FLAURA is the landmark Phase 3 trial that established osimertinib (Tagrisso) as the preferred first-line EGFR TKI in EGFR-mutant advanced NSCLC. Versus gefitinib or erlotinib, osimertinib nearly doubled PFS (18.9 vs 10.2 months; HR 0.46) and significantly improved overall survival (38.6 vs 31.8 months; HR 0.80). FDA approved April 18, 2018. Sponsor: AstraZeneca.
Discover KOL Sentiment on FLAURA →Design — Phase 3, double-blind; 1L osimertinib 80 mg vs gefitinib/erlotinib, EGFR-mutant advanced NSCLC, n=556 (NCT02296125). (NEJM)
PFS (primary) — Median 18.9 vs 10.2 months; HR 0.46 (95% CI 0.37-0.57; p<0.0001) — 54% reduction in progression/death; ORR 80% vs 76%. (NEJM)
Overall survival — Median 38.6 vs 31.8 months; HR 0.80 (95% CI 0.64-1.00; p=0.0462). (NEJM 2020, 57.7% maturity)
Safety — Generally well tolerated; Grade 3 AEs 9.7%, Grade 4 0.9%; ILD/pneumonitis 3.9% (0.4% fatal). (NEJM)
Regulatory — FDA approved April 18, 2018; first 3rd-gen EGFR TKI first-line; NCCN preferred (companion Dx cobas EGFR). (FDA.gov)
Sponsor / Drug — AstraZeneca; osimertinib (Tagrisso), a 3rd-generation EGFR TKI, 80 mg daily. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.













Top 10 by impressions - click to view on X
FLAURA2 press release: addition of chemotherapy to 1L osimertinib in #EGFR NSCLC improves overall survival. Already approved based on significant PFS benefit. Awaiting data to see...
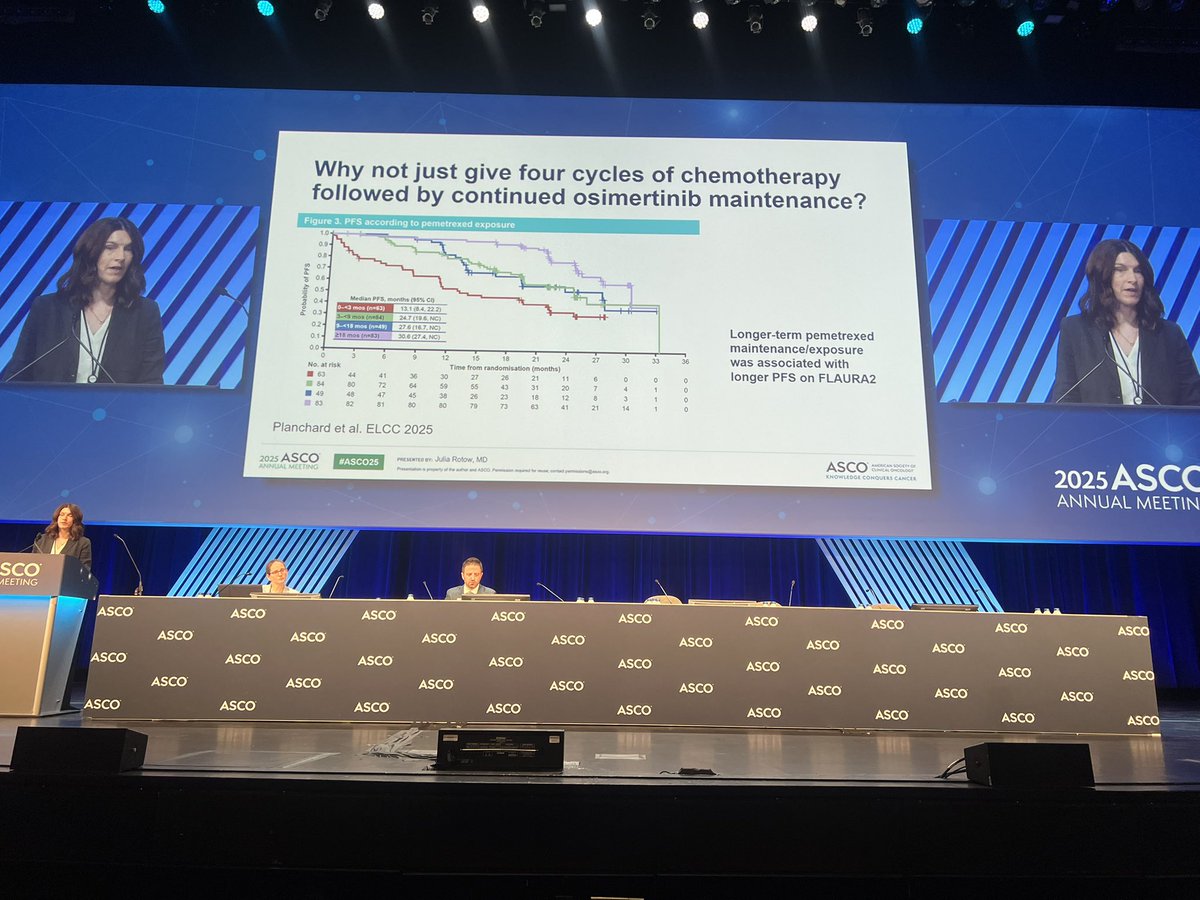
So important to remember - continuation of pemetrexed maintenance on the #FLAURA2 likely is required to derive benefit! @JuliaRotow @asco #ASCO25...
