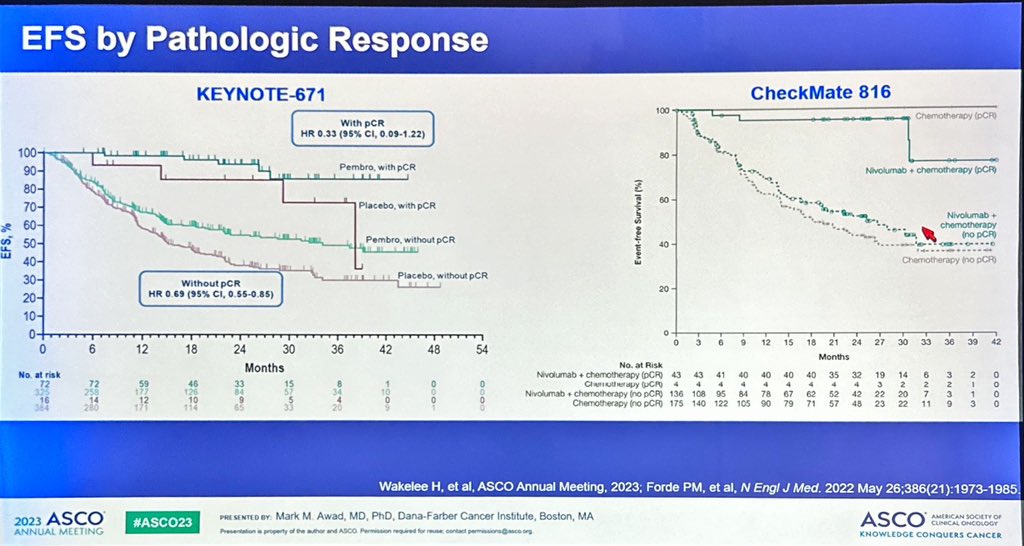
Great discussion of KEYNOTE 671 by Dr. @DrMarkAwad at #ASCO23. Notes challenges of comparing studies given differences in populations. But EFS curves do appear to widen over...

🔥🚨@OncoAlert Hot off the press. Just published @NEJM in conjunction with presentation @myESMO #ESMO23. “Results of #AEGEAN trial of...
Original Article: Perioperative Durvalumab for Resectable Non–Small-Cell Lung Cancer (AEGEAN phase 3 trial) #oncology
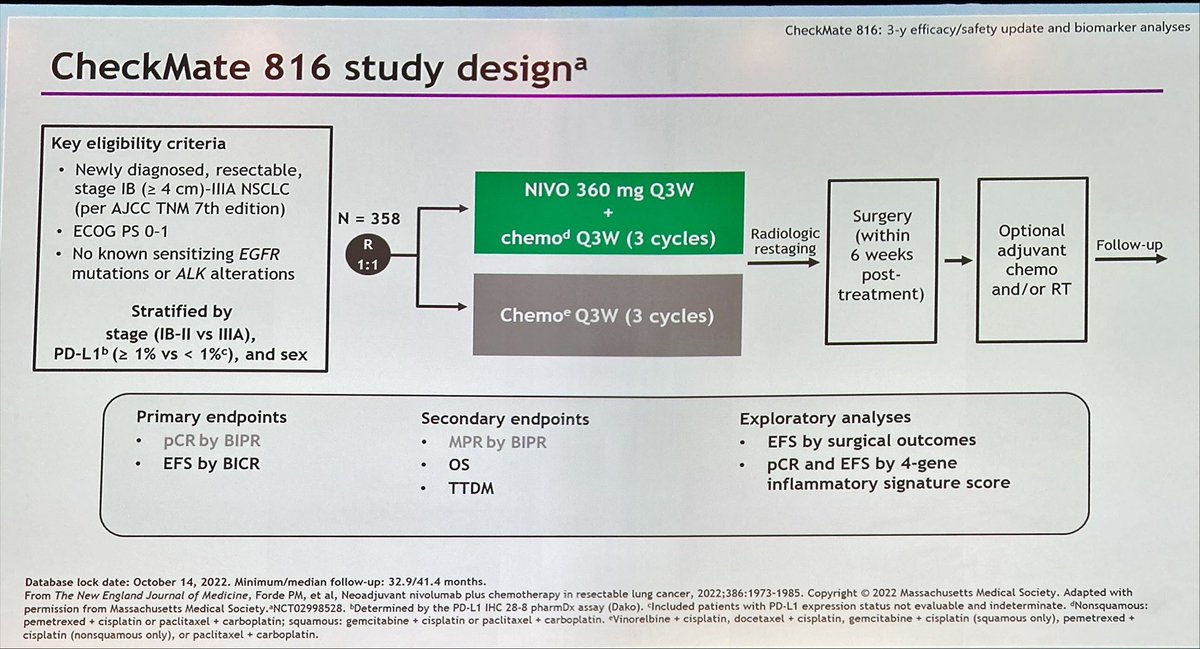
#CM816 3yr update was recently presented at #ELCC23 (OS: 0.67 and EFS 57% at 3yrs/65% at 2yrs) and today, #AEGEAN data was presented at...

