BREAKWATER is a Phase III trial of first-line encorafenib (BRAFTOVI) + cetuximab (Erbitux) + mFOLFOX6 in BRAF V600E-mutant metastatic colorectal cancer. It near-tripled median overall survival (30.3 vs 15.1 months, HR 0.49) and improved PFS (12.8 vs 7.1 months, HR 0.53). FDA-approved (traditional, February 24, 2026). Sponsor: Pfizer.
BRAF V600E-mutant metastatic colorectal cancer (1L)BRAFTOVI + Erbitux + mFOLFOX6/FOLFIRIASCO 2025 (#ASCO25) / ASCO GI 2026 Cohort 3✓ FDA Approved (2026-02)
Design: Phase III randomized trial (NCT04607421) of first-line encorafenib + cetuximab + mFOLFOX6 vs standard-of-care chemotherapy in BRAF V600E-mutant metastatic colorectal cancer. PFS (dual primary): 12.8 vs 7.1 months, HR 0.53 (95% CI 0.41–0.68, P<0.0001). OS: 30.3 vs 15.1 months, HR 0.49 (95% CI 0.38–0.63, P<0.0001) — a near-tripling of median survival (NEJM / ASCO 2025). ORR: ~61% vs 40%. Cohort 3 (FOLFIRI backbone, ASCO GI 2026): ORR ~64% vs 39%, early OS trend HR 0.49 (OS immature) — a non-oxaliplatin option. Companion diagnostic: Guardant360 CDx (co-approved). Regulatory: ✅ FDA-approved — accelerated approval Dec 20, 2024, converted to traditional (full) approval Feb 24, 2026 based on OS, in exactly this 1L BRAF V600E mCRC indication. Sponsor/drug: Pfizer; encorafenib (BRAFTOVI) + cetuximab (Erbitux, Eli Lilly).
Influence Leaders
Top KOLs Discussing BREAKWATER
Dr. Cathy Eng
@CathyEngMD
35.8K impressions
Nicholas Hornstein
@GIMedOnc
16.3K impressions
Oncology Brothers
@OncBrothers
10.4K impressions
Yakup Ergün
@dr_yakupergun
8.7K impressions
Krishan Jethwa
@KrishanJethwa
8.3K impressions
Dr Amol Akhade