@MassimoDiMaio75 Love how the response is that "data suggest that the greatest overall survival benefit is achieved with the use of adjuvant osimertinib, as supported by the results of...
Always love hearing @JuliaRotow speak! Great to spend time with her in NOLA! BOOKMARK her updated slide! 🔖
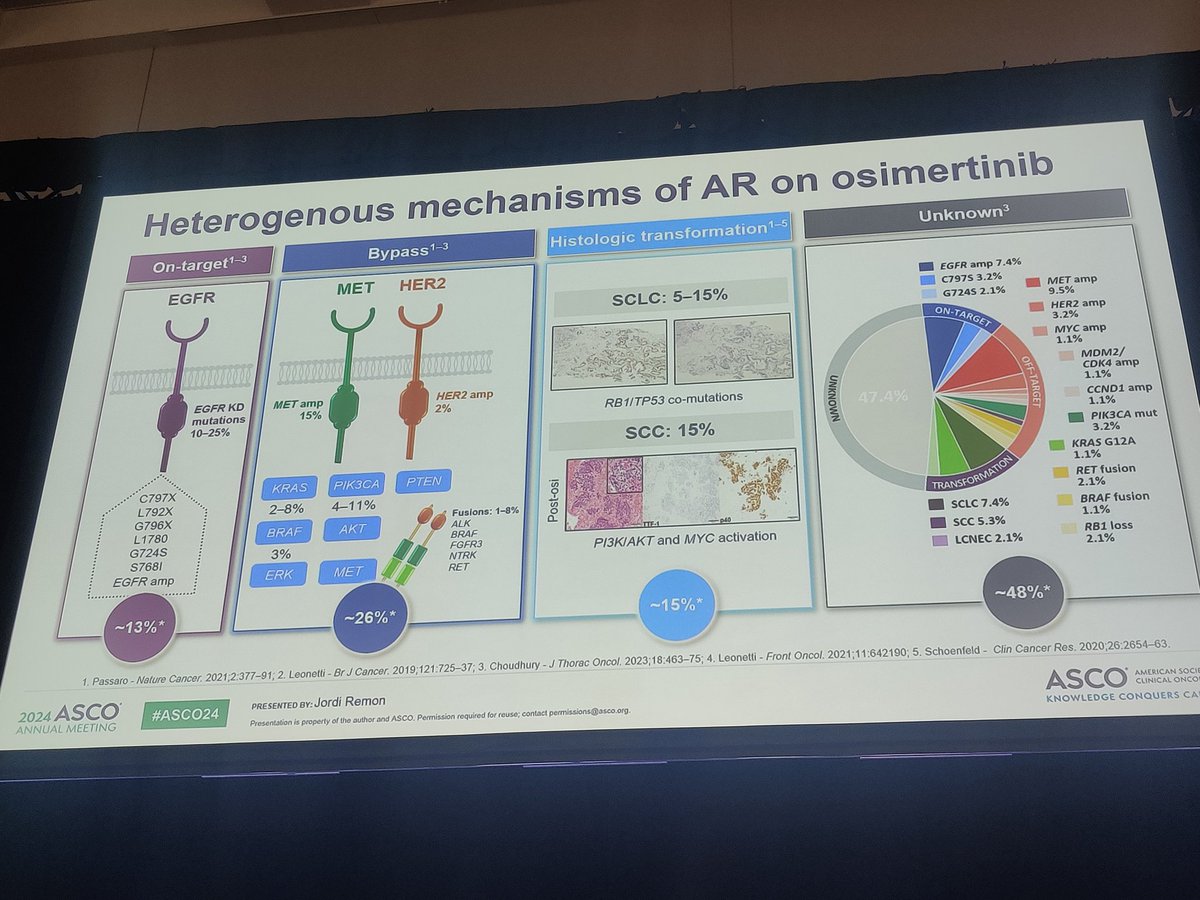
#ASCO24 Masterclass by @JordiRemon mechanisms of resistance to #EGFR #NSCLC 1. On-target 🎯 2. Bypass 👣 3. Histo transf...
