1L PD-L1+ NSCLC - Summit/Akeso
Discover KOL Sentiment on HARMONi-2 →Design — Phase 3 (China); ivonescimab (PD-1/VEGF bispecific) monotherapy vs pembrolizumab, 1L PD-L1+ advanced NSCLC (NCT05499390). (WCLC 2024 / JTO)
PFS (primary) — Median PFS 11.14 vs 5.82 mo, stratified HR 0.51 (95% CI 0.38-0.69; p<0.0001) — 49% risk reduction. (WCLC 2024, page data)
OS — Immature; interim HR ~0.78 favoring ivonescimab, not yet significant. (page data)
Safety — Grade ≥3 treatment-related AEs 29% vs 16%; most common Grade ≥3 event hypertension (5%). (page data)
Regulatory — US: NOT FDA approved (investigational). Approved in China (2024/2025) for 1L PD-L1+ NSCLC. (Summit/Akeso)
Sponsor / Drug — Summit Therapeutics / Akeso; ivonescimab, a first-in-class PD-1/VEGF bispecific antibody. (Summit)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 20, 2026.





















Top 10 by impressions - click to view on X
Akeso wins Chinese approval for PD-1/VEGF drug positioned to rival Merck’s $MRK Keytruda Ivonescimab lung cancer approval based on Harmoni-2 study. Also new interim OS data HR=0.784 not yet stat...
Good oncologists don't give single agent pembro to pdl1 1-49 And really good oncologists don't give single agent pembro to pdl1 <90 Bizarre trial....
💥 The end of Pembro reign? Phase 3 Study of Ivonescimab (AK112) vs. Pembrolizumab as First-line Treatment for PD-L1-positive Advanced NSCLC: HARMONi-2 #WCLC24 #LCSM
Going to channel my inner @JackWestMD here and remind everyone it’s China only data, not SOC comparator in US and no OS yet before everyone goes overboard on ivonescimab...
The #WCLC24 late-breaker you've all been waiting for: Akeso's Harmoni-2 trial of $SMMT ivonescimab in 1L PD-L1 ≥1% NSCLC, vs $MRK...
#WCLC24 abstract titles released! Don't miss the plenary Sunday September 8th at 8:30am PDT - I am particularly eager to see the ivonescimab vs pembro HARMONi-2...

Ivonescimab vs Pembrolizumab. For First line NSCLC. Harmoni-2 trial. Remember PFS is already declared postive as clinically meaningful. In both Squamous and Non Squamous histology and in both...

🚨🔥@OncoAlert Hot off the press Just published @TheLancet Results of #HARMONi2 phase 3 trial of #Ivonescimab (#PD1 &...
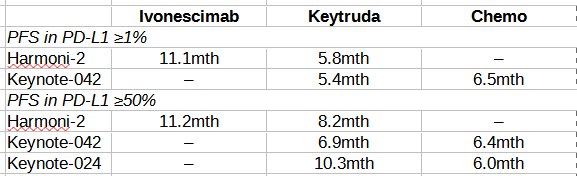
$SMMT Akeso ivonescimab looks pretty convincing in Harmoni-2, but did Keytruda perform in line with KN-042 & KN-024? I've done a handy comparison...