@SuyogCancer
7.6K impressions
Conference Presentations
BREAKWATER Key Slides & Visuals
Official trial slides and relevant visuals shared by KOLs at ASCO 2025 (#ASCO25) / ASCO GI 2026 Cohort 3. Click any image to expand.
[Slide 1]
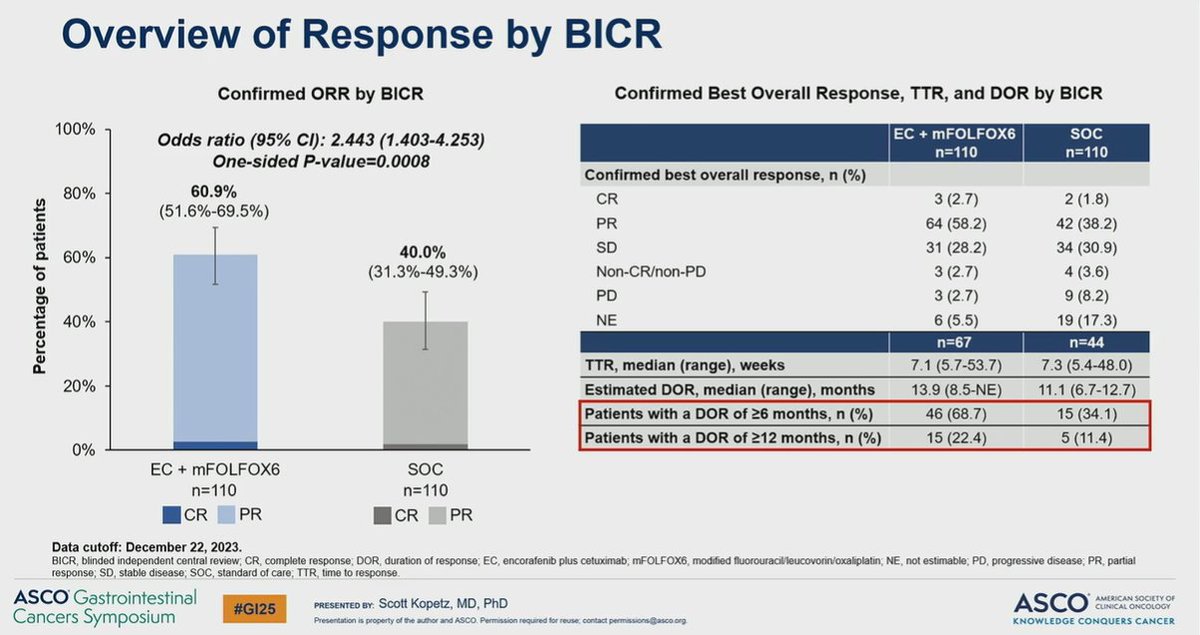
Overview of Response by BICR
Confirmed ORR by BICR
Confirmed Best Overall Response, TTR, and DOR by BICR
100%
Odds ratio (95% CI): 2.443 (1.403-4.253)
EC + mFOLFOX6
SOC
n=110
n=110
One-sided P-value=0.0008
Confirmed best overall response, n (%)
80%
60.9%
CR
3 (2.7)
2 (1.8)
(51.6%-69.5%)
PR
64 (58.2)
42 (38.2)
Percentage of patients
40.0%
SD
60%
31 (28.2)
34 (30.9)
(31.3%-49.3%)
Non-CR/non-PD
3 (2.7)
4 (3.6)
PD
3 (2.7)
9 (8.2)
40%
NE
6 (5.5)
19 (17.3)
n=67
n=44
TTR, median (range), weeks
7.1 (5.7-53.7)
7.3 (5.4-48.0)
20%
Estimated DOR, median (range), months
13.9 (8.5-NE)
11.1 (6.7-12.7)
Patients with a DOR of ≥6 months, n (%)
46 (68.7)
15 (34.1)
Patients with a DOR of â¥12 months, n (%)
15 (22.4)
5 (11.4)
0%
EC + mFOLFOX6
SOC
n=110
n=110
CR
PR
CR
PR
Data cutoff: December 22, 2023.
BICR, blinded independent central review, CR, complete response; DOR, duration of response; EC, encorafenib plus cetuximab; mFOLFOX6, modified fluorouracil/leucovorin/oxaliplatin; NE, not estimable; PD, progressive disease; PR, partial
response; SD, stable disease; SOC, standard of care; TTR, time to response
ASCO Gastrointestinal
#GI25
PRESENTED BY: Scott Kopetz, MD, PhD
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
Cancers Symposium
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 2]
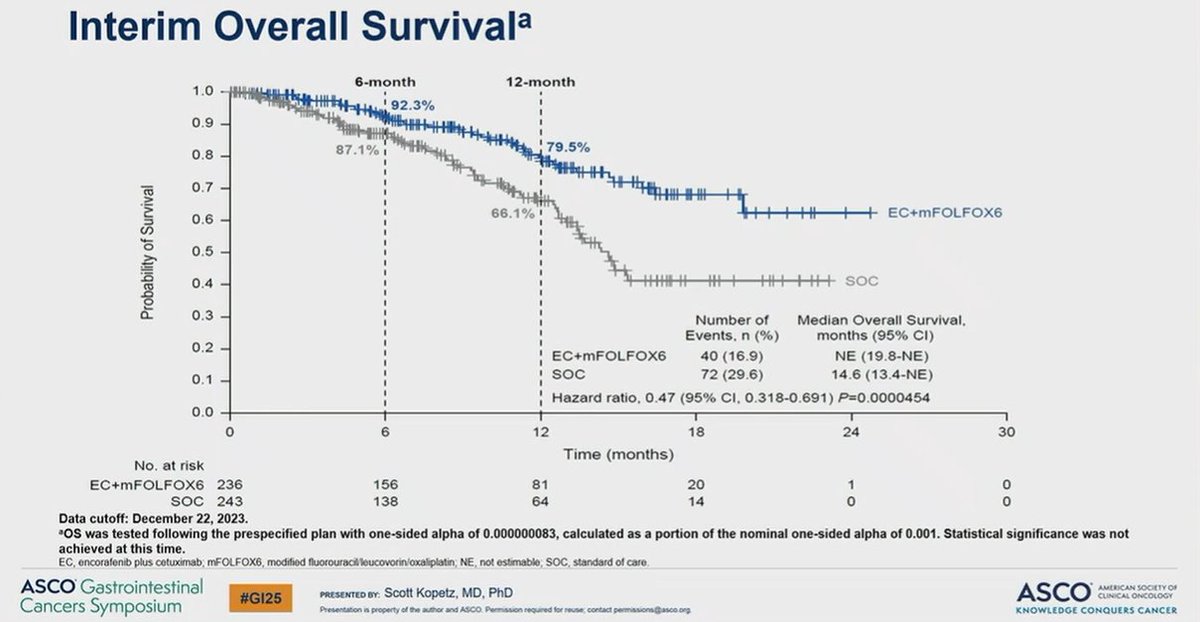
