MARIPOSA is a Phase 3 trial of amivantamab (Rybrevant) plus lazertinib (Lazcluze) versus osimertinib in first-line EGFR exon 19 deletion or L858R advanced NSCLC. The combination improved median PFS to 23.7 vs 16.6 months (HR 0.70; p=0.0002) and later showed an overall survival benefit, supporting FDA approval on August 19, 2024. Sponsor: Janssen (Johnson & Johnson).
Discover KOL Sentiment on MARIPOSA →Design — Phase 3, open-label; amivantamab (Rybrevant) + lazertinib (Lazcluze) vs osimertinib, 1L EGFR ex19del/L858R advanced NSCLC, n=1,074 (NCT04487080). (NEJM)
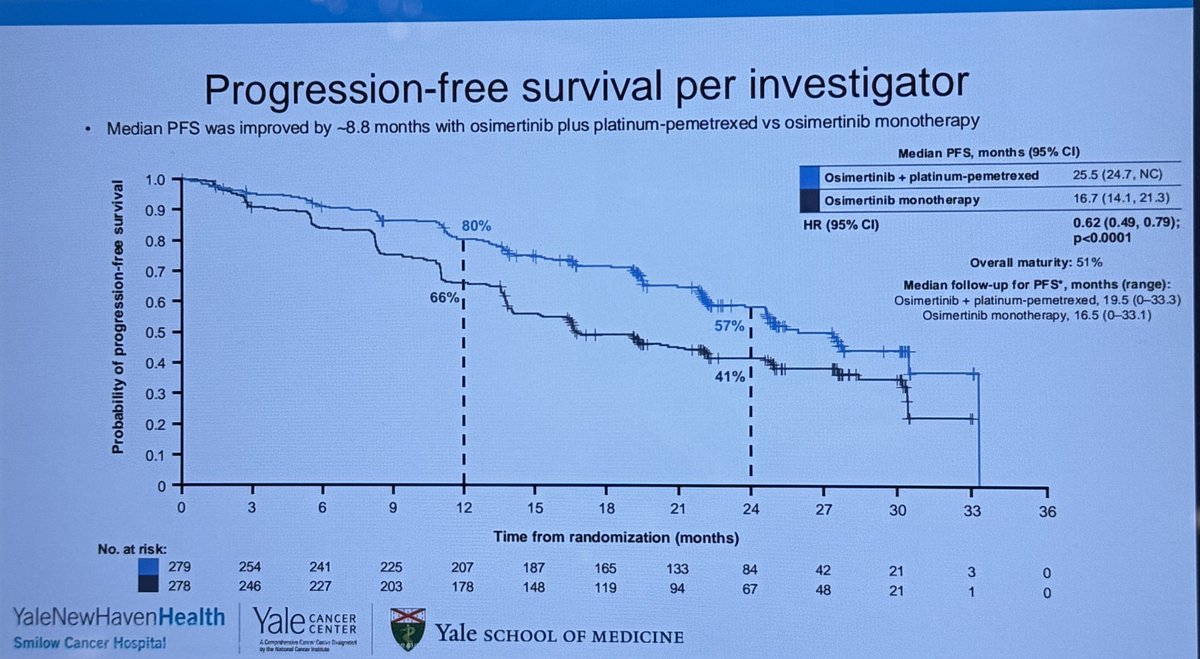
PFS (primary) — Median 23.7 vs 16.6 months; HR 0.70 (95% CI 0.58-0.85; p=0.0002). (NEJM, DCO1)
Overall survival — Statistically significant OS benefit at 42-mo follow-up; HR 0.75, >1 year median OS improvement. (ELCC 2025 update)
Safety — Higher AE burden than osimertinib; notable venous thromboembolism (VTE) signal requiring prophylactic anticoagulation for the first 4 months; EGFR/MET skin & nail toxicity. (NEJM)
Regulatory — FDA approved August 19, 2024 for 1L EGFR ex19del/L858R advanced NSCLC. (FDA.gov)
Sponsor / Drug — Janssen (Johnson & Johnson); amivantamab (EGFR-MET bispecific) + lazertinib (3rd-gen EGFR TKI). (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.
















Top 10 by impressions - click to view on X

Report on time to symptomatic progression from phase III MARIPOSA study in EGFR mutant NSCLC available. Median was 43.6m with 1L amivantamab + lazertinib compared to 29.3m with osimertinib (HR 0.69). TTSP strongly correlated with PFS and OS.
‼️#MARIPOSA study update: Combination therapy shows over ONE-YEAR mOS improvement compared to osimertinib alone. Key data to discuss with patients in clinic—but does this simplify...
MET IHC is a strong predictive factor for the efficacy of amivantamab + lazertinib in pts with EGFRmut NSCLC, independently of the resistance mechanism to osimertinib. PFS 12.2/4.2mo in MET+/-. Might...
‼️Breaking news—the OVERALL SURVIVAL results from #MARIPOSA are out at #ELCC25. Does this update change practice for all patients with treatment-naïve EGFR+...