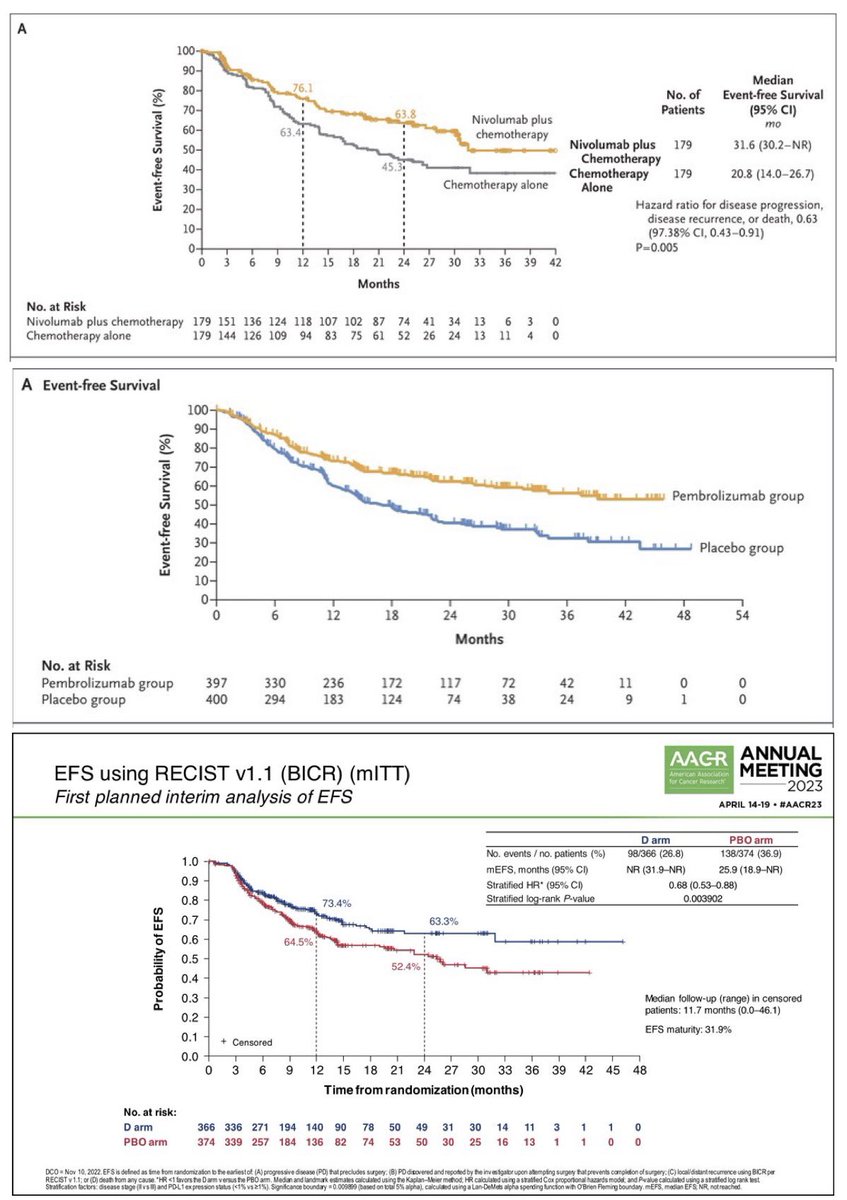
Three phase 3 trials of neoadjuvant IO for NSCLC with survival data. 2-year EFS was: - 63.8% with neoadjuvant only nivo (CM816, 4 cycles of IO) - 62.4% with neoadjuvant + adjuvant pembro (KN671, 17...
