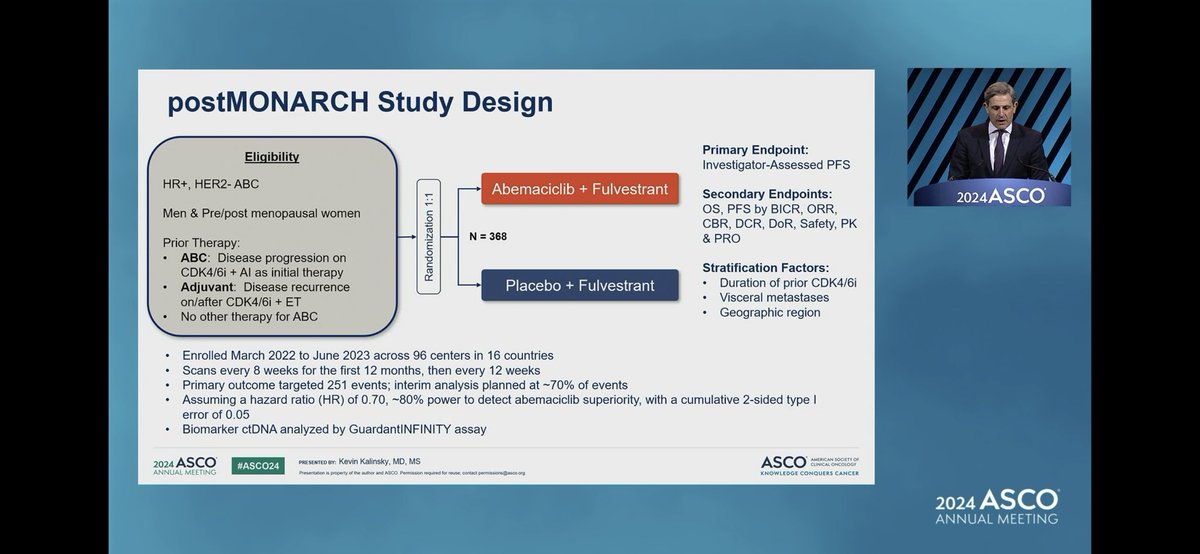
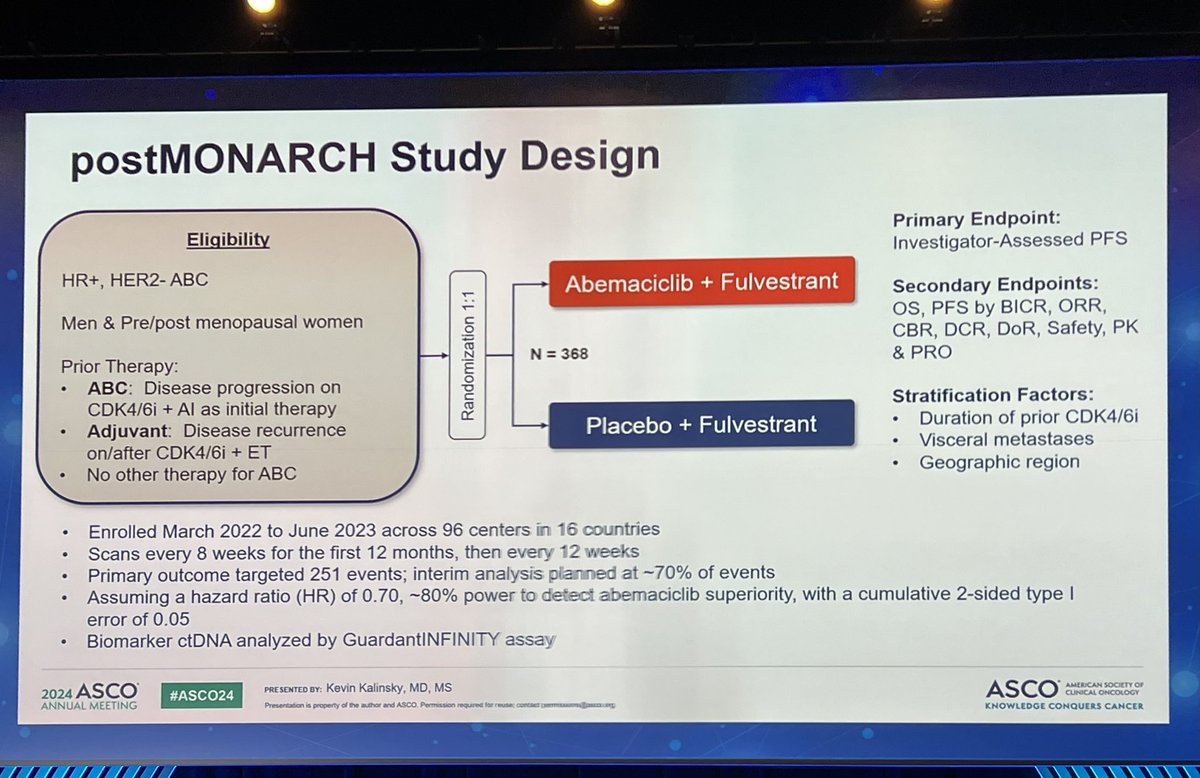
Design - Phase 3 abemaciclib + fulvestrant vs placebo + fulvestrant after prior CDK4/6-inhibitor progression, HR+/HER2- mBC (NCT05169567).
