PALOMA-3 is a Phase 3 trial of the CDK4/6 inhibitor palbociclib (Ibrance) plus fulvestrant versus fulvestrant alone in HR-positive, HER2-negative metastatic breast cancer that progressed on prior endocrine therapy. Palbociclib-fulvestrant more than doubled median progression-free survival (9.5 vs 4.6 months; HR 0.46) and improved overall survival (34.8 vs 28.0 months; HR 0.81). The regimen is FDA-approved. Sponsor: Pfizer.
Discover KOL Sentiment on PALOMA-3 →Design — Phase 3, randomized (2:1), double-blind; palbociclib (Ibrance) + fulvestrant vs placebo + fulvestrant, HR+/HER2- metastatic breast cancer after prior endocrine therapy (NCT01942135). (NEJM / Lancet Oncol)
PFS (primary) — Median 9.5 vs 4.6 months at final analysis (HR 0.46; 95% CI 0.36-0.59); interim analysis 9.2 vs 3.8 months (HR 0.42; p<0.000001). (NEJM, Turner et al.)
Overall survival — Median 34.8 vs 28.0 months with 73.3-month follow-up (stratified HR 0.81; 95% CI 0.65-0.99); 6-year OS 19.1% vs 12.9%. (Lancet Oncol / extended follow-up)
Subgroup — OS benefit most pronounced in endocrine-sensitive disease and patients without prior chemotherapy; ctDNA (ESR1/PIK3CA) biomarker analyses reported. (Lancet Oncol)
Safety — Neutropenia most common AE: 83% all-grade (Grade 3 55%, Grade 4 11%); febrile neutropenia rare (0.9-1.8%). (NEJM / label)
Regulatory / Sponsor — FDA approved (Ibrance + fulvestrant, HR+/HER2- advanced breast cancer after endocrine therapy). Pfizer. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.



















Top 10 by impressions - click to view on X
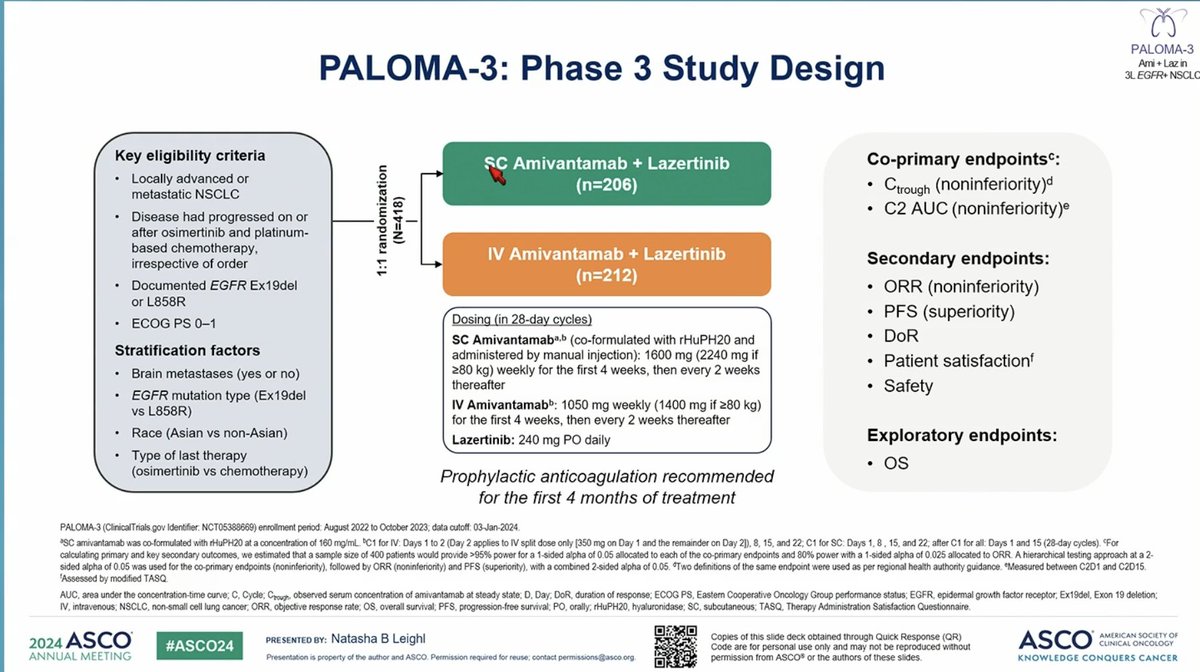
Dr. Natasha Leighl now reviews data from the PALOMA-3 Trial at #ASCO24 Very excited to hear about this data regarding subcutaneous amivantamab-- a real potential to transform the...