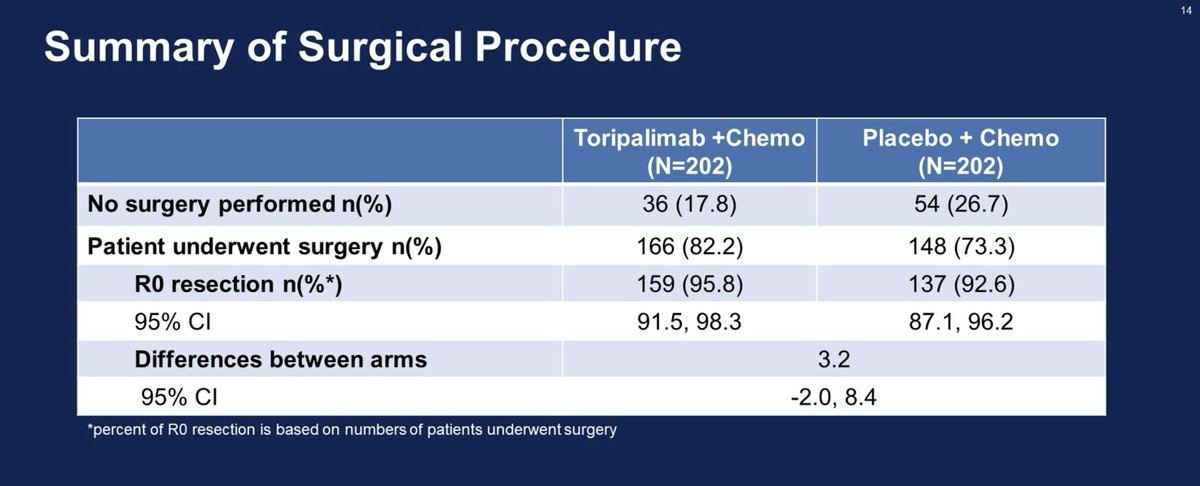
Once again, many participants (22%) who were started on systemic therapy didn't make it to surgery. By comparison: CM816 = 20%, AEGEAN = 19%. Are any of these people being...
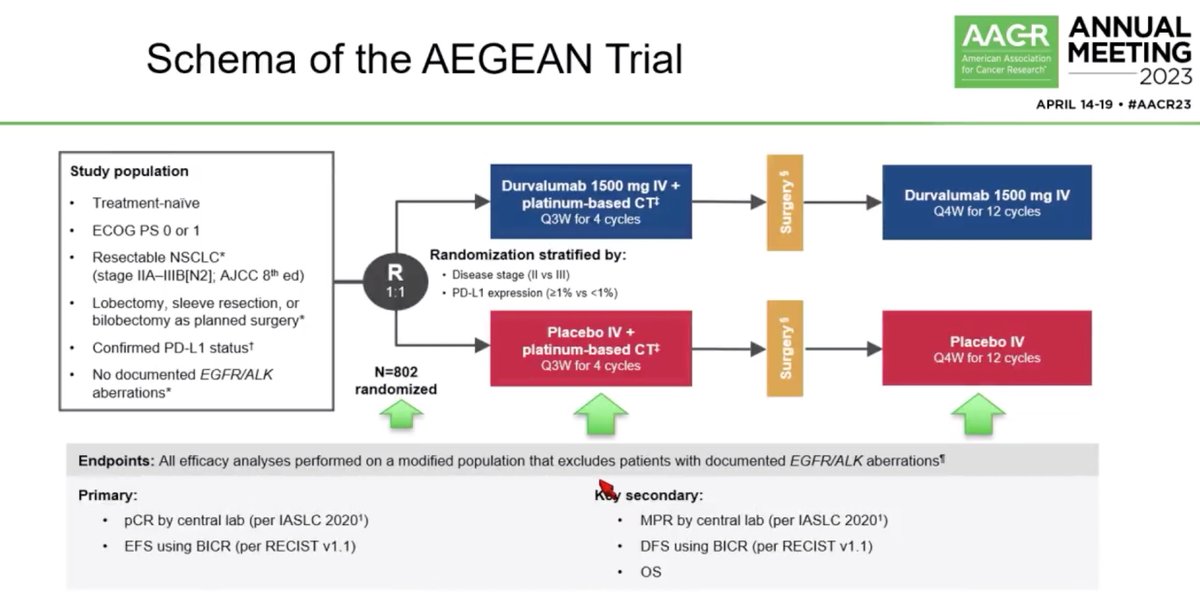
AEGEAN is a global Phase III, randomized, double-blind, placebo-controlled trial evaluating perioperative durvalumab (Imfinzi) in combination with neoadjuvant platinum-based chemotherapy for patients with resectable non-small cell lung cancer (stage IIA to IIIB [N2], AJCC 8th edition). The trial randomized 802 patients 1:1 to receive neoadjuvant durvalumab 1500 mg plus chemotherapy or placebo plus chemotherapy every 3 weeks for 4 cycles prior to surgery, followed by adjuvant durvalumab or placebo every 4 weeks for up to 12 cycles. AEGEAN is the first phase 3 study to describe the benefit of perioperative immunotherapy plus neoadjuvant chemotherapy in resectable NSCLC, irrespective of PD-L1 expression, and led to FDA approval in August 2024.