#MARIPOSA🦋 @JNJNews announces Positive OS results in 1L EGFR #lcsm 🎯 Amivantamab + lazertinib vs. osimertinib: ✅ Statistically significant improvement in...

Original Article: Amivantamab Plus Lazertinib in Previously Untreated EGFR-Mutated Advanced NSCLC (MARIPOSA phase 3 trial) #LungCancer

💥 Just @NEJM published OS data from MARIOOSA vs presented FLAURA-2 data at @IASLC #WCLC25 Survival of intensification strategy in 1L EGFR lung cancer. Both works,...

Why would anyone take these toxic shit medicines over the well tolerated Osi for just a PFS benefit. Also if you want PFS just do chemo OSI. It's way cheaper.

Osimertinib BEATEN!! MARIPOSA (Ami + Lazer) shows significant OS (HR 0.75, p<0.005, 3yr 60% vs 51%) and landmark 3-yr icPFS improvement (36% vs 18%)—first combo to show OS superiority over...
✨MARIPOSA: Amivantamab + lazertinib v osimertinib in 1L EGFR+ mNSCLC: Biomarkers of high-risk dz? ▫️TP53 co-mutation ▫️+ctDNA ▫️Liver mets A path forward to identify biomarkers to help us determine...
🚨🔥@OncoAlert Hot off the press. Just published @NEJM Results of #MARIPOSA Study of: #Amivantamab plus #Lazertinib vs...
MARIPOSA is a phase 3, randomized, open-label trial (NCT04487080) evaluating amivantamab plus lazertinib versus osimertinib as first-line therapy in patients with EGFR-mutant advanced non-small cell lung cancer (NSCLC). The trial enrolled 1,074 patients with locally advanced or metastatic NSCLC harboring EGFR exon 19 deletions or exon 21 L858R substitution mutations. Results demonstrated a statistically significant improvement in both PFS and OS with the combination, leading to FDA approval in August 2024.
Phase 3, randomized (2:2:1), open-label, active-controlled, multicenter trial comparing amivantamab (EGFR-MET bispecific antibody) plus lazertinib (third-generation EGFR TKI) versus osimertinib monotherapy in treatment-naive EGFR-mutant advanced NSCLC.
Adults with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations, as detected by an FDA-approved test. No prior systemic therapy for advanced disease.
Amivantamab-vmjw (Rybrevant) intravenous plus lazertinib (Lazcluze) oral daily versus osimertinib monotherapy. A third arm evaluated lazertinib monotherapy.
Primary endpoint: progression-free survival (PFS) assessed by blinded independent central review. Key secondary endpoints included overall survival (OS), overall response rate (ORR), duration of response (DOR), and intracranial PFS.
The combination of amivantamab plus lazertinib demonstrated a statistically significant improvement in PFS versus osimertinib (HR 0.70; 95% CI: 0.58-0.85; p=0.0002). Median PFS was 23.7 months (95% CI: 19.1-27.7) with the combination versus 16.6 months (95% CI: 14.8-18.5) with osimertinib. ORR was 86% with the combination versus 85% with osimertinib.