@dr_yakupergun @SuyogCancer @myESMO @BalazsHalmosMD @Alfdoc2 @5_utr @StephenVLiu @ADesaiMD @FordePatrick...
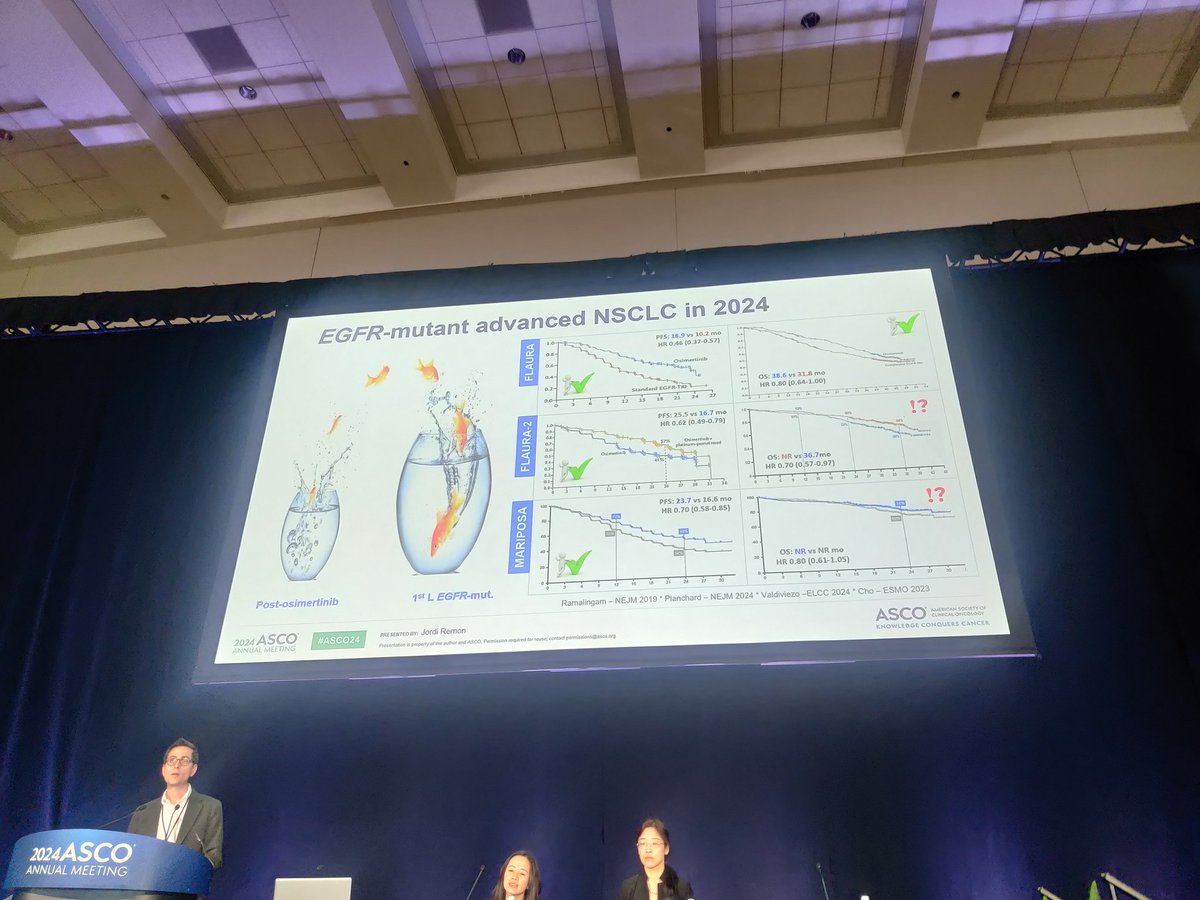
Dr. @LuisPaz_Ares discusses 1L #EGFR NSCLC at #ITCD2024 - osimertinib is our standard but as most patients see progression within 2 years, need better...