Phase III, global, double-blind, 1:1 randomized, placebo-controlled trial in patients with treatment-naive, resectable stage IIA-IIIB (N2) NSCLC (tumors ≥4 cm and/or node positive). Randomization stratified by disease stage (II vs. III) and PD-L1 expression (≥1% vs. <1%, assessed by VENTANA PD-L1 [SP263] IHC assay). Patients with documented EGFR mutations or ALK rearrangements were excluded from efficacy analyses. Choice of platinum-based chemotherapy was at investigator discretion.
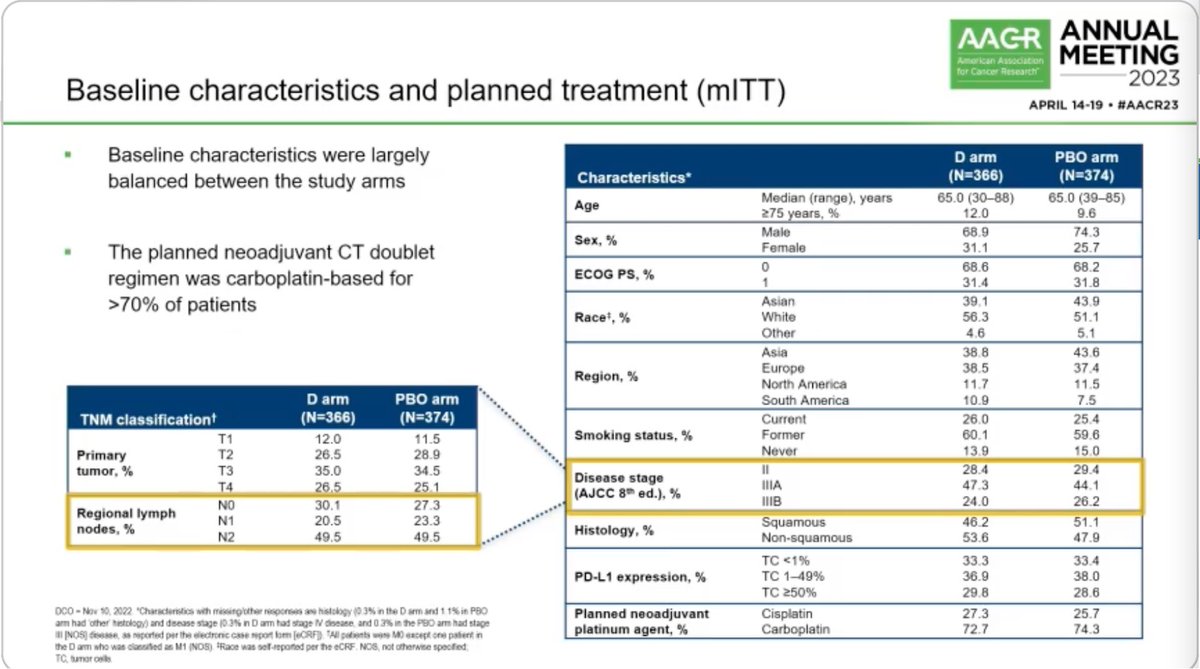
Adults with newly diagnosed, previously untreated, resectable stage IIA-IIIB (N2) NSCLC per AJCC 8th edition, ECOG PS 0-1, estimated life expectancy ≥12 weeks. Planned surgery limited to lobectomy, sleeve resection, or bilobectomy. Excluded: documented EGFR/ALK alterations, T4 tumors (except size >7 cm), planned pneumonectomy. Approximately 71% had stage III disease; 49.5% had N2 disease.
