High-risk smoldering multiple myeloma - Janssen
Discover KOL Sentiment on AQUILA →










Top 10 by impressions - click to view on X
This is likely the breaking news of the day at #ASH24 Aquila soars high, Hope in smoldering shadows, New light breaks the dark. @ASH_hematology @TheIACH...
AQUILA trial for high risk smoldering myeloma published in @NEJM today. @thanosdimop Personally for me, it is a huge milestone along 25 years of work that started in 1998....
Ridiculous. Super expensive drug to treat healty people who feel just fine, the primary endpoint includes slim criteria. Even PFS2 may include asymptomatic events. An industry sponsored joke....
Dr Rajkumar I respect you for all you have done (way more than me for field of myeloma by a billion) but strongly disagree. If the care in a control arm in a clinical trial strongly deviates from...
Just out: Paradigm changing AQUILA randomized trial in high risk smoldering myeloma #ASH24 @thanosdimop @NEJM Daratumumab significantly prolongs time to active...
AQUILA Trial is out! Important to note that ~30% of patients received a clearly suboptimal 1st line anti-myeloma treatment (no PI+IMiD- based triplet or CD38-based combos), which makes the OS signal...
Why we are not ready to treat smoldering myeloma! This paper explains it all. Free download.
Oncology Poll We now have a randomized trial showing Daratumumab improves OS and delays progression. As an oncologist are you going to start treating high risk smoldering myeloma or are you not...