Interim Overall Survivalᵃ
6-month
12-month
1.0
92.3%
0.9
0.8
87.1%
79.5%
0.7
Probability of Survival
66.1%
EC+mFOLFOX6
0.6
0.5
0.4
SOC
0.3
Number of
Median Overall Survival,
Events, n (%)
months (95% CI)
0.2
EC+mFOLFOX6
40 (16.9)
NE (19.8-NE)
0.1
SOC
72 (29.6)
14.6 (13.4-NE)
Hazard ratio, 0.47 (95% CI, 0.318-0.691) P=0.0000454
0.0
0
6
12
18
24
30
Time (months)
No. at risk
EC+mFOLFOX6 236
156
81
20
1
0
SOC 243
138
64
14
0
0
Data cutoff: December 22, 2023.
OS was tested following the prespecified plan with one-sided alpha of 0.000000083, calculated as a portion of the nominal one-sided alpha of 0.001. Statistical significance was not
achieved at this time.
EC, encorafenib plus cetuximab; mFOLFOX6, modified fluorouraci/leucovorin/oxaliplatin; NE, not estimable; SOC, standard of care.
ASCO Gastrointestinal
#GI25
ASCO
AMERICAN SOCIETY OF
PRESENTED BY: Scott Kopetz, MD, PhD
CLINICAL ONCOLOGY
Cancers Symposium
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
[Slide 1]
2
Key Takeaway Points
Precision oncology has now fully entered the first-line setting of mCRC,
with early combinations tailored to molecular subtypes delivering
clinically transformative outcomes:
encorafenib + cetuximab + mFOLFOX based on BREAKWATER in
BRAF V600E is to be considered practice changing
Pause
nivolumab + ipilimumab based on Checkmate 8HW in MSI-H is to
be considered practice changing
Oral Multikinase inhibitors including antiangiogenic properties remain
anchored in broader applicability, but the ANCHOR trial of anlotinib +
chemotherapy does not shift current standards in 1L RAS/BRAF WT
disease
2025 ASCO
#ASCO25