@FordePatrick After FLAURA and ADAURA, we would have expected LAURA to be positive for both PFS and OS. This press release is very encouraging!

@SuyogCancer @myESMO @Alfdoc2 @dr_yakupergun @5_utr @StephenVLiu @ADesaiMD @FordePatrick @n8pennell It will take a lot...

@ArianaPantasy @Banana_Oncology It's my understanding that Astra positions FLAURA2 only for subpopulations like pts with brain mets or other subgroups of...
FLAURA is the landmark Phase III trial that established osimertinib (Tagrisso) as the preferred first-line EGFR TKI for patients with EGFR-mutant advanced NSCLC. The double-blind, active-controlled trial randomized 556 treatment-naive patients 1:1 to osimertinib 80 mg daily versus standard-of-care gefitinib or erlotinib. FLAURA demonstrated both a near-doubling of PFS and a statistically significant overall survival benefit, fundamentally changing the first-line treatment paradigm for EGFR-mutant NSCLC and earning NCCN preferred status as the only Category 1 preferred EGFR TKI.
Phase III, multicenter, international, randomized, double-blind, active-controlled trial (NCT02296125) in 556 patients with previously untreated, locally advanced or metastatic EGFR-mutant NSCLC. EGFR mutations detected by FDA-approved companion diagnostics: cobas EGFR Mutation Test v2 or FoundationOne CDx.
Adults with newly diagnosed, treatment-naive, unresectable or metastatic (Stage IV) NSCLC harboring EGFR exon 19 deletions or exon 21 L858R mutations, WHO performance status 0-1. Stable CNS metastases were permitted. Two-thirds of enrolled patients were women.
Osimertinib 80 mg orally once daily versus standard-of-care gefitinib 250 mg or erlotinib 150 mg orally once daily. Crossover to osimertinib was permitted upon progression with T790M positivity; 20-31% of control arm patients crossed over.
Primary endpoint: investigator-assessed progression-free survival (PFS). Key secondary endpoints: overall survival (OS), objective response rate (ORR), duration of response (DoR). Preplanned exploratory analysis: CNS PFS, CNS ORR, and CNS duration of response in patients with baseline brain metastases.
Osimertinib nearly doubled median PFS: 18.9 months vs 10.2 months (HR 0.46; 95% CI: 0.37-0.57; p<0.0001), representing a 54% reduction in the risk of progression or death. Confirmed ORR was 80% vs 76%, with median duration of response of 17.6 vs 9.6 months. PFS benefit was observed in patients with and without baseline brain metastases.