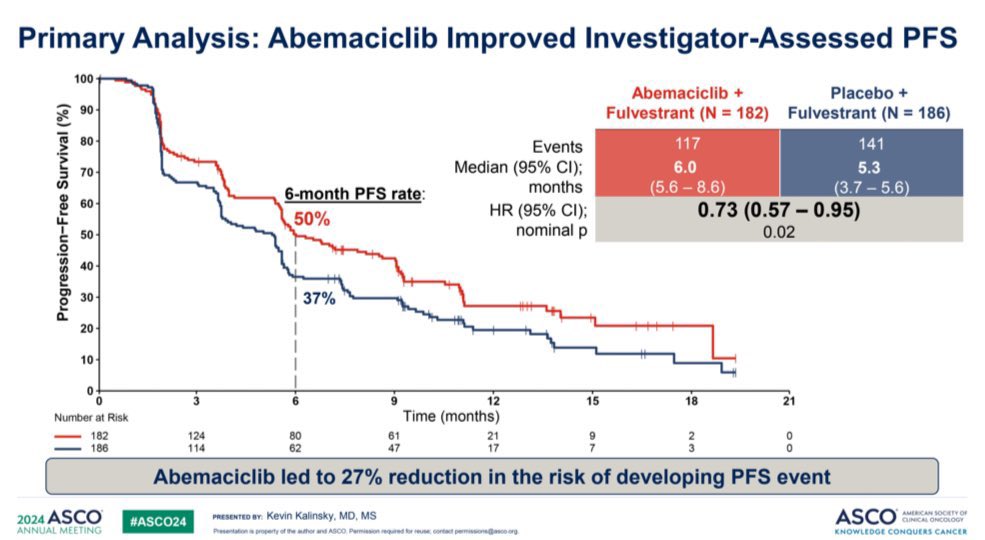
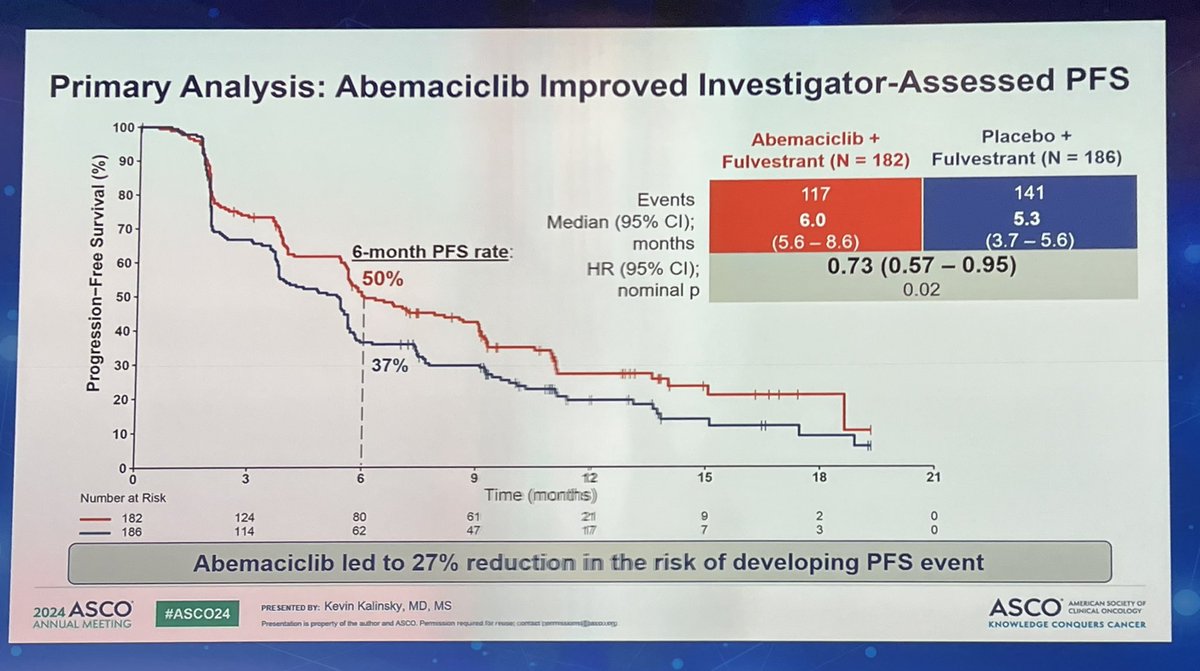
PFS (primary) - MET - investigator-assessed median 6.0 vs 5.3 mo, HR 0.73 (95% CI 0.57-0.95), P=0.02; BICR-assessed 12.9 vs 5.6 mo, HR 0.55 (P=0.0004).
OS - Immature at the primary analysis - no overall survival results reported.