Updated OS data presented at ELCC 2025 showed a statistically significant OS improvement with amivantamab plus lazertinib versus osimertinib. At 42 months of follow-up, the OS HR was 0.75, with more than one year of median OS improvement. Three-year OS rates were 60% with the combination versus 51% with osimertinib.
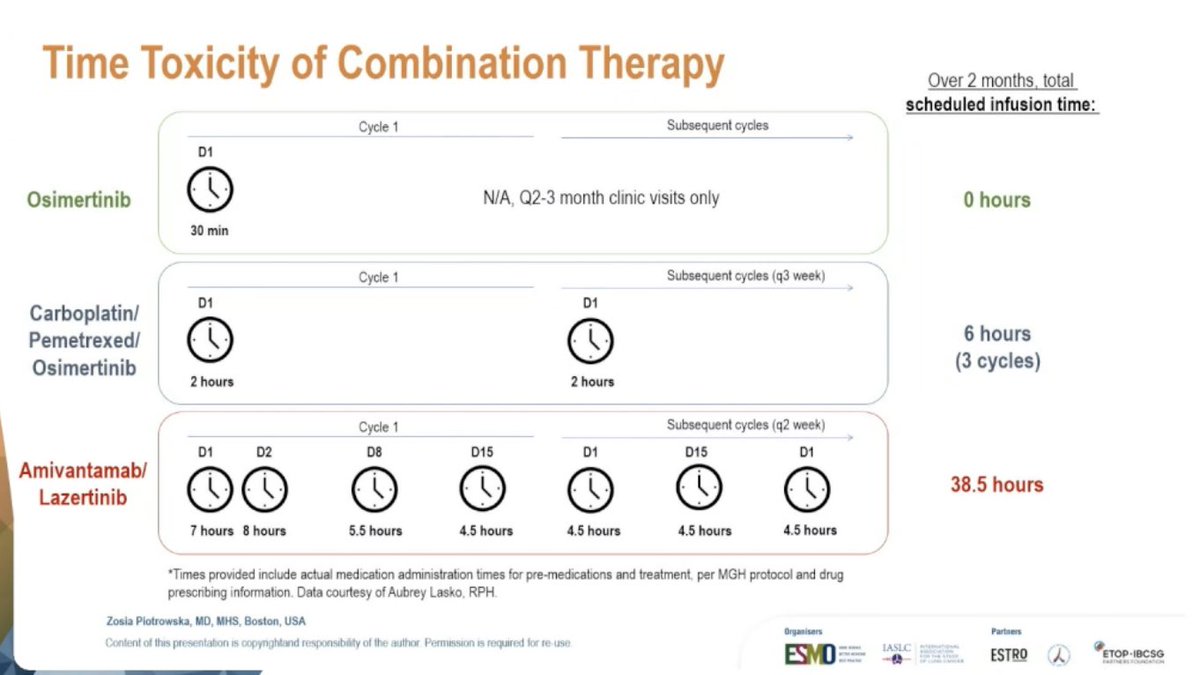
The combination was associated with higher rates of adverse events compared to osimertinib monotherapy. A notable safety signal of venous thromboembolic events (VTE) was observed, requiring prophylactic anticoagulation for the first four months of therapy. Infusion-related reactions and skin toxicity were also more common with the combination. Time toxicity — the burden of treatment-related clinic visits and infusions — has been raised as a practical consideration by treating physicians.
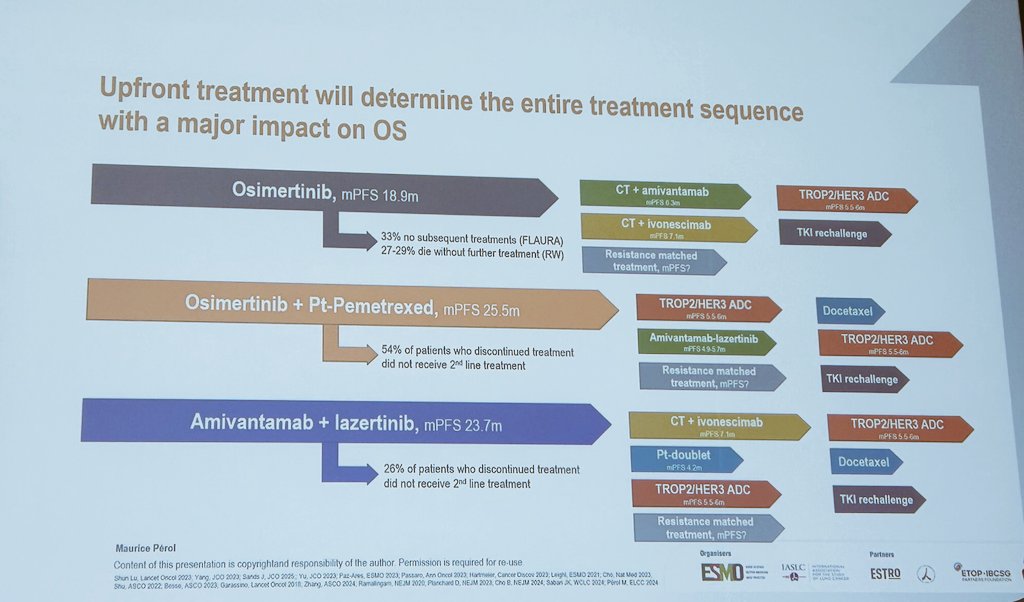
MARIPOSA establishes amivantamab plus lazertinib as a new first-line standard for EGFR-mutant advanced NSCLC. The combination received FDA approval in August 2024 for patients with EGFR exon 19 deletions or L858R mutations. However, the increased toxicity and time burden compared to osimertinib monotherapy remain active topics of clinical debate, with some physicians reserving the combination for specific patient subgroups such as those with MET-positive tumors.
MARIPOSA is a Phase 3, randomized, open-label trial (NCT04487080) evaluating amivantamab (Rybrevant) plus lazertinib (Lazcluze) versus osimertinib as first-line therapy in 1,074 patients with locally advanced or metastatic NSCLC harboring EGFR exon 19 deletions or exon 21 L858R mutations.
Yes. On August 19, 2024 the FDA approved lazertinib (Lazcluze) in combination with amivantamab-vmjw (Rybrevant) for the first-line treatment of locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations, as detected by an FDA-approved test.
The combination of amivantamab plus lazertinib improved median progression-free survival to 23.7 months versus 16.6 months with osimertinib (HR 0.70; 95% CI 0.58-0.85; p=0.0002), a statistically significant improvement.
Yes. Updated data presented at ELCC 2025 (42-month follow-up) showed a statistically significant overall survival improvement with amivantamab plus lazertinib versus osimertinib (HR 0.75), with more than one year of median OS improvement.
The combination has a higher adverse-event burden than osimertinib monotherapy, including EGFR- and MET-related skin and nail toxicity and a notable venous thromboembolic event (VTE) signal that requires prophylactic anticoagulation during the first four months of therapy.




