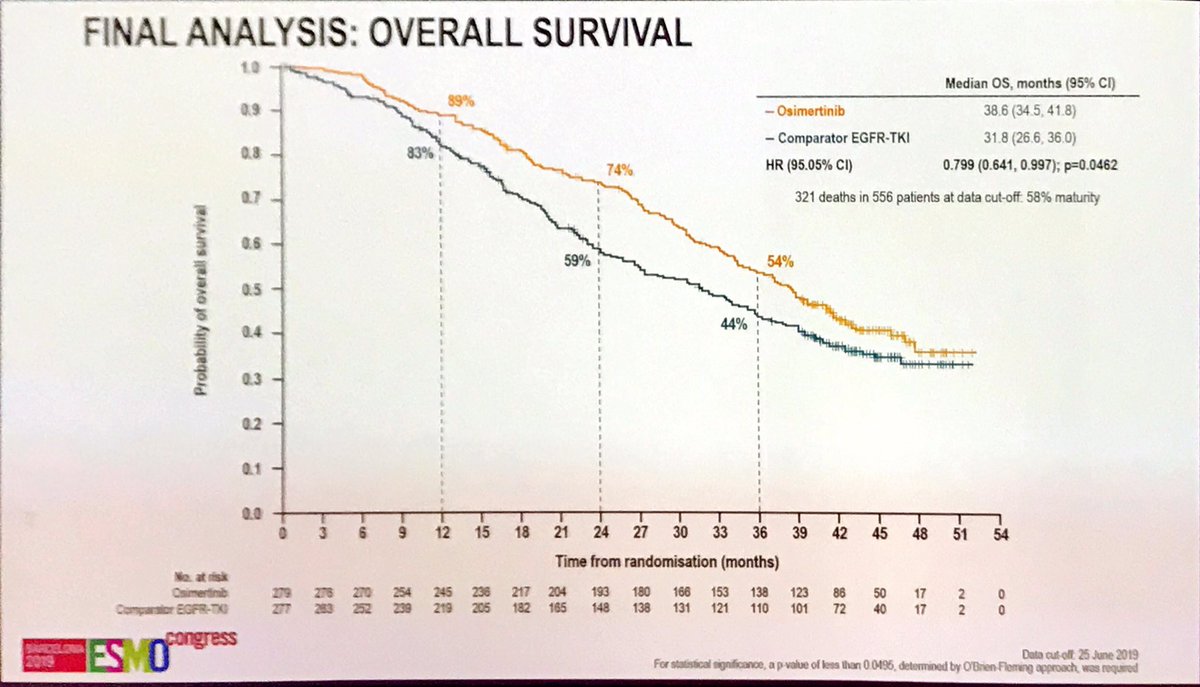
At a later data cut-off (57.7% maturity), osimertinib demonstrated a statistically significant OS benefit: median OS 38.6 months vs 31.8 months (HR 0.80; 95% CI: 0.64-1.00; p=0.0462), a 21% relative improvement in survival. At 3 years, 54% of osimertinib patients were alive vs 44% in the control arm. This OS benefit was achieved despite 20-31% of control patients crossing over to osimertinib, which drove one of the highest control-arm survival rates ever reported for first-generation TKIs.
Osimertinib was generally well tolerated. Most AEs were Grade 1-2 in severity. Grade 3 AEs occurred in 9.7% and Grade 4 in 0.9% of osimertinib-treated patients. ILD/pneumonitis occurred in 3.9% (0.4% fatal). QTc prolongation >60 msec