Safety - Consistent with known abemaciclib toxicity - Grade 3+ neutropenia 25%, anemia 11%; AE discontinuation 6% vs 0%; one Grade 5 event (pneumonia).
Regulatory - Investigational in the post-CDK4/6i setting; abemaciclib is FDA approved in other HR+/HER2- breast cancer settings.
[Slide 1]
postMONARCH Study Design
Primary Endpoint:
Eligibility
Investigator-Assessed PFS
HR+, HER2-ABC
Abemaciclib + Fulvestrant
Secondary Endpoints:
Men & Pre/post menopausal women
OS, PFS by BICR, ORR,
CBR, DCR, DoR, Safety, PK
N = 368
Prior Therapy:
& PRO
ABC: Disease progression on
Stratification Factors:
CDK4/6i + Al as initial therapy
Adjuvant: Disease recurrence
Placebo + Fulvestrant
Duration of prior CDK4/6i
Visceral metastases
on/after CDK4/6i + ET
No other therapy for ABC
Geographic region
Enrolled March 2022 to June 2023 across 96 centers in 16 countries
Scans every 8 weeks for the first 12 months, then every 12 weeks
Primary outcome targeted 251 events; interim analysis planned at ~70% of events
Assuming a hazard ratio (HR) of 0.70, ~80% power to detect abemaciclib superiority, with a cumulative 2-sided type I
error of 0.05
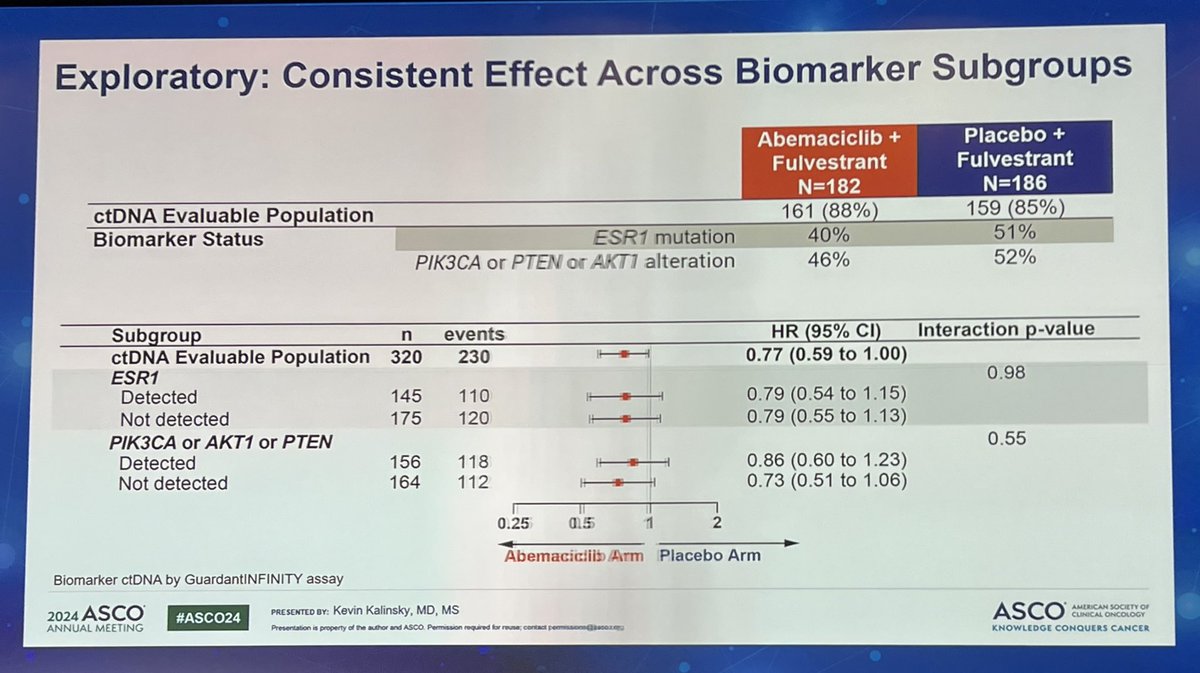
Biomarker ctDNA analyzed by GuardantINFINITY assay
2024
ASCO
PRESENTED BY: Kevin Kalinsky, MD, MS
ASCO
AMERICAN SOCIETY OF
#ASCO24
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission
KNOWLEDGE CONQUERS CANCER
[Slide 1]
X
15:00 GMT-5
Abemaciclib plus fulvestrant vs
C
fulvestrant alone for HR+, HER2-
advanced breast cancer following
progression on a prior CDK4/6
inhibitor plus endocrine therapy:
Primary outcome of the phase 3
1
postMONARCH trial.
Presenter: Kevin Kalinsky, MD, MS
I
Winship Cancer Institute of Emory
University
Abstract: LBA1001
---
[Slide 2]
Se
Presenter: Rebecca Arielle Shatsky, MD
Abstract: LBA501
P
15:24 GMT-5
A randomized, multicenter, open-
label, phase III trial comparing
anthracyclines followed by taxane
versus anthracyclines followed by
taxane plus carboplatin as (neo)
adjuvant therapy in patients with
C
early triple-negative breast
cancer: Korean Cancer Study
Group BR 15-1 PEARLY trial.