PRESENTED BY: Andrea Sartore-Bianchi, MD
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse contact permissions@@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 2]
12
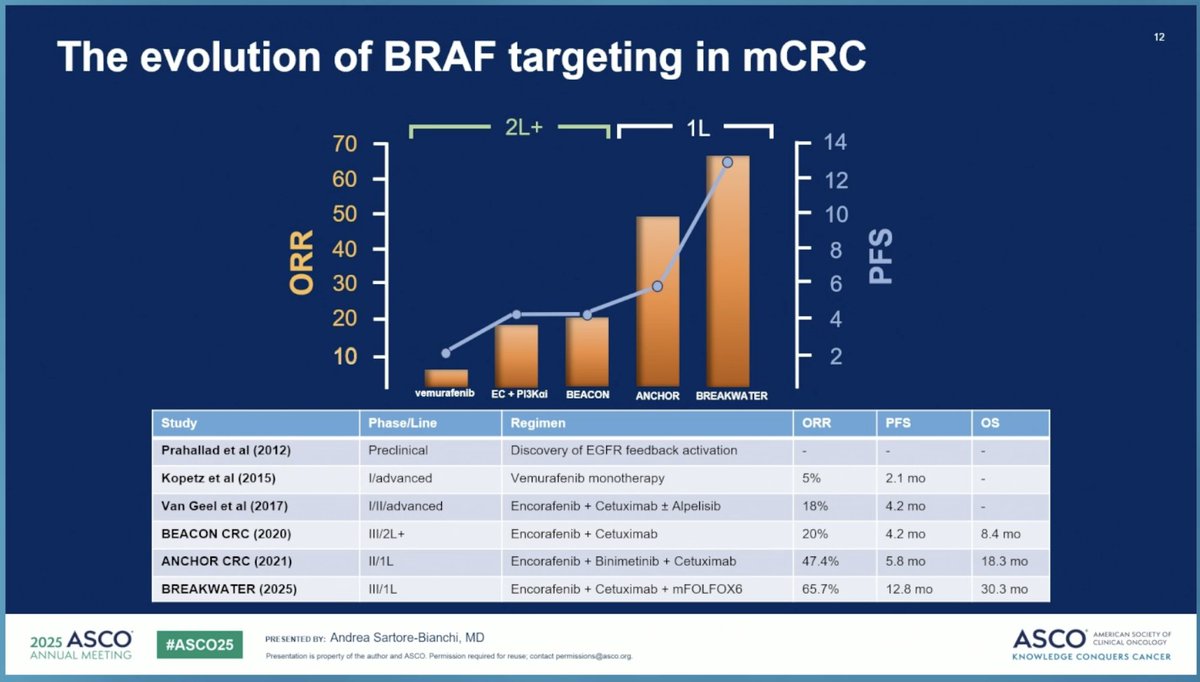
The evolution of BRAF targeting in mCRC
2L+
1L
70
14
O
60
12
50
10
ORR
40
8
PFS
30
O
6
20
4
10
2
vemurafenib
EC PI3Kai
BEACON
ANCHOR
BREAKWATER
Study
Phase/Line
Regimen
ORR
PFS
OS
Prahallad et al (2012)
Preclinical
Discovery of EGFR feedback activation
-
-
-
Kopetz et al (2015)
l/advanced
Vemurafenib monotherapy
5%
2.1 mo
-
Van Geel et al (2017)
I/II/advanced
Encorafenib + Cetuximab + Alpelisib
18%
4.2 mo
-
BEACON CRC (2020)
III/2L+
Encorafenib + Cetuximab
20%
4.2 mo
8.4 mo
ANCHOR CRC (2021)
II/1L
Encorafenib + Binimetinib + Cetuximab
47.4%
5.8 mo
18.3 mo
BREAKWATER (2025)
III/1L
Encorafenib + Cetuximab + mFOLFOX6
65.7%
12.8 mo
30.3 mo
2025 ASCO
#ASCO25
PRE SENTED BY: Andrea Sartore-Bianchi, MD
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 3]
22
3501: CheckMate 8HW expanded results
Clinical interpretation framework
BUT
YES,
NIVO IPI
NIVO
(n 352)
(n 351)
Checkmate
All treated patients, n (%)
Any grade
Grade 3/4
Any grade
Grade 3/4
Progression-free survival: NIVO + IPI vs NIVO (all lines)
TRAEs*
Any TRAEs
285 (81)
78 (22)
249 (71)
50 (14)
Centrally confirmed
NIVO
100
MSI-M/diam
(n = 296)
( - 286)
Serious TRAEs
65 (18)
55 (16)
29 (8)
24 (7)
Median PFS,' mo
NR
19.3
90
12-mo rate
24-mo rate
95% CI
53.8-NE
22.1-NE
TRAEs leading to discontinuation
48 (14)
33(9)
21 (6)
14 (4)
36-mo rate
60
76%
71%
MR (95% o)
elated deaths
2 1)*
1 1)*
67%
Progression-free survival (%)
70
rted in 2 10% of patients