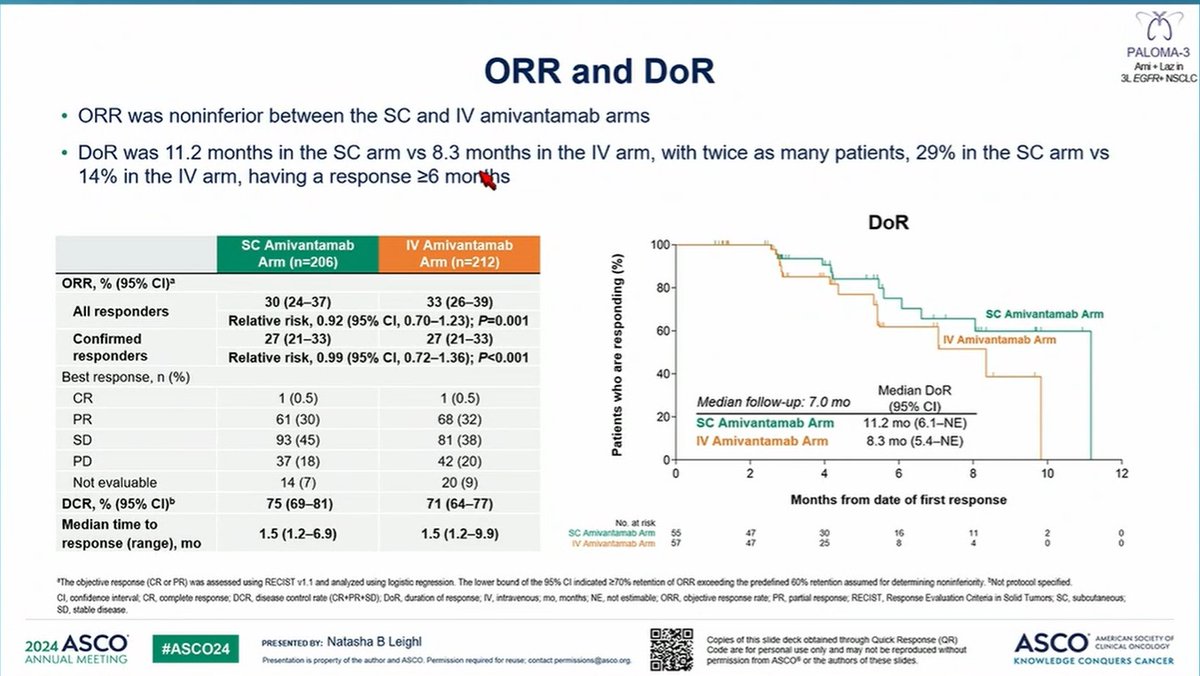
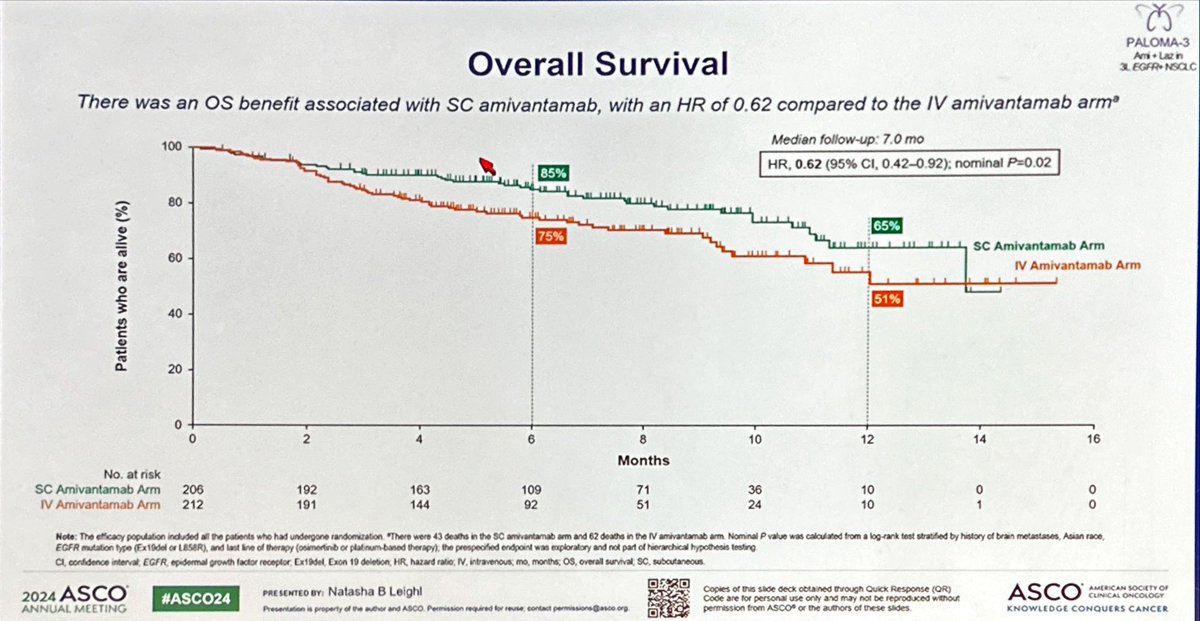
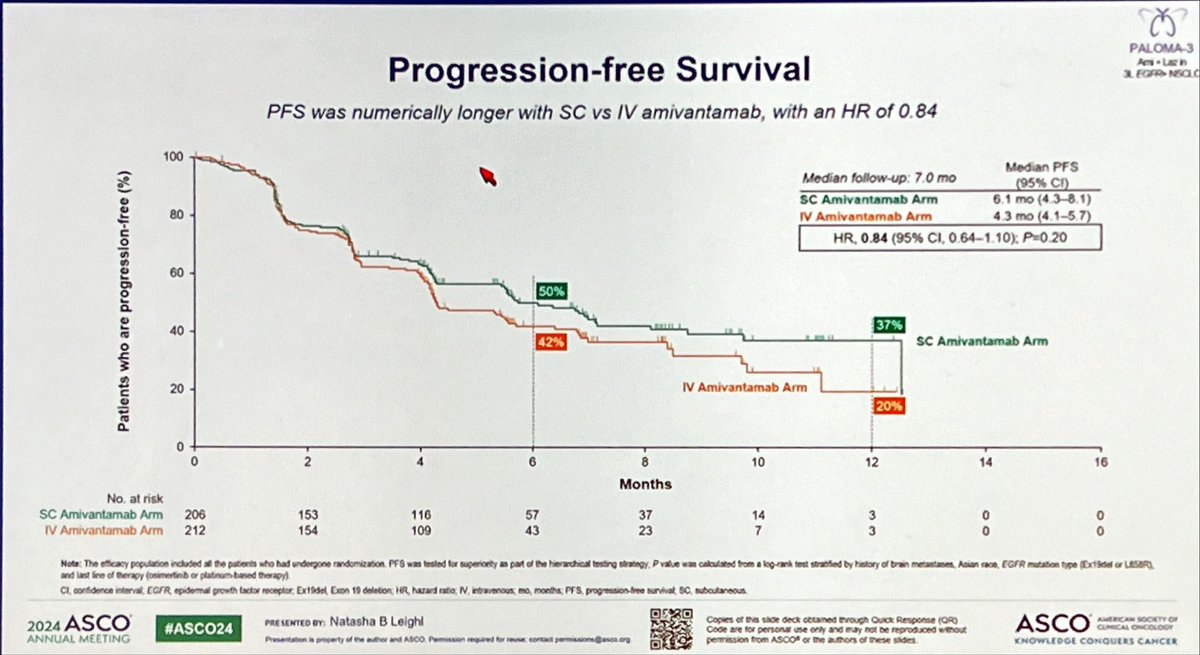
#ASCO24 PALOMA-3 trial: SC amivantamab vs IV amivantamab (both in combination with lazertinib) 💥SC ami demonstrated noninferior PK and ORR compared to IV 📌 PFS and OS➡️longer in the...