Presenter: Joohyuk Sohn, MD, PhD
I
Division of Medical Oncology, Department
O
of Internal Medicine, Yonsei University
College of Medicine
B
Abstract: LBA502
---
[Slide 3]
16:00 GMT-5
SACI-IO HR+: A randomized
phase II trial of sacituzumab
govitecan with or without
1
pembrolizumab in patients with
metastatic hormone receptor-
positive/HER2-negative breast
cancer.
O
Presenter: Ana Christina Garrido-Castro,
MD I Dana-Farber Cancer Institute
B
Abstract: LBA1004
P
16:12 GMT-5
Enfortumab vedotin (EV) in triple-
negative breast cancer (TNBC)
and HR+/HER2- breast cancer
(BC) cohorts of EV-202.
Presenter: Antonio Giordano, MD, PhD
I
C
Dana-Farber Cancer Institute
Abstract: 1005
...
---
[Slide 4]
Fi
3
X
Se
Presentations
15:00 GMT-5
P
A-BRAVE trial: A phase III
randomized trial with avelumab in
early triple-negative breast
cancer with residual disease after
neoadjuvant chemotherapy or at
high risk after primary surgery
and adjuvant chemotherapy.
C
Presenter: Pier Franco Conte, MD
|
Department of Surgery Oncology and
Gastroenterology, University of Padua
Abstract: LBA500
o
15:12 GMT-5
B
Rates of pathologic complete
L
response (pCR) after
datopotamab deruxtecan (Dato)
P
plus durvalumab (Durva) in the
neoadjuvant setting: Results from
the I-SPY2.2 trial.
Presenter: Rebecca Arielle Shatsky, MD
Abstract: LBA501
[Slide 1]
LOXO@Lilly
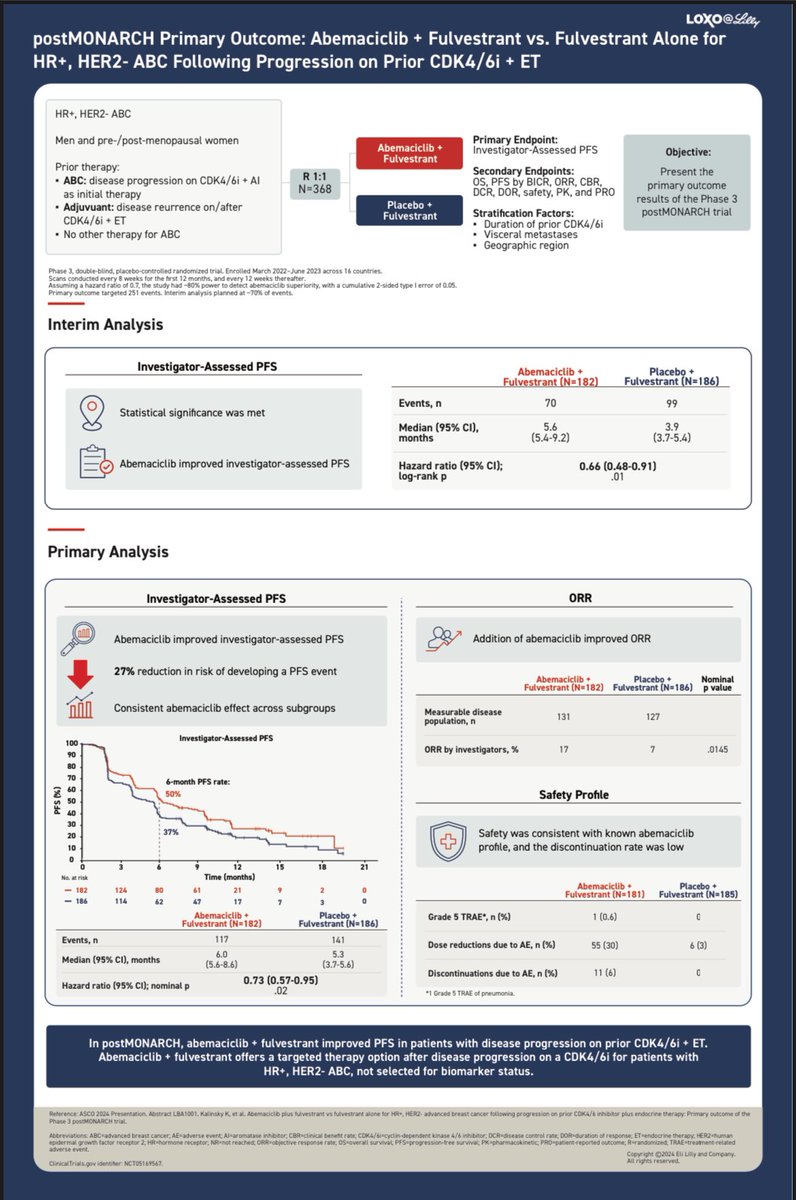
postMONARCH Primary Outcome: Abemaciclib + Fulvestrant vs. Fulvestrant Alone for
HR+, HER2- ABC Following Progression on Prior CDK4/6i + ET
HR+, HER2-ABC
Men and pre-/post-menopausal women
Primary Endpoint:
Abemaciclib
Investigator-Assessed PFS
Objective:
Fulvestrant
Prior therapy:
ABC: disease progression on CDK4/61 AI
R 1:1
Secondary Endpoints:
Present the
OS, PFS by BICR, ORR CBR.