Yes and how many on the control arm never ever got a cd38 antibody.

As I mentioned y'day... FDA questioning the benefit-risk of $JNJ $GMAB Darzalex in smoldering myeloma. This is from the FDA's review, posted this morning.
AQUILA is a phase 3, randomized, open-label, multicenter trial (NCT03301220) evaluating subcutaneous daratumumab (Darzalex Faspro) monotherapy versus active monitoring in patients with high-risk smoldering multiple myeloma. The trial enrolled 390 patients and demonstrated that daratumumab significantly delayed progression to active myeloma. FDA approved November 6, 2025 - the first treatment for smoldering myeloma.
Phase 3, randomized, open-label, multicenter trial comparing subcutaneous daratumumab monotherapy versus active monitoring in patients with high-risk smoldering multiple myeloma.
Adults with high-risk smoldering MM. 41% met 2+ criteria: serum monoclonal protein >2 g/dL, involved-to-uninvolved serum-free light chain ratio >20, and bone marrow plasma cells >20%.
Darzalex Faspro 1,800 mg/30,000 units SC - weekly (wks 1-8), every 2 weeks (wks 9-24), then every 4 weeks until 39 cycles (up to 36 months) versus active monitoring.
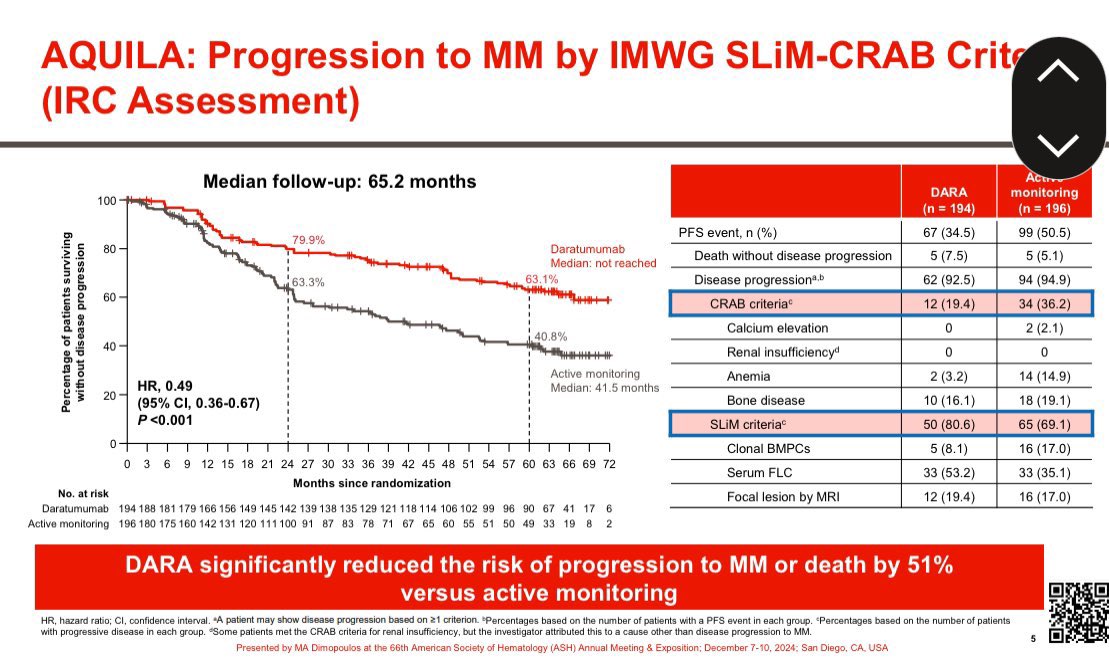
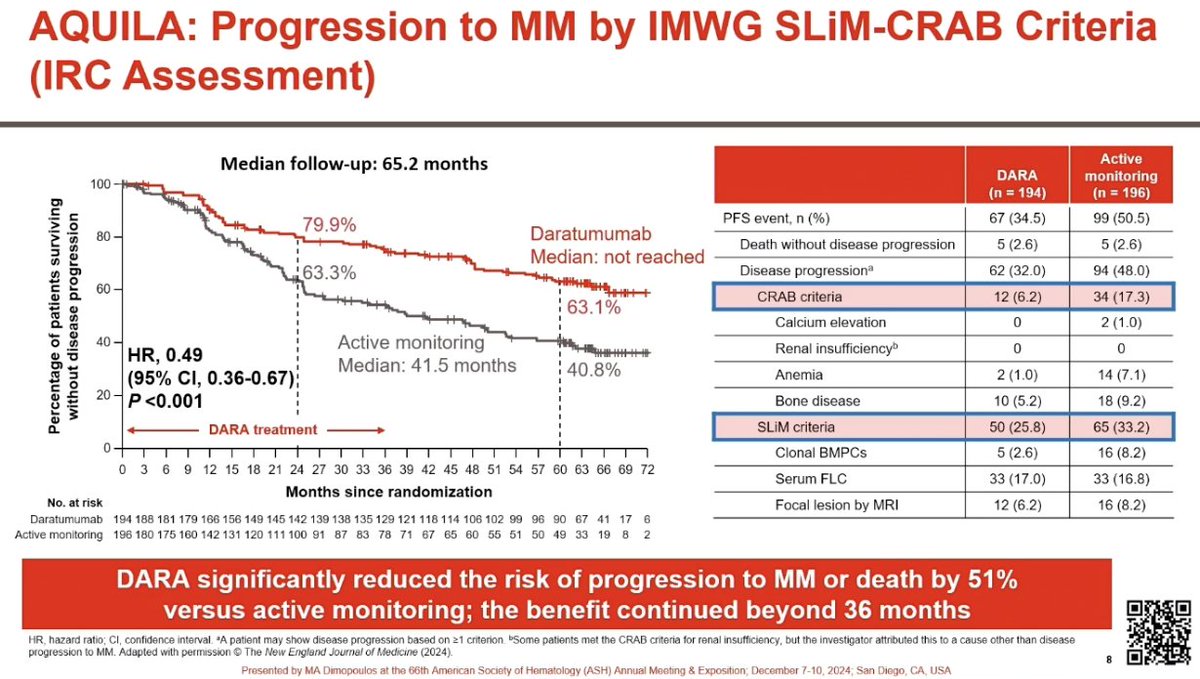
Progression-free survival (PFS) by independent review committee, defined as progression to active MM (IMWG SLiM-CRAB criteria) or death.