Neoadjuvant: durvalumab 1500 mg IV plus platinum-based chemotherapy every 3 weeks for up to 4 cycles, followed by surgery. Adjuvant: durvalumab 1500 mg IV every 4 weeks for up to 12 cycles. Control arm received matched placebo in both phases.
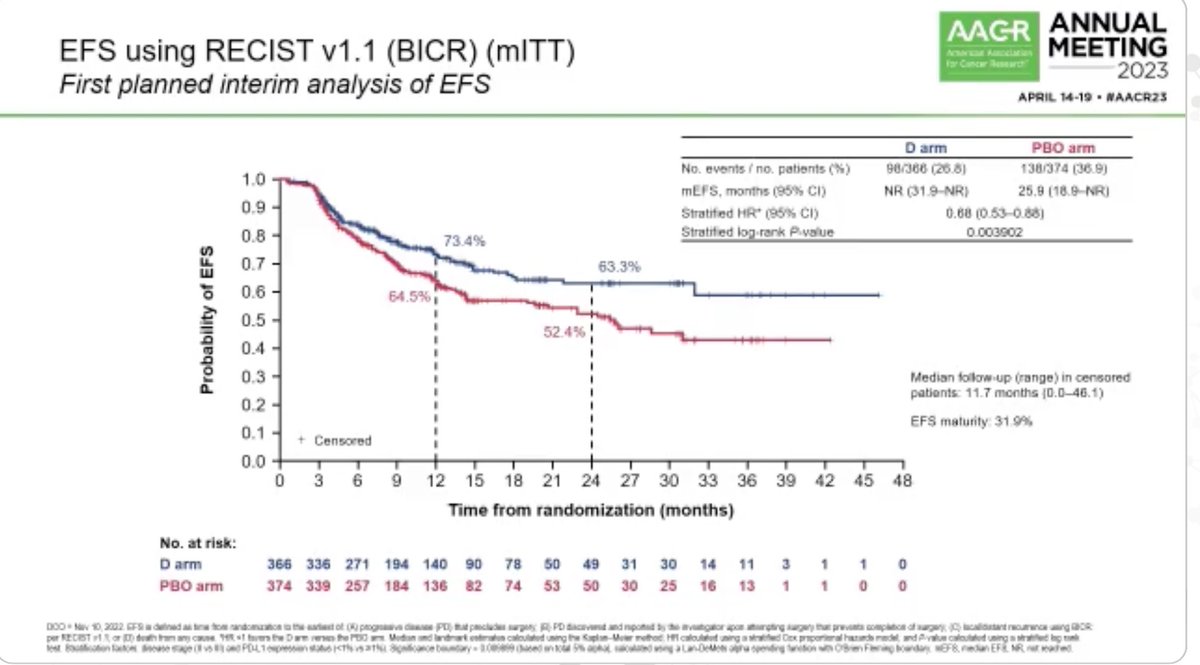
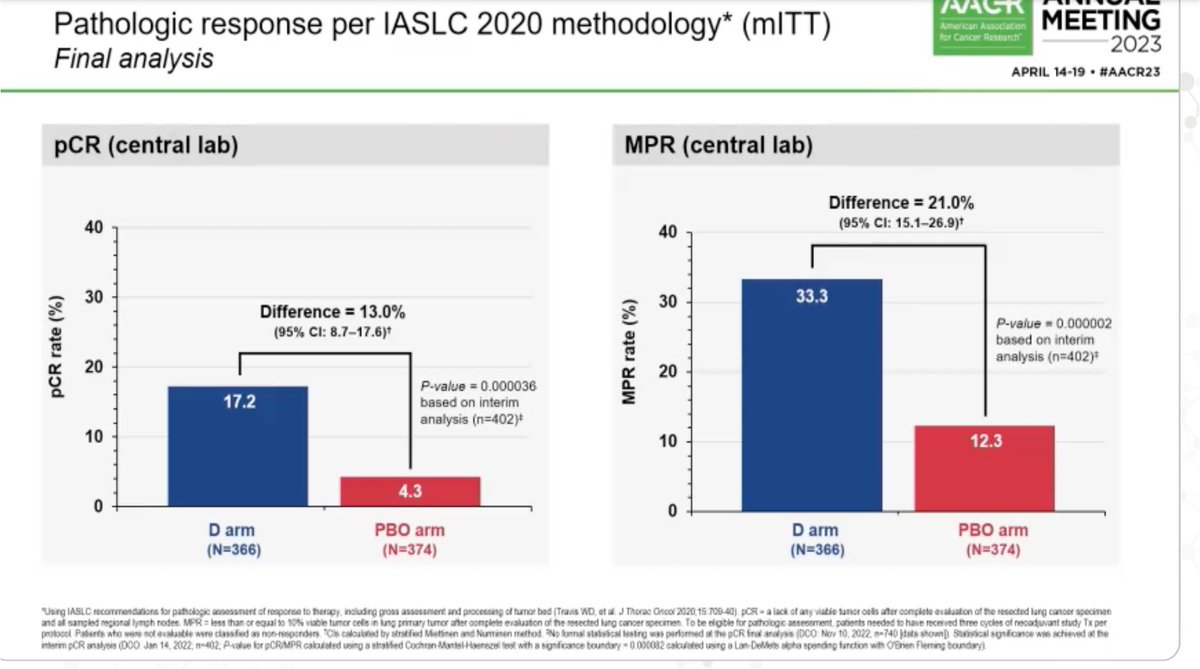
Co-primary endpoints: event-free survival (EFS) assessed by blinded independent central review (BICR, RECIST v1.1) and pathological complete response (pCR) assessed by blinded central pathology review (IASLC 2020 criteria). Key secondary endpoints: major pathologic response (MPR), disease-free survival (DFS) in the resected subpopulation, overall survival (OS), safety, and health-related quality of life.