N=368
primary outcome
as initial therapy
DCR DOR, safety, PK, and PRO
results of the Phase 3
Adjuvuant: disease reurrence on/after
Placebo +
CDK4/6 ET
Fulvestrant
Stratification Factors:
postMONARCH trial
Duration of prior CDK4/6
No other therapy for ABC
Visceral metastases
Geographic region
Phase 3. double randomized trial Enrolled March 2022-June 2023 across 14 countries
for
the
test
12
months
and
12
thereafter
the study had -80% power superiority with cumulative -sided type error of 0.05
Primary outcome targeted 25 events Interim planned of events
Interim Analysis
Investigator-Assessed PFS
Abemaciclib +
Placebo +
Fulvestrant (N=182)
Fulvestrant (N=186)
Events, n
70
99
Statistical significance was met
Median (95% CI),
5.6
3.9
months
(5.4-9.2)
(3.7-5.4)
Abemaciclib improved investigator-assessed PFS
Hazard ratio (95% CI);
0.66 (0.48-0.91)
log-rank p
.01
Primary Analysis
Investigator-Assessed PFS
ORR
Abemaciclib improved investigator-assessed PFS
Addition of abemaciclib improved ORR
27% reduction in risk of developing a PFS event
Abemaciclib +
Placebo
Nominal
Fulvestrant (N=182)
Fulvestrant (N=186)
P value
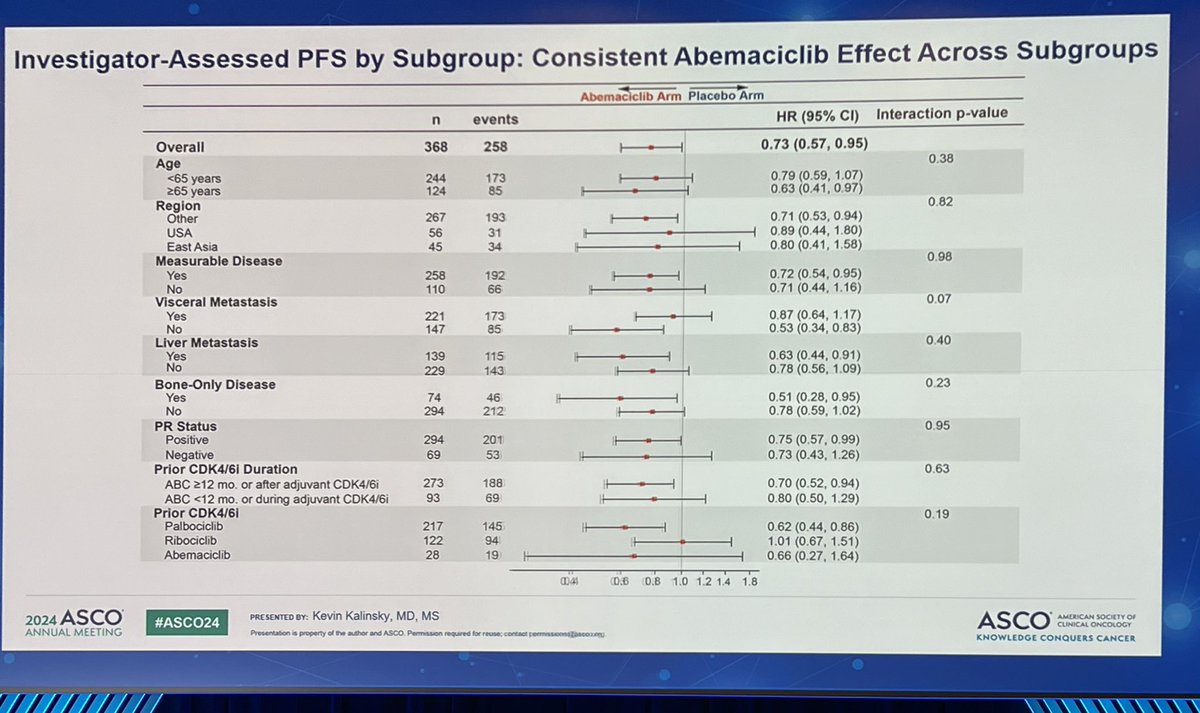
Consistent abemaciclib effect across subgroups
Measurable disease
131
127
population, n
100
Investigator-Assessed PFS
ORR by investigators, %
17
7
.0145
90
80
70
6-month PFS rate:
60
50%
50
Safety Profile
40
30
20
37%
Safety was consistent with known abemaciclib
10
profile, and the discontinuation rate was low
D
0
3
9
12
15
18
21
Time (months)
182
124
80
61
21
9
2
0
Abemaciclib
Placebo
Fulvestrant (N=181)
Fulvestrant N=185)
186
114
62
47
17
7
3
D
Abemaciclib
Placebo +
Grade 5 TRAE*, (%)
1 (0.6)
0
Fulvestrant (N=182)
Fulvestrant (N=186)
Events, n
117
141
Dose reductions due to AE, n (%)
55 (30)
6 (3)
6.0
5.3
Median (95% CI), months
(5.6-8.6)
(3.7-5.6)
Discontinuations due to AE, n (%)
11 (6)
0
Hazard ratio (95% CI); nominal P
0.73 (0.57-0.95)
.02
* Grade TRAE pneumonia
In postMONARCH, abemaciclib + fulvestrant improved PFS in patients with disease progression on prior CDK4/6i + ET.