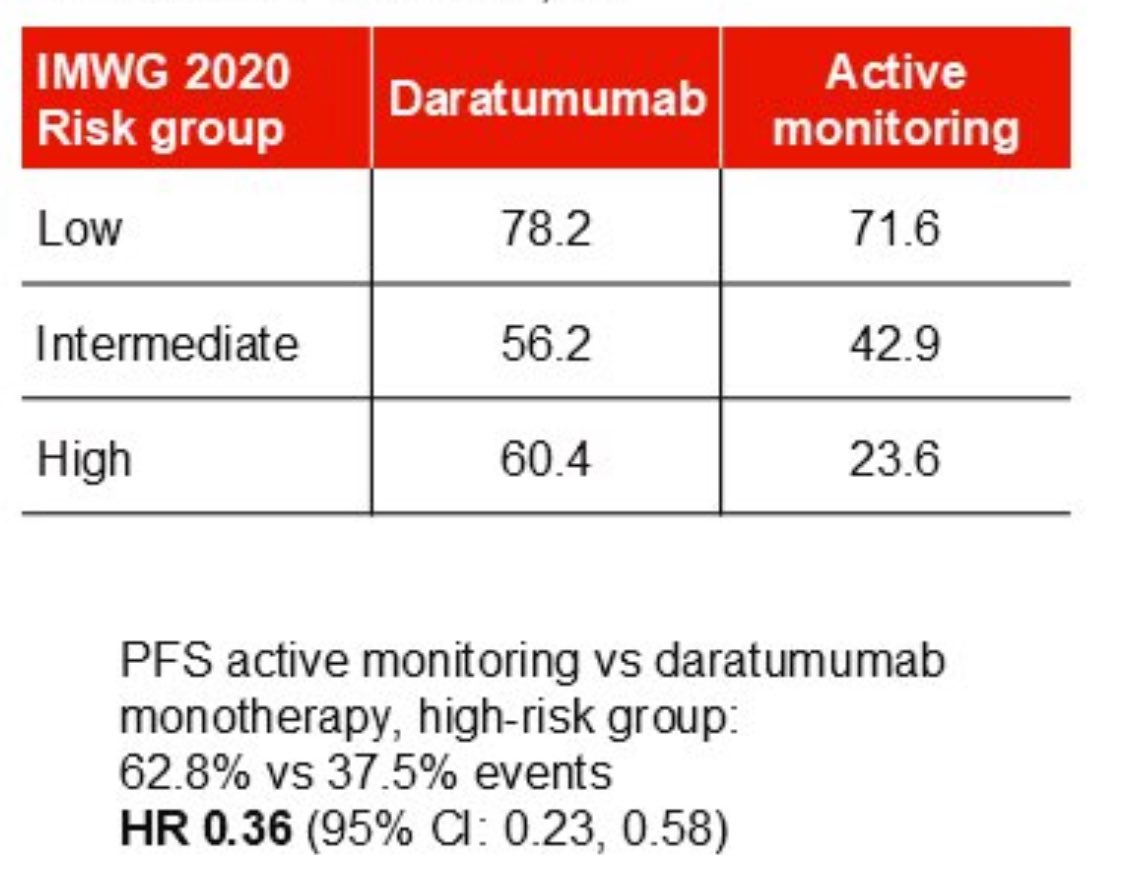
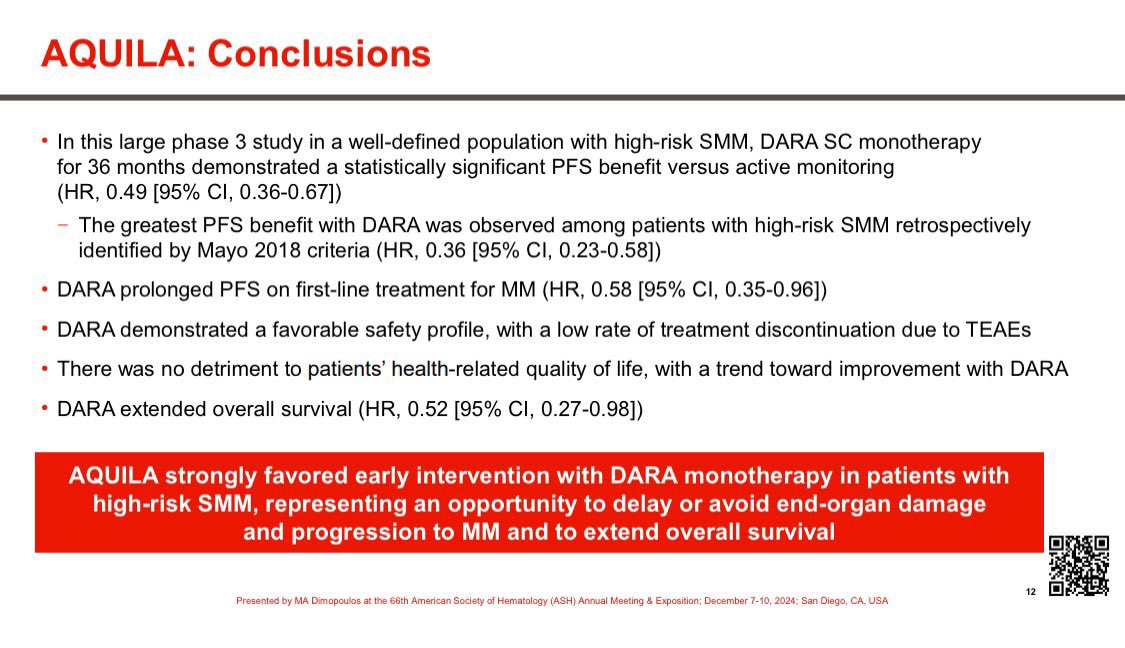
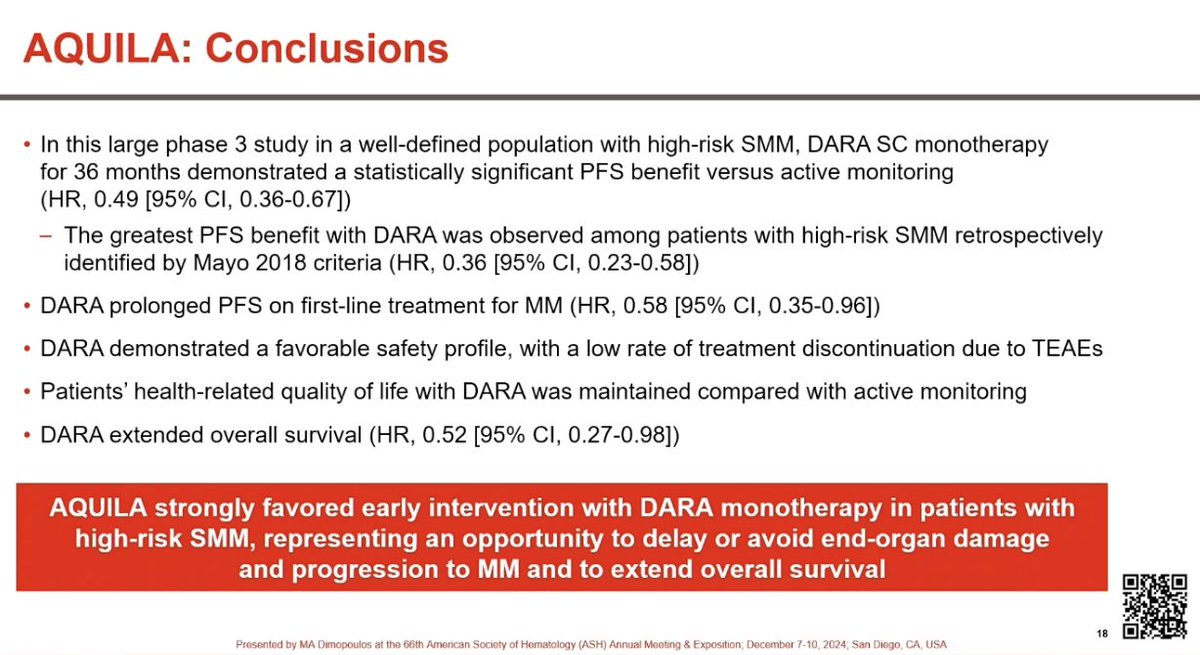
51% reduction in risk of progression to active myeloma or death. Median PFS not reached versus 41.5 months with active monitoring (HR 0.49; 95% CI: 0.36-0.67; p<0.0001). Benefit greatest in highest-risk patients (HR 0.36).