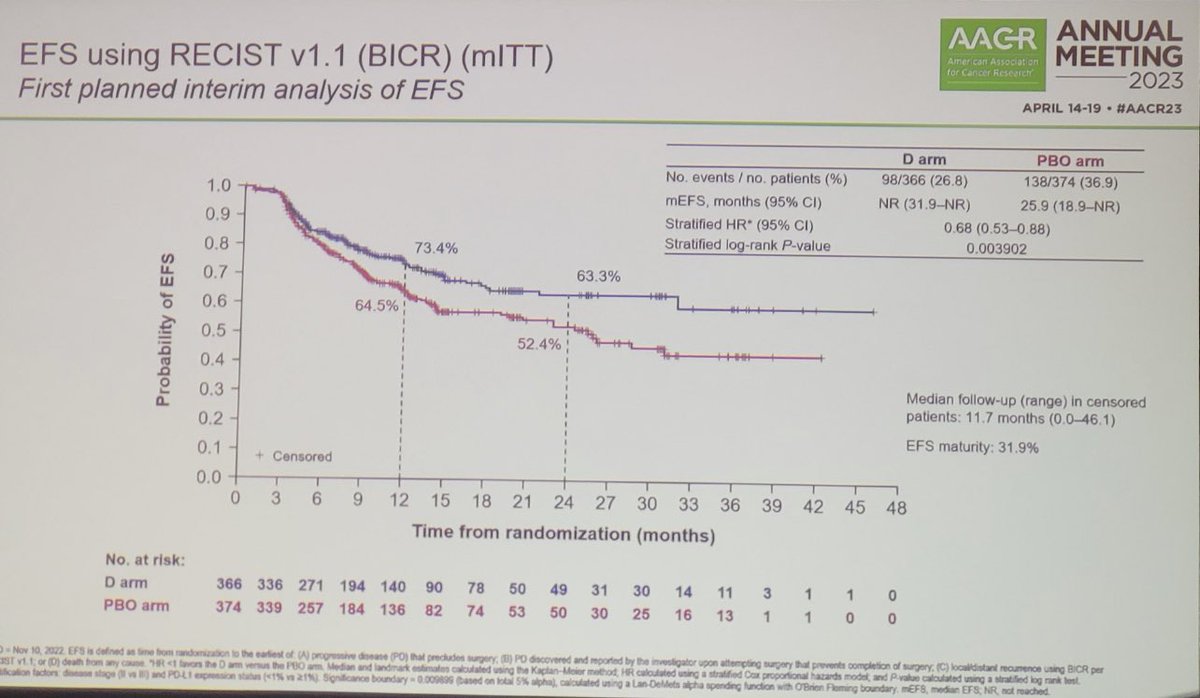
At the first interim analysis, perioperative durvalumab demonstrated a statistically significant EFS improvement: EFS HR 0.68 (95% CI: 0.53-0.88; p=0.004), with median EFS not reached vs. 25.9 months for placebo. The pCR rate was 17.2% vs. 4.3% (difference 13.0%; p<0.001). At the updated second interim analysis (25.9 months median follow-up, 39.1% maturity), the EFS HR was maintained at 0.69 (95% CI: 0.55-0.88), with median EFS not reached (95% CI: 42.3-NR) vs. 30.0 months (95% CI: 20.6-NR). Three-year EFS rates were 60.1% vs. 47.9%.
At the time of the prespecified interim analyses, overall survival was not formally tested for statistical significance. A descriptive analysis at the second interim analysis showed a trend favoring durvalumab with OS HR 0.89 (95% CI: 0.70-1.14) at 35.3% maturity, with median OS not reached in either arm. Lung cancer-specific survival HR was 0.70 (95% CI: 0.52-0.93), with 3-year rates of 76.7% vs. 68.9%.
The safety profile was manageable and consistent with the individual agents. Grade 3/4 AEs occurred in 43.6% of durvalumab patients vs. 43.2% with placebo across the overall study period. Immune-mediated AEs occurred in 25.4% vs. 10.3% (grade 3/4: 4.5% vs. 2.5%). Immune-mediated pneumonitis: 4.5% vs. 1.8%. Treatment discontinuation due to AEs: 12.7% vs. 6.3%. Surgical complications were similar between arms (59.1% vs. 60.1%); grade ≥3 surgical complications: 6.1% vs. 8.3%. Surgery cancellation due to AEs: 1.7% vs. 1.0%.
AEGEAN established perioperative durvalumab as a new treatment option for resectable NSCLC, receiving FDA approval in August 2024. However, the trial design cannot distinguish whether the benefit comes from the neoadjuvant phase, adjuvant phase, or both. ODAC unanimously agreed that future perioperative trials must assess the contribution of each treatment phase. Key debates include potential overtreatment (given adjuvant durvalumab alone failed to show DFS benefit in a separate trial), the role of ctDNA-based surrogate markers, and how to manage the adjuvant phase based on pathologic response status. AEGEAN competes in a crowded perioperative NSCLC space alongside KEYNOTE-671 (pembrolizumab, which has demonstrated OS benefit with HR 0.72) and CheckMate 77T (nivolumab).




