Abemaciclib - fulvestrant offers a targeted therapy option after disease progression on a CDK4/61 for patients with
HR+, HER2- ABC, not selected for biomarker status.
Reference ASCO 2024 Presentation Abstract LBA1001 Kalinsky K et al Abemaciclib Minestrant vi Minestrant alone for HR HER2 advanced breast cancer following progression on prior COKA/A inhibitor plus endocrine therapy Primary outcome of the
DOSEMONARCH trial
Abbreviations Cradvanced breast cancer. AE -adverse event inhibitor CBR-clinical behaff rate dependent DCR-disease control rate DOR-duration of response ETrendocrine therapy. ER2+human
growth factor reception HRxharmone reception ARKNO reached OS-overal survival Rerandomized TRAP
event
Copyright C2024 EL Lily and Company
[Slide 1]
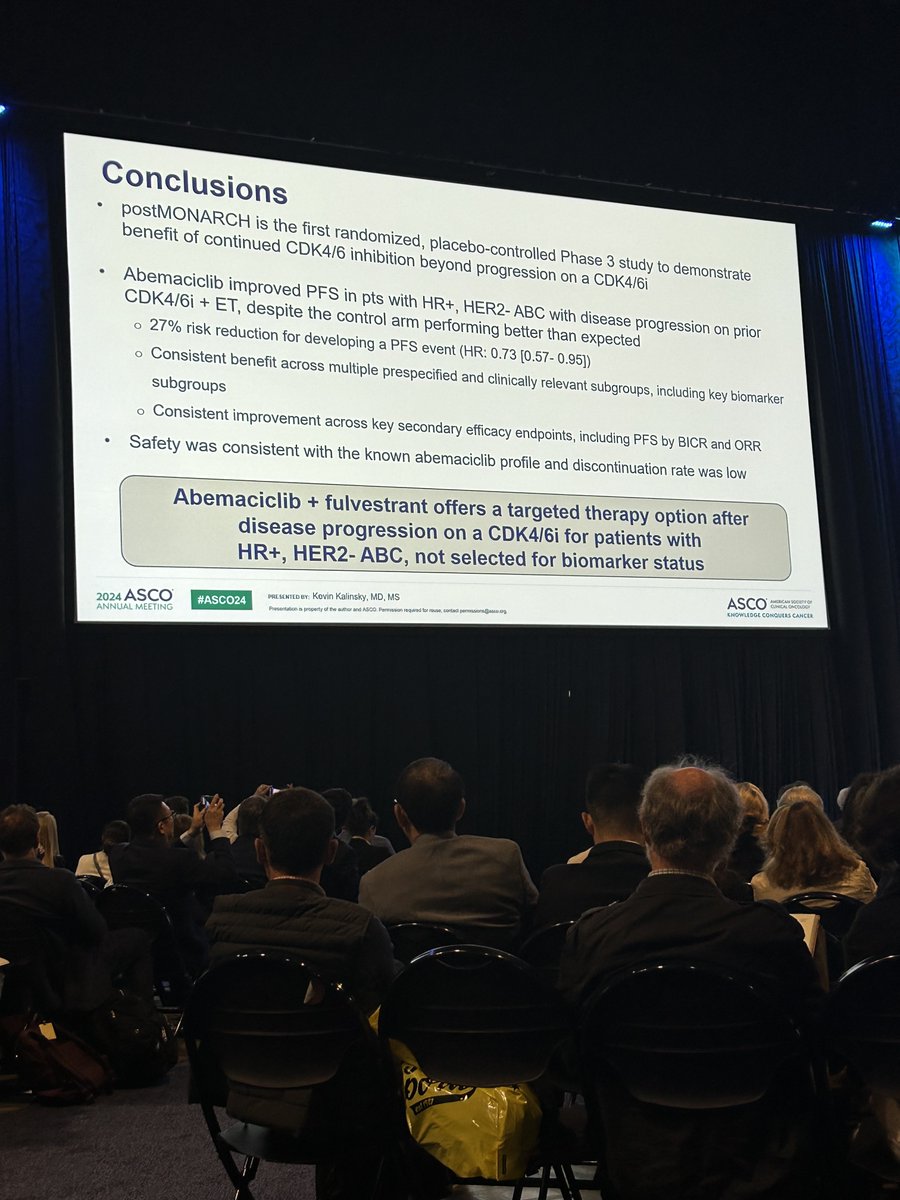
Conclusions
postMONARCH is the first randomized, placebo-controlled Phase 3 study to demonstrate
benefit of continued CDK4/6 inhibition beyond progression on a CDK4/6i
Abemaciclib improved PFS in pts with HR+, HER2- ABC with disease progression on prior
CDK4/6i + ET, despite the control arm performing better than expected
27% risk reduction for developing a PFS event (HR: 0.73 [0.57-0.95])
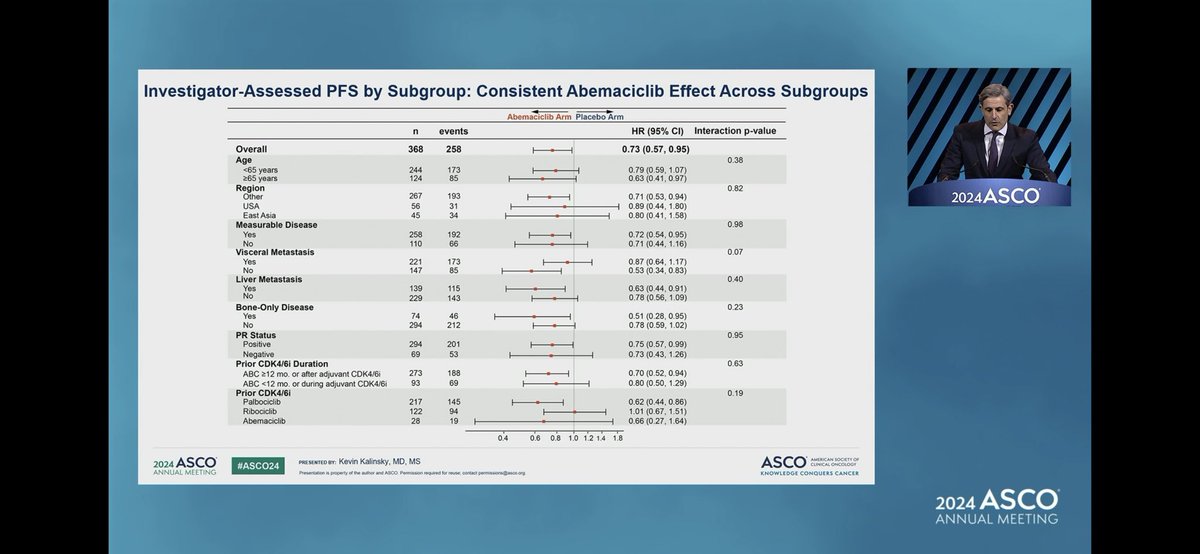
Consistent benefit across multiple prespecified and clinically relevant subgroups, including key biomarker
subgroups
Consistent improvement across key secondary efficacy endpoints, including PFS by BICR and ORR
Safety was consistent with the known abemaciclib profile and discontinuation rate was low