Ivonescimab Monotherapy Decisively Beats Pembrolizumab Monotherapy Head-to-Head, Achieves Statistically Significant Superiority in PFS in First-Line Treatment of Patients with PD-L1 Positive NSCLC in...
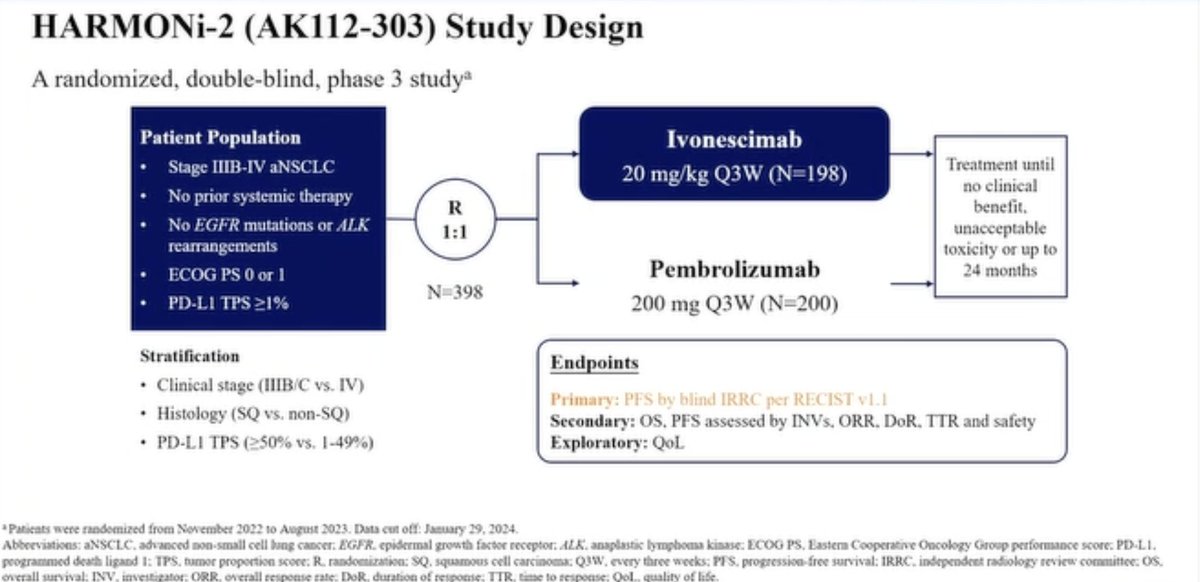
HARMONi-2 is a Phase III, multicenter, double-blind trial that compared ivonescimab monotherapy versus pembrolizumab monotherapy as first-line treatment for patients with PD-L1-positive (TPS >=1%) locally advanced or metastatic NSCLC. The trial randomized 398 patients across 55 centers in China between November 2022 and August 2023. Ivonescimab is a first-in-class bispecific antibody that simultaneously blocks PD-1 and VEGF-A within a single molecule, leveraging cooperative binding and a unique 'daisy chaining' mechanism. At the preplanned interim analysis, ivonescimab demonstrated a statistically significant and clinically meaningful PFS improvement over the established standard-of-care pembrolizumab.
Phase III, multicenter, double-blind, 1:1 randomized trial in 398 patients with untreated locally advanced or metastatic PD-L1-positive (TPS >=1%) NSCLC, negative for EGFR mutations and ALK rearrangements, ECOG PS 0-1. Stratified by PD-L1 expression level (TPS 1-49% vs >=50%) and histology (squamous vs non-squamous). Crossover was not allowed.
Adults with previously untreated locally advanced or metastatic NSCLC, PD-L1 TPS >=1%, ECOG PS 0-1, without EGFR mutations or ALK rearrangements. Approximately 58% had PD-L1 TPS 1-49% and 42% had TPS >=50%. Both squamous and non-squamous histologies were included.
Ivonescimab 20 mg/kg IV every 3 weeks (n=198) versus pembrolizumab 200 mg IV every 3 weeks (n=200) until disease progression or unacceptable toxicity.
Primary endpoint: progression-free survival (PFS) assessed by masked independent radiographic review committee (IRRC). Key secondary endpoints: overall survival (OS), objective response rate (ORR), duration of response, and safety.
At a median follow-up of 8.67 months, median PFS was 11.14 months with ivonescimab versus 5.82 months with pembrolizumab (stratified HR 0.51; 95% CI: 0.38-0.69; p<0.0001), representing a 49% reduction in the risk of disease progression or death. The 9-month PFS rates were 56% with ivonescimab and 40% with pembrolizumab. The PFS benefit was consistent across subgroups: PD-L1 TPS 1-49% (HR 0.54; 95% CI: 0.37-0.78; median PFS 8.0 vs 5.4 months), PD-L1 TPS >=50% (HR 0.48; 95% CI: 0.29-0.79; median PFS 11.1 vs 8.2 months), and across both squamous and non-squamous histologies.
Overall survival data remain immature. A preliminary interim OS analysis showed a hazard ratio of 0.777 favoring ivonescimab, suggesting a 22.3% numerical reduction in the risk of death, but statistical significance has not been reached at this data maturity level. The second and final OS analyses will be critical to confirm this trend. The HARMONi-7 global trial (ivonescimab vs pembrolizumab in high PD-L1 NSCLC) is powered for both OS and PFS co-primary endpoints to address this question in a multiregional population.
Ivonescimab demonstrated a manageable safety profile with no new safety signals. Grade >=3 treatment-related adverse events occurred in 29% of ivonescimab patients versus 16% with pembrolizumab. The most common grade >=3 TRAE with ivonescimab was hypertension (5%). Serious TRAEs were reported in 21% versus 16%. Grade >=3 immune-related AEs were similar between arms (7% vs 8%). Common AEs related to VEGF blockade included proteinuria and hypertension, generally low-grade. In patients with squamous cell carcinoma, grade >=3 TRAEs were comparable between groups.
HARMONi-2 established ivonescimab as the first therapy to demonstrate a significant PFS benefit over pembrolizumab in a head-to-head Phase III study. Ivonescimab monotherapy was approved in China in April 2025 for first-line PD-L1-positive advanced NSCLC based on these results. However, the trial was conducted exclusively in China, raising questions about generalizability to global populations. Key unresolved questions include: (1) whether the PFS benefit will translate to a definitive OS advantage, (2) whether results will replicate in the ongoing multiregional HARMONi-7 trial, and (3) whether the unique cooperative binding and daisy chaining mechanism of ivonescimab differentiates it from other PD-1/VEGF bispecifics entering the pipeline. Ivonescimab remains investigational in the US and Europe.
HARMONi-2 is a Phase 3 head-to-head trial (conducted in China) of ivonescimab, a PD-1/VEGF bispecific antibody, versus pembrolizumab monotherapy as first-line treatment of PD-L1-positive advanced non-small cell lung cancer (NCT05499390).
No. Ivonescimab is not FDA approved in the United States; it is investigational there. Ivonescimab is approved in China for first-line PD-L1-positive advanced NSCLC. US registrational trials are ongoing.
Ivonescimab monotherapy significantly improved progression-free survival versus pembrolizumab: median PFS was 11.14 versus 5.82 months (stratified HR 0.51; 95% CI 0.38-0.69; p<0.0001), a 49% reduction in the risk of progression or death. It was the first therapy to beat pembrolizumab on PFS in a head-to-head Phase 3 study. Overall survival data remain immature.
In HARMONi-2, Grade ≥3 treatment-related adverse events occurred in 29% of ivonescimab patients versus 16% with pembrolizumab, with hypertension the most common Grade ≥3 event (5%). As a VEGF-targeting agent, ivonescimab has VEGF-class effects such as hypertension.
Ivonescimab is developed by Akeso and, outside China, by Summit Therapeutics.



















