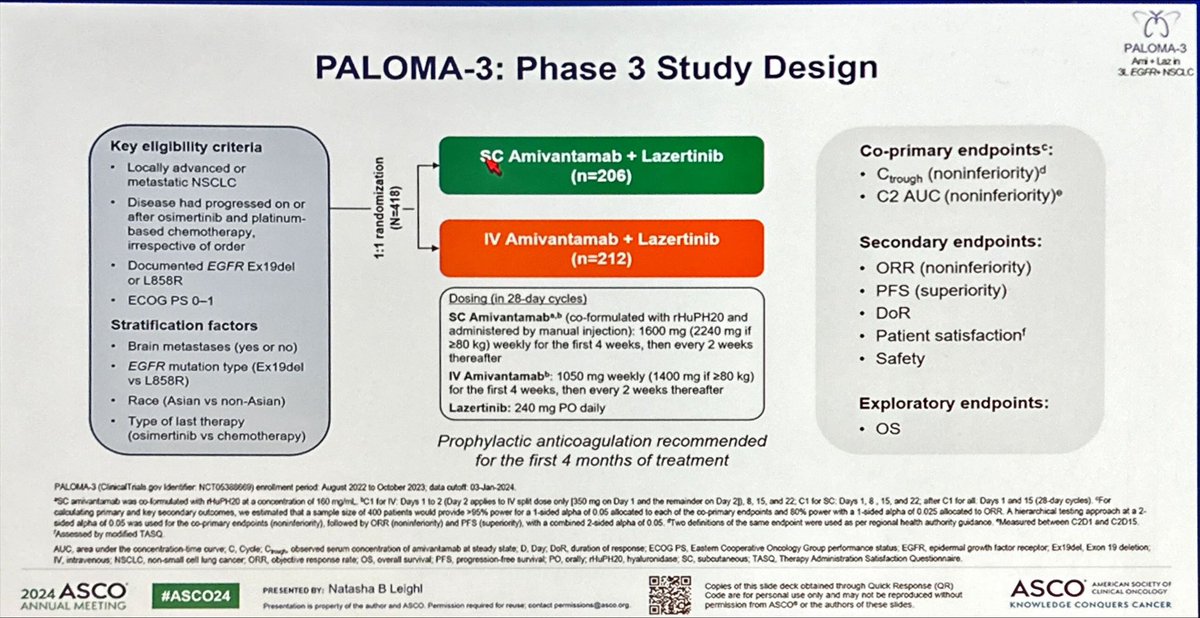
Some #LBAs already out! ➡️ PALOMA-3 (NCT05388669): SC amivantamab (ami) + lazertinib (laz) vs IV ami + laz in EGFR-mutated advanced NSCLC. 📊 Results: - Noninferior PK &...
#lungcancer RCT of Subcutaneous versus I.V. Amivantamab (EGFR bispecific) in PALOMA-3 presented by Dr Leigh’s #ASCO24. Non-inferior for safety, efficacy + intriguing...
Can’t wait to hear more about PALOMA-3 TODAY at #ASCO24 Subcutaneous Amivantamab has the potential to ⬇️ infusion-related reactions & clinic visits/time that patients have...
$JNJ flies towards a more convenient Rybrevant, but has a long way to go before this is a $5bn product #ASCO24 via @ApexOnco
Can’t wait to hear more about PALOMA-3 TODAY at #ASCO24 Subcutaneous Amivantamab has the potential to ⬇️ infusion-related reactions & clinic visits/time that patients have...