60
62%
91 (26)
0
63 (18)
0
50
55%
51%
71 (20)
3 (< 1)
59 (17)
2 (< 1)
40
idism
61 (17)
2 (< 1)
31(9)
0
10
20
58 (16)
2 (< 1)
44 (13)
2 (< 1)
10
42 (12)
1(<1)
35 (10)
1 (< 1)
0
Hyperthyroidism
40 (11)
0
16(5)
0
0
1
5
9
12
15
18
21
24
27
30
13
36
39
42
45
48
51
54
57
60
No. risk
Months
Arthralgia
38 (11)
1 (<1)
23 (7)
0
NIVO
296
248
234
225
214
207
200
180
164
146
136
134
121
102
100
61
54
29
23
0
0
Rash
34 (10)
3 (< 1)
29(8)
1 1)
HIVO
286
210
E
179
169
184
158
141
124
109
"
=
=
72
19
19
"
15
12
1
0
Adrenal insufficiency
34(10)
8(2)
12(3)
3 (< 1)
The long-term benefit of upfront dual ICI justifies the up-front immune-related risk when patients
are well selected
I
(
clinical scores?) and toxicities managed proactively
NIVO + IPI should be considered a standard of care option in 1L MSI-H mCRC
2025 ASCO
#ASCO25
PRE SENTED BY: Andrea Sartore-Bianchi, MD
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 4]
5
The evolution of precision oncology in 1L mCRC
Treatment of mCRC slowly progressed from primarily relying on chemotherapy
to incorporating targeted therapies and immunotherapy
The key advancements that catalyzed the transition of precision oncology into
the 1L therapeutic landscape have been RAS selection for anti-EGFR, MMR
selection, and histology-specific BRAF, KRAS G12C and HER2 targeting
Bevacizumab
Panitumumab
chemo-sensitive
Cetuximab
FOLFOX
Histology (CRC) -
Encorafenib +
5FU
5FU/LV
FOLFIRI
Capecitabine
RAS selection
specific targeting
cetuximab + CT
1960
1980
2000 2004 2006 2012 2014 2015
2020
2023
2025
Cetuximab
Encorafenib +
Sotorasib +
Regorafenib
chemo-refractory
Ramucirumab cetuximab