Early OS trend favors daratumumab but data are not mature. The FDA sought ODAC input specifically due to concerns about lack of robust OS data.
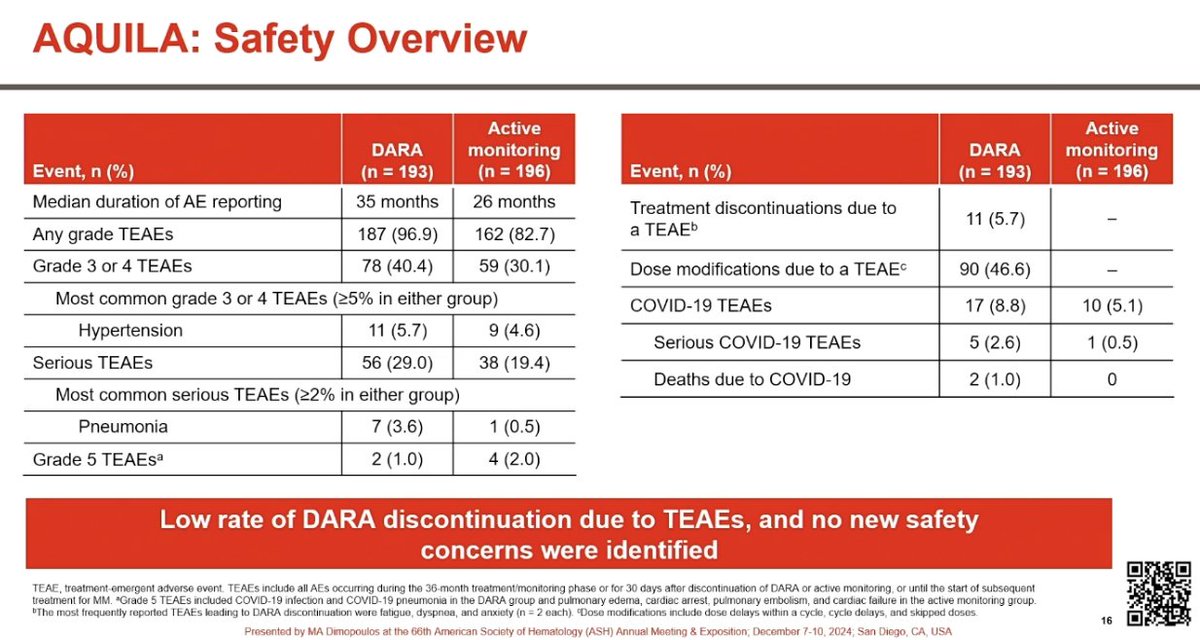
Grade 3+ AEs in 40.4% versus 30.1% with monitoring. Hypertension most common G3+ (5.7%). Pneumonia 3.6% vs 0.5%. Systemic administration reactions in 17%. 6.7% discontinued due to AEs.