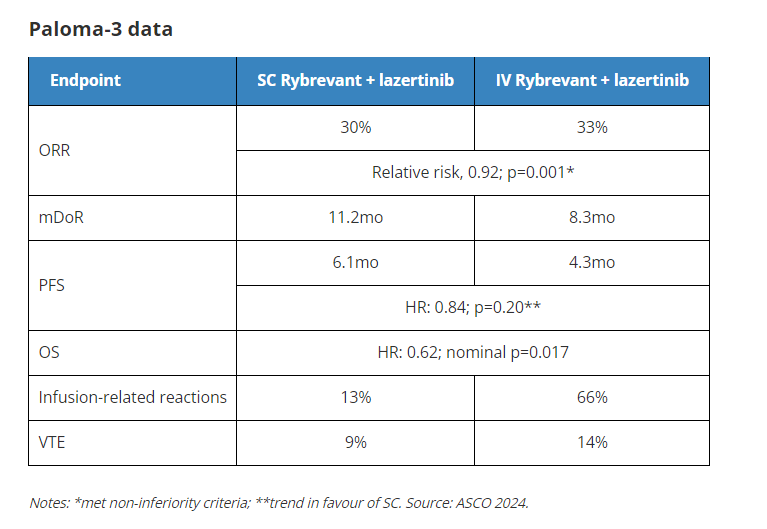
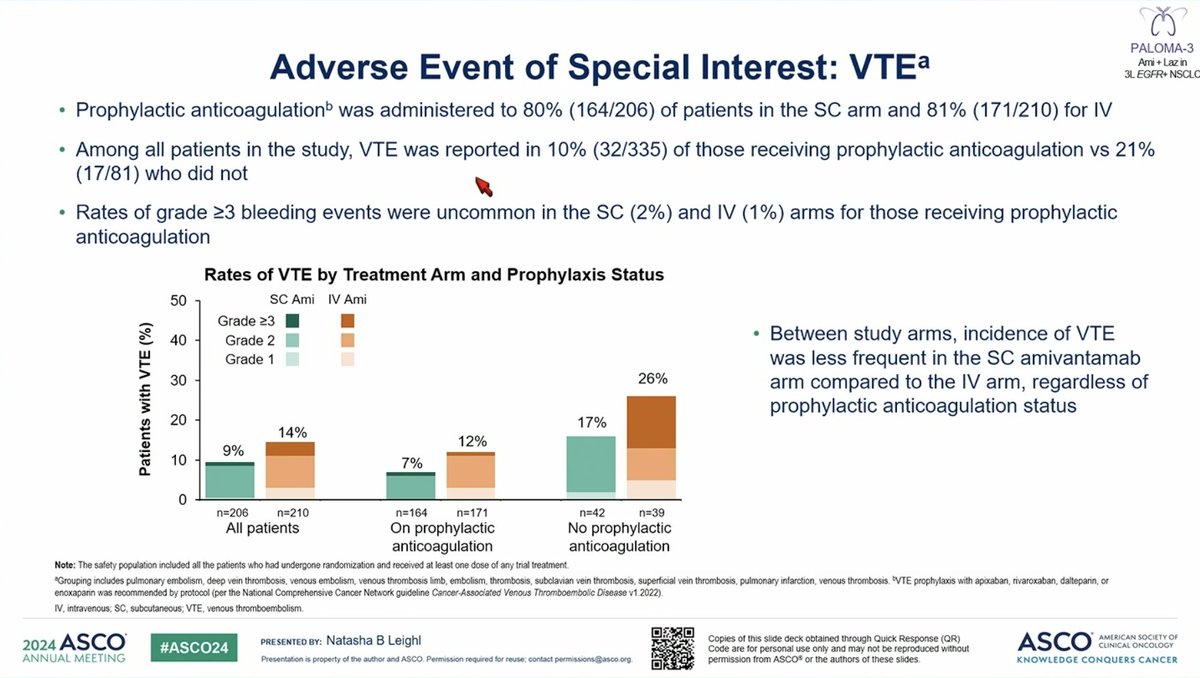
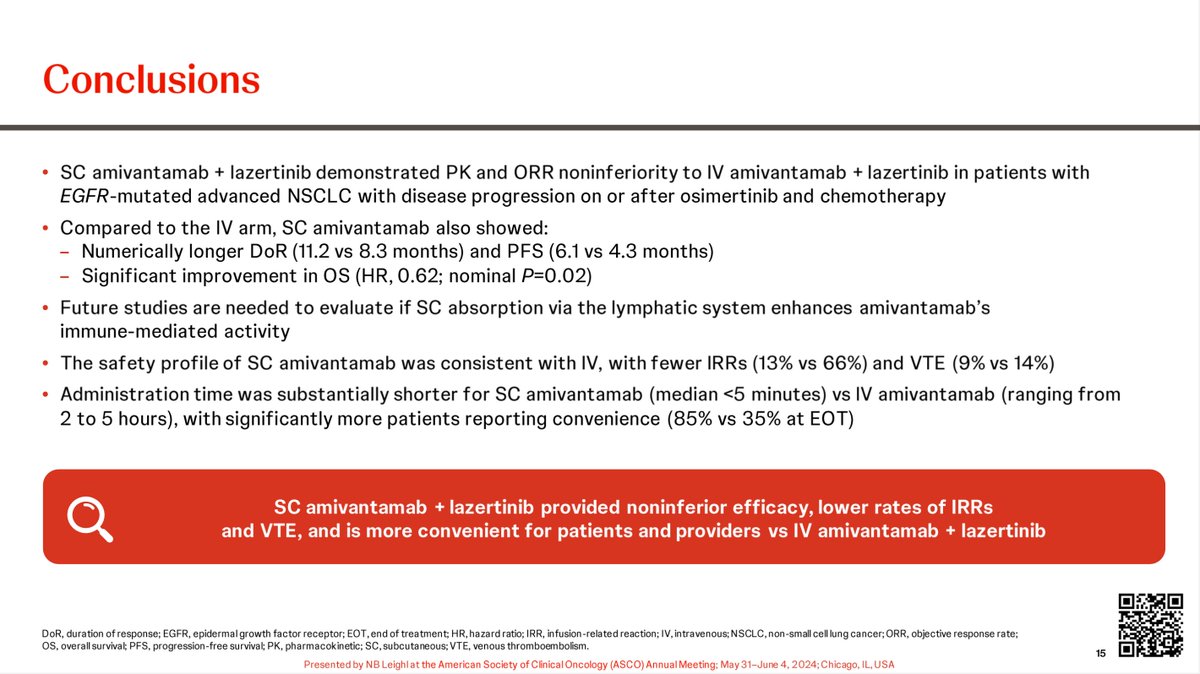
PALOMA-3 trial: SC vs. IV amivantamab + lazertinib in EGFR-mutant NSCLC. Similar ORRs, numerically better PFS, improved OS with SC vs. IV. Significant reduction in IRRs with SC vs. IV (shorter...

Compelling data presented today from the PALOMA-3 trial (amivantamab) in EFGR mutant NSCLC #LCSM SC administration wins over IV and reduces burden on patients by reducing adelverse...

PALOMA-3 SubQ vs I. Ami+lazer in post osi, post chemo setting (Dr Leighl). PK non-inferiority endpoints met. ORR non inferior. DOR and PFS and OS (sign) improved for SC. TRAEs similar between arms....
PALOMA-3 is the pivotal Phase III, randomized, double-blind, placebo-controlled trial that established palbociclib (Ibrance) plus fulvestrant as a standard of care for women with HR+/HER2- advanced or metastatic breast cancer whose disease progressed on prior endocrine therapy. The trial enrolled 521 women regardless of menopausal status and demonstrated a clinically meaningful and statistically significant PFS benefit that has been supported by over 6 years of follow-up data including ctDNA biomarker analyses.
Phase III, international, multicenter, 2:1 randomized, double-blind, placebo-controlled trial (NCT01942135). Patients received palbociclib 125 mg daily (3 weeks on, 1 week off) plus fulvestrant 500 mg IM, or matching placebo plus fulvestrant. Pre- and perimenopausal women also received concurrent goserelin (LHRH agonist). Stratified by sensitivity to prior hormonal therapy, menopausal status, and presence of visceral metastases.
Women of any menopausal status with HR+/HER2- advanced or metastatic breast cancer whose disease progressed on or after prior endocrine therapy. Patients must have had documented disease progression during or after endocrine therapy. Up to one prior line of chemotherapy for advanced disease was permitted. ER-positive and/or PR-positive (1% or greater staining), HER2-negative by IHC or ISH.
Palbociclib 125 mg orally daily for 21 days of every 28-day cycle plus fulvestrant 500 mg IM on Days 1 and 15 of Cycle 1, then every 28 days. Versus matching placebo plus fulvestrant on the same schedule.
Primary endpoint: investigator-assessed PFS (RECIST 1.1). Key secondary endpoints: OS, ORR, DoR, CBR (CR/PR/SD 24 weeks or more), safety, pharmacokinetics, and patient-reported outcomes including time to deterioration in pain.