Tucatinib +
Panitumumab
panitumumab
trastuzumab
Ziv-aflibercept
2025 ASCO
#ASCO25
PRESENTED BY: Andrea Sartore-Bianchi, MD
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
[Slide 1]
The NEW ENGLAND
10
JOURNAL of MEDICINE
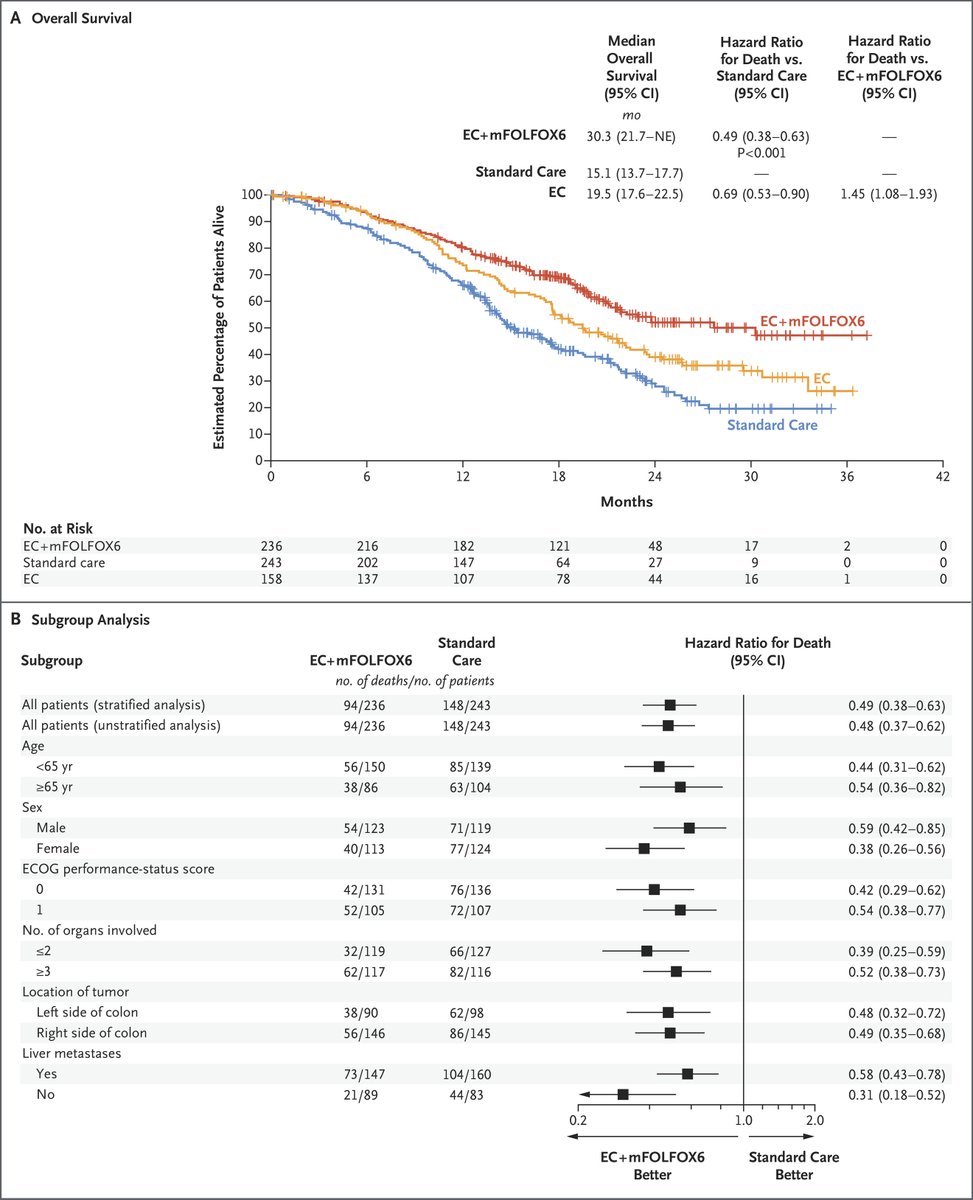
Progression-free Survival
100
90
80
Estimated Percentage of Patients
70
Free from Event
60
50
40
EC+mFOLFOX6
30
20
Standard Care
10
EC
0
0
6
12
18
24
30
36
42
Months
ORIGINAL ARTICLE MAY 30, 2025
MEETING OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY
Targeted Therapy in BRAF
V600E Metastatic Colorectal
Cancer
E. Elez and Others
New 1L standard of care for BRAF V600E-mutant mCRC. Near-tripled OS (30.3 vs 15.1 mo, HR 0.49) in a historically aggressive subtype. Cohort 3 (FOLFIRI backbone) is extending evidence to patients with oxaliplatin contraindications.
FDA APPROVED BRAFTOVI (encorafenib) + Erbitux (cetuximab) — Adult patients with metastatic colorectal cancer with a BRAF V600E mutation, as detected by an FDA-authorized test, in combination with cetuximab and fluorouracil-based chemotherapy (mFOLFOX6 or FOLFIRI)
FDA granted accelerated approval on 2024-12-20 based on ORR/PFS data, followed by traditional approval on 2026-02-24 after mature PFS and OS data.
Median PFS was 12.8 months with encorafenib+cetuximab+mFOLFOX6 vs. 7.1 months with standard chemotherapy (HR 0.53, 95% CI 0.41-0.68, P<0.0001). ORR was 61% vs. 40% (odds ratio 2.443).
Median OS was 30.3 months with EC+mFOLFOX6 vs. 15.1 months with SOC (HR 0.49, 95% CI 0.38-0.63, P<0.0001). Near-tripled median survival in this historically aggressive subtype.