Abemaciclib + fulvestrant offers a targeted therapy option after
disease progression on a CDK4/6i for patients with
HR+, HER2- ABC, not selected for biomarker status
ASCO
AMERICAN
CONCAL ENCOLOGY
PRE SENTED BY: Kevin Kalinsky, MD, MS
KNOWLEDGE CONQUERS CANCER
2024 ASCO
#ASCO24
Presentation property if the altor and ASCO Permission required - - contact
ANNUAL MEETING
[Slide 1]
Oral presentation
#ASCO24
Primary Outcome Results from the Phase 3
postMONARCH study
A CDK 4/6 Inhibitor + Fulvestrant in HR+, HER2-
Advanced Breast Cancer Following Progression
on a Prior CDK 4/6 Inhibitor
Presentation Date and Time:
Room:
Saturday, June 1, 3:00 PM CDT
Hall B1 I Live Stream
LOXO@Lilly
Abstract #LBA1001
postMONARCH is a global, randomized, double-blind, placebo-controlled Phase III trial evaluating abemaciclib (Verzenio) plus fulvestrant versus placebo plus fulvestrant in patients with HR+/HER2- advanced breast cancer who progressed on a prior CDK4/6 inhibitor and endocrine therapy. It is the first Phase III, placebo-controlled study to demonstrate a statistically significant benefit of continued CDK4/6 inhibition beyond progression on a prior CDK4/6 inhibitor, regardless of biomarker status.
Phase III, global, randomized (1:1), double-blind, placebo-controlled trial (NCT05169567). Patients received abemaciclib 150 mg orally twice daily plus fulvestrant 500 mg IM, or placebo plus fulvestrant. Stratified by duration of prior CDK4/6 inhibitor, visceral metastases, and geographic region. Enrolled March 2022 to June 2023 across 96 centers in 16 countries.