Palbociclib plus fulvestrant demonstrated a clinically meaningful and statistically significant PFS improvement. At the interim analysis, median PFS was 9.2 months vs. 3.8 months (HR 0.42; 95% CI: 0.32-0.56; p<0.000001). At the final PFS analysis, median PFS was 9.5 months vs. 4.6 months (HR 0.46; 95% CI: 0.36-0.59; p<0.000001). ctDNA analyses showed PFS benefit regardless of ESR1 (HR 0.25 for ESR1-mutated), PIK3CA, or TP53 mutation status.
With extended follow-up of 73.3 months, palbociclib plus fulvestrant maintained a clinically meaningful OS benefit. Median OS was 34.8 months (95% CI: 28.8-39.9) vs. 28.0 months (95% CI: 23.5-33.8) (stratified HR 0.81; 95% CI: 0.65-0.99). 5-year OS rate: 23.3% vs. 16.7%. 6-year OS rate: 19.1% vs. 12.9%. In patients without prior chemotherapy for ABC, median OS was 39.3 months vs. 29.7 months (HR 0.72; 95% CI: 0.55-0.94). The earlier protocol-specified final OS analysis (median follow-up 44.8 months) showed median OS of 34.9 vs. 28.0 months (HR 0.81; 95% CI: 0.64-1.03; p=0.0429), which did not reach the prespecified significance threshold. Patients with ESR1 mutations showed OS HR 0.59 (95% CI: 0.37-0.94).
The safety profile was generally tolerable with adverse reactions manageable through dose modifications. Neutropenia was the most common AE: 83% all-grade (Grade 3: 55%, Grade 4: 11%). Febrile neutropenia was rare (0.9-1.8%). Other common AEs: leukopenia 53%, infections 47%, fatigue 41%, nausea 34%, anemia 30%, stomatitis 28%. Permanent discontinuation due to AEs: 6% (palbociclib) vs. 3% (placebo). One death from neutropenic sepsis was recorded. QoL was maintained or improved; median time to deterioration in pain was 8.0 months vs. 2.8 months (HR 0.642; p<0.001).
PALOMA-3 established palbociclib plus fulvestrant as a standard of care for HR+/HER2- mBC after prior endocrine therapy. The extended 6-year follow-up confirmed a clinically meaningful OS benefit, particularly in patients without prior chemotherapy and those with endocrine-sensitive disease. The ctDNA biomarker analyses revealed that ESR1-mutated patients derive the greatest benefit (PFS HR 0.25, OS HR 0.59), suggesting a potential role for liquid biopsy-guided treatment selection. Key debate: while no OS benefit was formally significant at the protocol-specified analysis, the consistent trend with extended follow-up and the OS benefit in the no-prior-chemotherapy subgroup support CDK4/6 inhibitor therapy in this setting.
PALOMA-3 (NCT01942135) is a Phase 3, randomized (2:1), double-blind trial of the CDK4/6 inhibitor palbociclib (Ibrance) plus fulvestrant versus placebo plus fulvestrant in patients with HR-positive, HER2-negative metastatic breast cancer whose disease progressed on prior endocrine therapy. It was sponsored by Pfizer.
Palbociclib plus fulvestrant significantly improved progression-free survival, with a final median PFS of 9.5 versus 4.6 months (HR 0.46). With extended 73.3-month follow-up, median overall survival was 34.8 versus 28.0 months (stratified HR 0.81; 95% CI 0.65-0.99), a clinically meaningful benefit most pronounced in endocrine-sensitive disease.
Yes. Palbociclib (Ibrance) in combination with fulvestrant is FDA approved for HR-positive, HER2-negative advanced or metastatic breast cancer with disease progression following endocrine therapy. That fulvestrant-combination indication was approved in February 2016 and was supported by PALOMA-3; Ibrance was first approved (with letrozole) in February 2015.
PALOMA-3 established palbociclib plus fulvestrant as a standard of care for HR-positive, HER2-negative metastatic breast cancer after progression on prior endocrine therapy, helping to define the CDK4/6-inhibitor-plus-endocrine-therapy paradigm that is now central to management of this disease.
The most common adverse event was neutropenia, occurring in about 83% of patients (Grade 3 in 55%, Grade 4 in 11%), but febrile neutropenia was rare (0.9-1.8%). Other common events included leukopenia, infections, fatigue, nausea and anemia; toxicity was generally managed with dose modifications.






