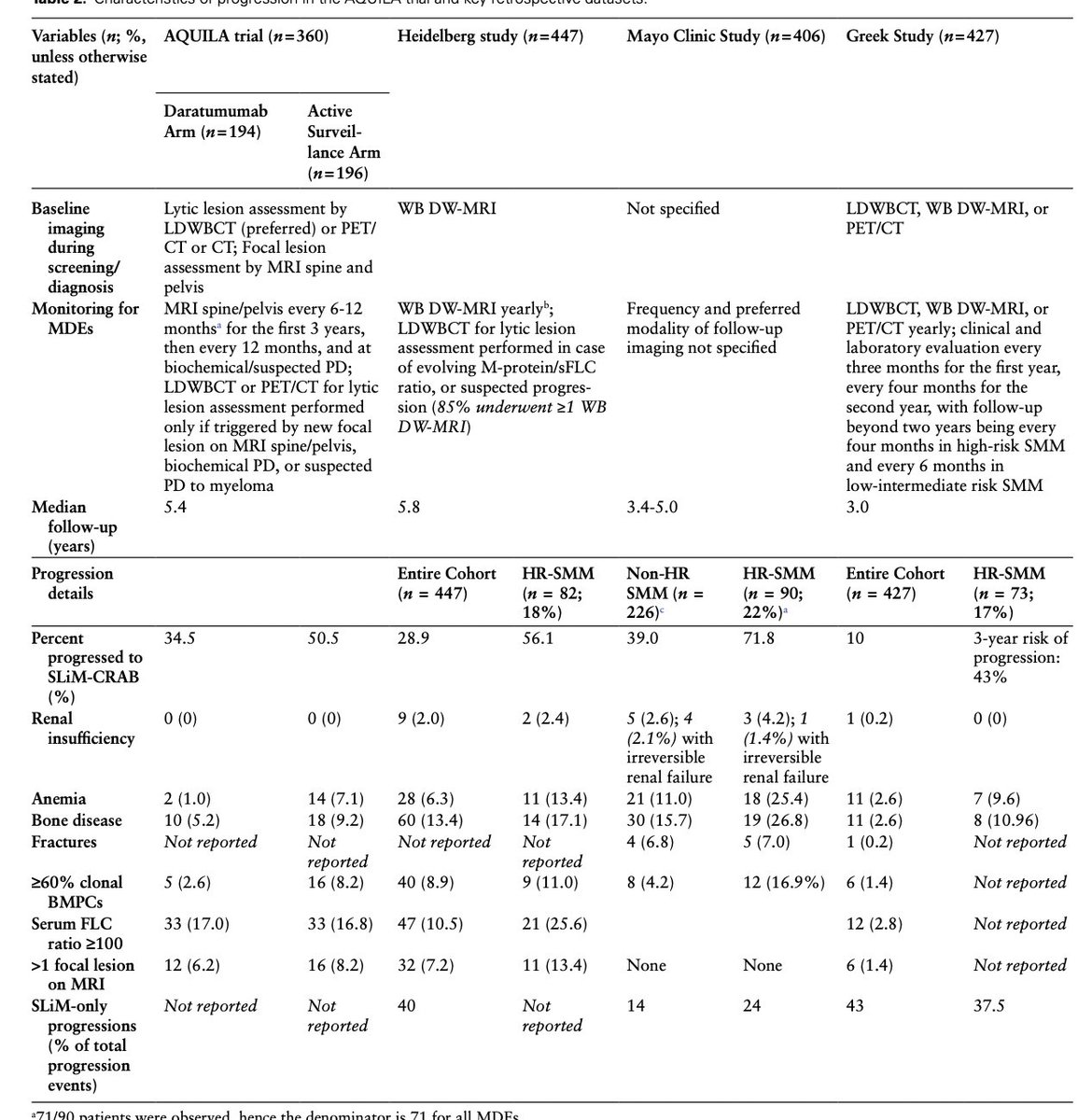
FDA approved November 6, 2025 - first treatment for smoldering myeloma. However, ODAC voted 6-2, reflecting field division. Control group median time to progression was 41.5 months - raising overtreatment concerns. Experts emphasize shared decision-making: not every high-risk SMM patient needs immediate treatment.