Grade ≥3 all-cause AEs occurred in 74.0% with EC+mFOLFOX6 vs. 61.0% with SOC. Grade ≥3 treatment-related AEs: 69.7% vs. 53.9%. Safety consistent with individual component profiles; no unexpected signals. Cutaneous malignancy monitoring per BRAF inhibitor class effect.
✅ New 1L standard of care for BRAF V600E-mutant mCRC. New 1L standard of care for BRAF V600E-mutant mCRC. Near-tripled OS (30.3 vs 15.1 mo, HR 0.49) in a historically aggressive subtype. Cohort 3 (FOLFIRI backbone) is extending evidence to patients with oxaliplatin contraindications.
New translational analyses of BREAKWATER presented at ESMO GI 2026 (#ESMOGI26, Munich, Jul 1–4 2026) layer hypothesis-generating molecular biology on top of the trial's established primary OS/PFS readout above. These findings are exploratory and have not been peer-reviewed or published in a primary manuscript — they characterize subgroup consistency and resistance biology, not a new efficacy endpoint.
OS Benefit Consistent Across Molecular Subgroups
The overall survival benefit of encorafenib + cetuximab (EC), with or without FOLFOX, was reported as consistent across molecular subgroups analyzed — supporting the primary OS result (HR 0.49) as broadly applicable rather than driven by a single biomarker-defined subset.
(ESMO GI 2026, exploratory — KOL commentary)
UV-Response Pathway Activity Associated With OS Benefit
Elevated UV-response pathway activity was associated with improved OS benefit from EC/FOLFOX in this exploratory analysis — a hypothesis-generating molecular signal, not a validated predictive biomarker.
(ESMO GI 2026, exploratory — KOL commentary)
Distinct Resistance Profiles at Progressive Disease
Distinct resistance profiles were observed at the time of progressive disease (PD) when comparing EC alone vs. EC/FOLFOX — consistent with the field's broader hypothesis that adding chemotherapy to BRAF/EGFR blockade may shape a different resistance landscape than targeted therapy alone.
BREAKWATER (NCT04607421) is a Phase III randomized trial testing first-line encorafenib + cetuximab + mFOLFOX6 versus standard-of-care chemotherapy in patients with BRAF V600E-mutant metastatic colorectal cancer, sponsored by Pfizer.
What were the key efficacy results of BREAKWATER?
Median overall survival was 30.3 months with encorafenib + cetuximab + mFOLFOX6 versus 15.1 months with standard care (HR 0.49) — a near-tripling of median survival — and median progression-free survival was 12.8 versus 7.1 months (HR 0.53). Confirmed objective response rate was about 61% versus 40%. (NEJM / ASCO 2025)
Is the BREAKWATER regimen FDA approved?
Yes. The FDA granted accelerated approval on December 20, 2024, and converted it to traditional (full) approval on February 24, 2026 based on overall survival, for encorafenib with cetuximab and fluorouracil-based chemotherapy (mFOLFOX6 or FOLFIRI) in first-line BRAF V600E-mutant metastatic colorectal cancer. The Guardant360 CDx assay was co-approved as a companion diagnostic.
What is BREAKWATER Cohort 3?
Cohort 3 tested encorafenib + cetuximab + FOLFIRI (an irinotecan-based backbone) versus FOLFIRI ± bevacizumab, providing a non-oxaliplatin first-line option. Reported at ASCO GI 2026, it showed a higher response rate (about 64% vs 39%) with an early overall survival trend (HR 0.49, OS immature), extending the evidence to patients with oxaliplatin contraindications.
What did the ESMO GI 2026 translational analysis of BREAKWATER show?
Exploratory, hypothesis-generating analyses presented at ESMO GI 2026 reported that the OS benefit was consistent across molecular subgroups, that elevated UV-response pathway activity was associated with greater OS benefit, and that distinct resistance profiles emerged at progression. These findings are not peer-reviewed and are not a new efficacy endpoint.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 5, 2026.