from baseline in 3.6%, QTc >500 msec in 0.9%, with no QTc-related arrhythmias. Most common AEs (>=20%): diarrhea, rash, dry skin, nail toxicity, stomatitis, fatigue, decreased appetite. Permanent discontinuation due to AEs was 4.3%.
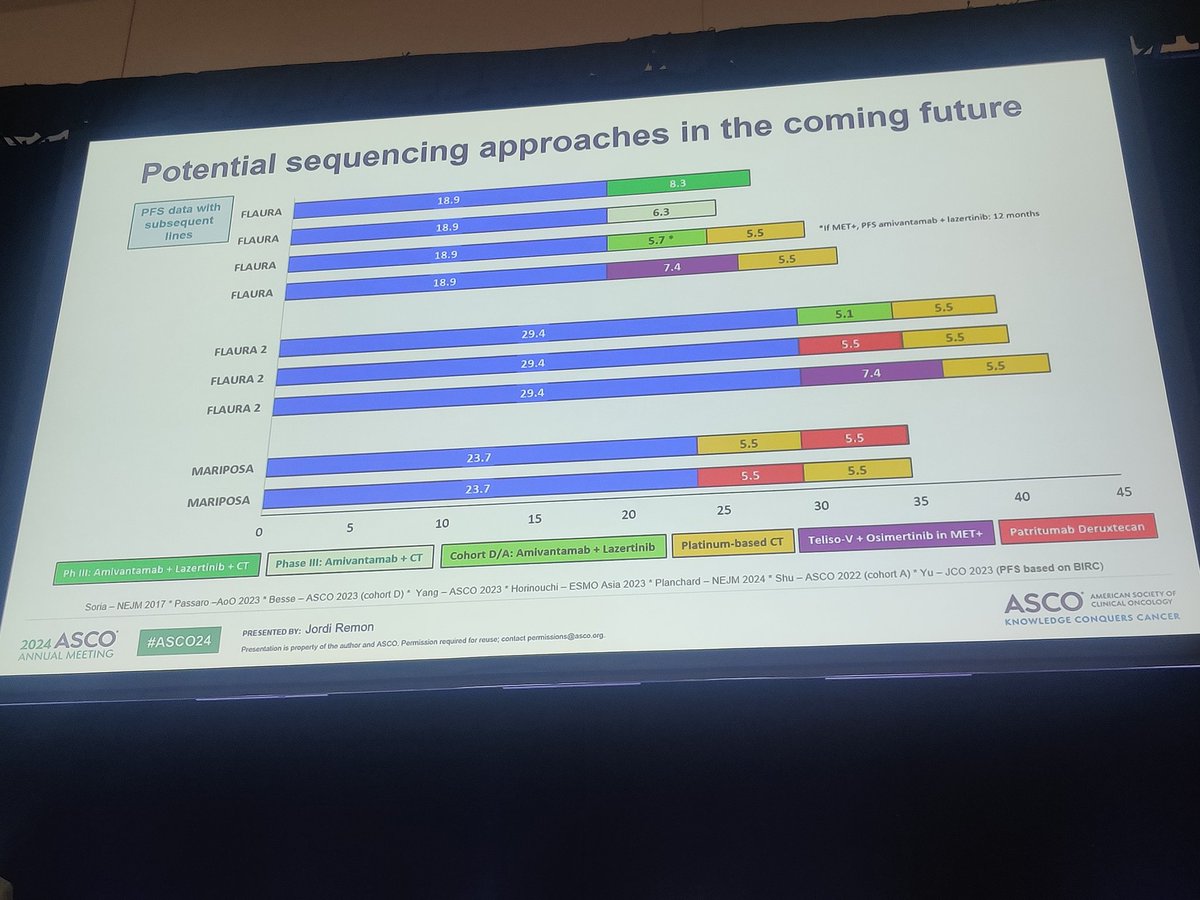
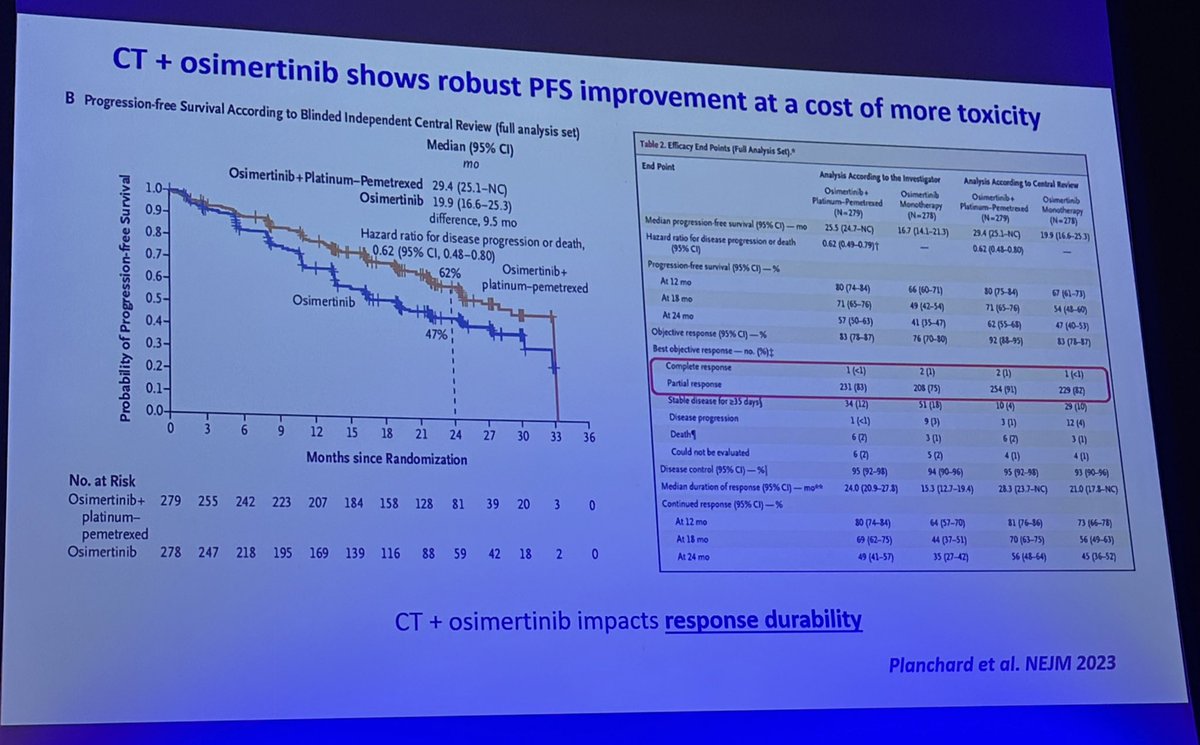
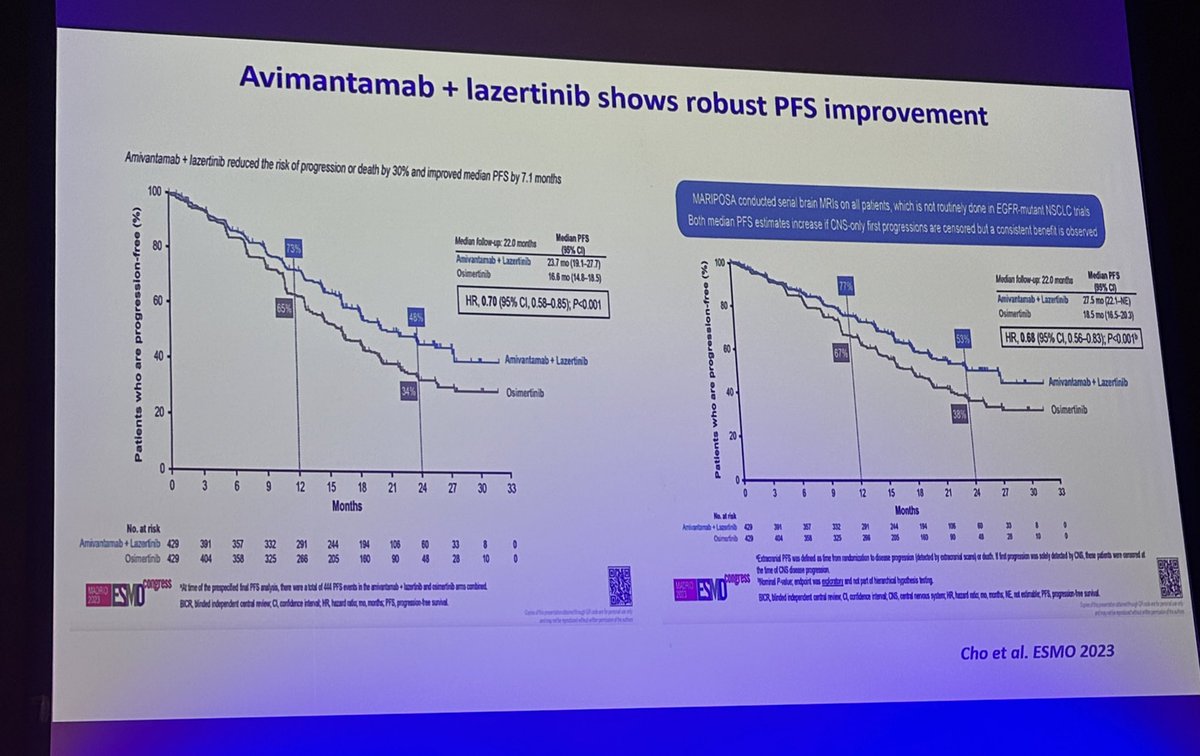
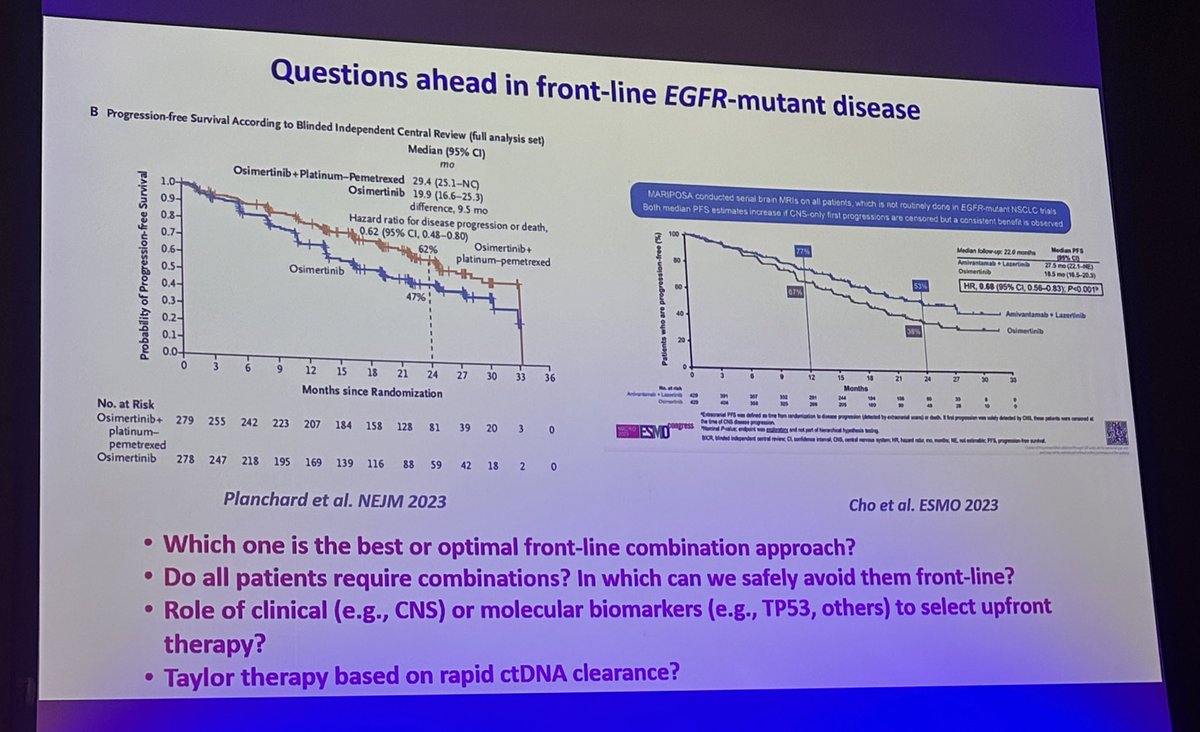
FLAURA established osimertinib as the undisputed first-line standard of care for EGFR-mutant advanced NSCLC, with both PFS and OS benefits plus superior CNS activity. The trial demonstrated that the best agent should be given first-line rather than sequenced, since ~30% of patients never received subsequent therapy. Key ongoing debates include: (1) FLAURA2 showed osimertinib + chemotherapy extends OS to 47.5 months, raising the question of mono vs. combo therapy; (2) MARIPOSA offers amivantamab + lazertinib as an alternative combo; (3) post-osimertinib resistance mechanisms beyond T790M require new strategies; (4) patient selection for mono vs. combo based on disease burden, CNS involvement, and mutation type.
FLAURA is a landmark Phase 3, double-blind, active-controlled trial (NCT02296125) that randomized 556 treatment-naive patients with EGFR-mutant advanced NSCLC to first-line osimertinib (Tagrisso) versus standard-of-care gefitinib or erlotinib.
Yes. On April 18, 2018 the FDA approved osimertinib (Tagrisso) for the first-line treatment of metastatic NSCLC with EGFR exon 19 deletion or exon 21 L858R mutations. It was the first third-generation EGFR TKI approved in the first-line setting and became the only NCCN preferred first-line EGFR TKI.
Osimertinib nearly doubled median progression-free survival to 18.9 months versus 10.2 months with gefitinib or erlotinib (HR 0.46; 95% CI 0.37-0.57; p<0.0001), a 54% reduction in the risk of progression or death. Confirmed objective response rate was 77% versus 69%.
Yes. At a later data cut-off (57.7% maturity), osimertinib demonstrated a statistically significant overall survival benefit: median OS 38.6 months versus 31.8 months (HR 0.80; 95% CI 0.64-1.00; p=0.0462), a 21% relative improvement in survival.
Osimertinib (Tagrisso) is a third-generation, CNS-active EGFR tyrosine kinase inhibitor developed by AstraZeneca.




