Population
Men and pre/postmenopausal women with HR+/HER2- advanced or metastatic breast cancer who experienced disease progression on CDK4/6 inhibitor plus aromatase inhibitor as initial advanced therapy, or disease recurrence on/after adjuvant CDK4/6 inhibitor plus ET. No prior chemotherapy, SERDs, or PI3K/mTOR/AKT inhibitors for advanced disease. ECOG PS 0-1. 368 patients randomized.
Interventions
Abemaciclib 150 mg orally twice daily on Days 1-28 of a 28-day cycle plus fulvestrant 500 mg IM on Days 1 and 15 of Cycle 1, then Day 1 of subsequent cycles, versus matched placebo plus fulvestrant.
Primary Endpoints
Primary endpoint: investigator-assessed PFS. Key secondary endpoints: overall survival (OS), BICR-assessed PFS, ORR, clinical benefit rate (CBR), disease control rate (DCR), duration of response, safety, pharmacokinetics, and patient-reported outcomes.
Progression-Free Survival (PFS)
The primary endpoint was met. At the primary analysis (258 events), median PFS was 6.0 months (95% CI: 5.6-8.6) with abemaciclib versus 5.3 months (95% CI: 3.7-5.6) with placebo (HR 0.73; 95% CI: 0.57-0.95; p=0.02), a 27% risk reduction. The 6-month PFS rate was 50% versus 37%. BICR-assessed PFS showed a larger benefit: 12.9 months versus 5.6 months (HR 0.55; 95% CI: 0.39-0.77; p=0.0004). Benefit was consistent across subgroups, including prior palbociclib (HR 0.62), bone-only disease (HR 0.51), liver metastases (HR 0.63), and prior CDK4/6i duration of 12+ months (HR 0.70).
PFS HR 0.73 — first Phase III post-CDK4/6i benefit
The safety profile was consistent with known abemaciclib toxicity. Grade 3+ AEs in the abemaciclib arm included neutropenia (25%), anemia (11%), leukopenia (8%), AST elevation (6%), diarrhea (4%), thrombocytopenia (4%), ALT elevation (4%), fatigue (3%), and VTE (2%). One grade 5 treatment-related AE (pneumonia) occurred in the abemaciclib arm. AEs led to dose reductions in 30% versus 3% and discontinuation in 6% versus 0%.
postMONARCH establishes abemaciclib plus fulvestrant as a biomarker-unselected treatment option after CDK4/6 inhibitor progression, addressing a critical unmet need. The modest absolute PFS gain (0.7 months by investigator, but 7.3 months by BICR) and the debate around the informative censoring discrepancy between investigator and BICR assessments are key discussion points. The trial supports CDK4/6i rechallenge with a switch strategy (especially from palbociclib to abemaciclib) but raises questions about whether ribociclib-pretreated patients benefit similarly (HR 1.01, wide CI). Clinical debate continues on optimal sequencing versus biomarker-directed therapies (ESR1: oral SERDs; PI3K: alpelisib/inavolisib) and ADCs.
Frequently Asked Questions
postMONARCH FAQ
What is the postMONARCH trial?
postMONARCH is a Phase 3 randomized trial (NCT05169567) of abemaciclib (Verzenio) plus fulvestrant versus placebo plus fulvestrant in patients with HR-positive, HER2-negative metastatic breast cancer whose disease progressed on a prior CDK4/6 inhibitor. Progression-free survival was the primary endpoint.
Did postMONARCH meet its primary endpoint?
Yes. The primary endpoint was met: investigator-assessed median progression-free survival was 6.0 versus 5.3 months (HR 0.73; 95% CI 0.57-0.95; P=0.02), a 27% risk reduction, and blinded independent central review (BICR) showed a larger benefit of 12.9 versus 5.6 months (HR 0.55; P=0.0004). Overall survival data were immature at the primary analysis.
Is abemaciclib plus fulvestrant FDA approved for use after CDK4/6 inhibitor progression?
The specific post-CDK4/6-inhibitor continuation setting studied in postMONARCH is investigational and not a separate FDA-approved indication. Abemaciclib (Verzenio) is FDA approved in other HR-positive, HER2-negative breast cancer settings - with an aromatase inhibitor or fulvestrant in advanced disease, and as adjuvant therapy for high-risk early breast cancer.
What is the safety profile in postMONARCH?
The safety profile was consistent with known abemaciclib toxicity. Grade 3 or higher adverse events in the abemaciclib arm included neutropenia (25%), anemia (11%), leukopenia (8%), and diarrhea (4%). Adverse events led to dose reductions in 30% versus 3% and to discontinuation in 6% versus 0%; one Grade 5 treatment-related event (pneumonia) occurred.
How should postMONARCH be interpreted given the modest PFS gain?
postMONARCH supports switching CDK4/6 inhibitors (for example from palbociclib to abemaciclib) plus fulvestrant as a biomarker-unselected option after CDK4/6-inhibitor progression, addressing an unmet need. The modest absolute investigator-assessed gain (0.7 months) versus a larger BICR benefit (7.3 months), and the discussion around informative-censoring differences between the two assessments, are key interpretive points.