Perioperative resectable NSCLC - BMS
Discover KOL Sentiment on CheckMate-77T →














Top 10 by impressions - click to view on X
Thoracic Oncologists — Siena is here Don't feel sad as #ASCO25 has no lung cancer plenary. But these lung cancer trials are unmissable: ✨ CheckMate 77T –...
Great presention at Presidential Session by Dr Tina Cascone on Checkmate 77T impressive data on perioperative IO in resected patients. Congrats to all the authors for this important trial...

Fantastic #oralabstract session today for #NSCLC, #mesothelioma, & #SCLC w/ my fabulous co-chair @_ShankarSiva at...
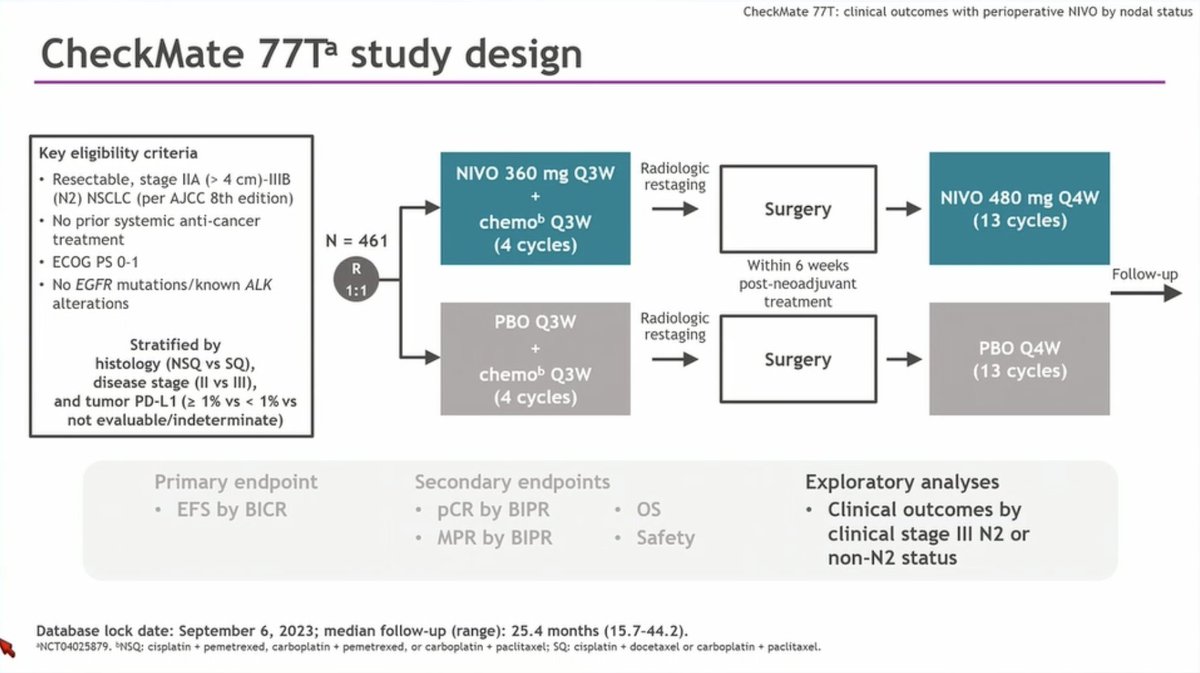
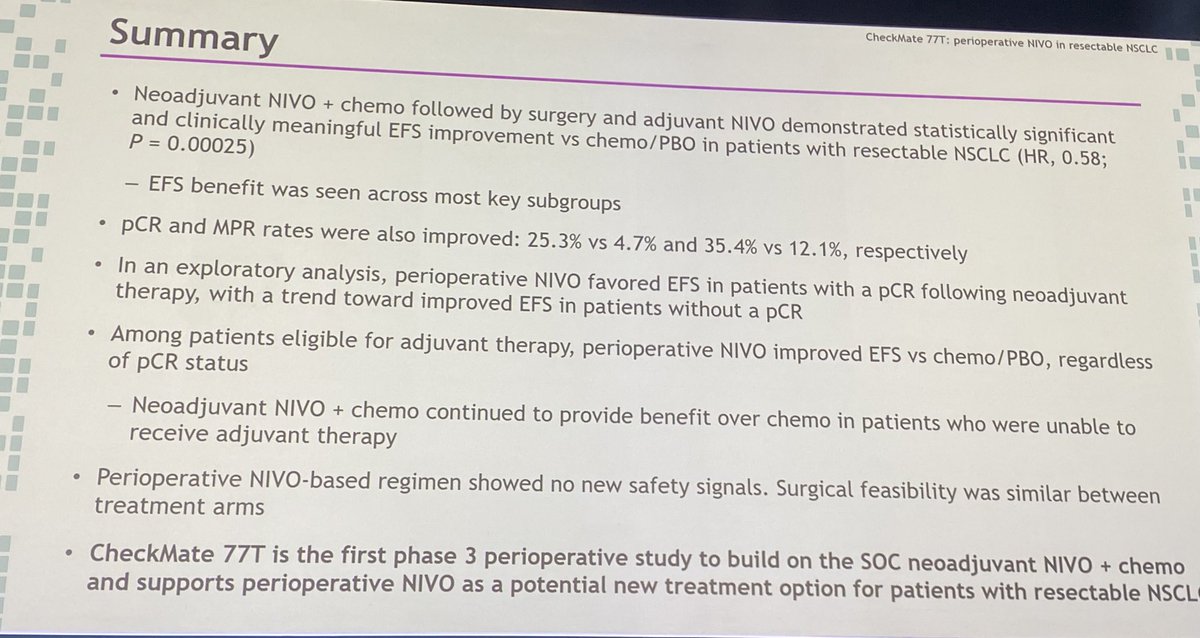
CheckMate-77T is a Phase III, randomized, double-blind, placebo-controlled multicenter trial evaluating perioperative nivolumab (Opdivo) in patients with resectable non-small cell lung cancer. The trial randomized 461 patients 1:1 to receive neoadjuvant nivolumab plus platinum-doublet chemotherapy followed by surgery and adjuvant nivolumab, versus neoadjuvant placebo plus chemotherapy followed by surgery and adjuvant placebo. CheckMate-77T is the first perioperative nivolumab regimen to receive FDA approval, establishing a new treatment paradigm for resectable NSCLC alongside the AEGEAN durvalumab approach.
Phase III, randomized (1:1), double-blind, placebo-controlled multicenter trial. Randomization was stratified by tumor PD-L1 expression (≥1% vs. <1% vs. indeterminate), disease stage (II vs. III), and tumor histology (squamous vs. nonsquamous). No companion diagnostic required.
Adults with previously untreated, resectable stage IIA (>4 cm) to select stage IIIB (T3-T4 N2) NSCLC per AJCC 8th edition, ECOG PS 0-1, eligible for complete resection. Excluded: known EGFR mutations or ALK translocations, brain metastases, active autoimmune disease, ILD, prior systemic therapy or radiotherapy for NSCLC. Demographics: median age 66 years; 71% male; 56% PD-L1 ≥1%; 64% stage III; 51% squamous histology; 90% former/current smokers.
Neoadjuvant nivolumab 360 mg IV Q3W plus histology-based platinum-doublet chemotherapy for up to 4 cycles, followed by surgery, then adjuvant nivolumab 480 mg IV Q4W for up to 13 cycles (~1 year) versus matched placebo in both phases.
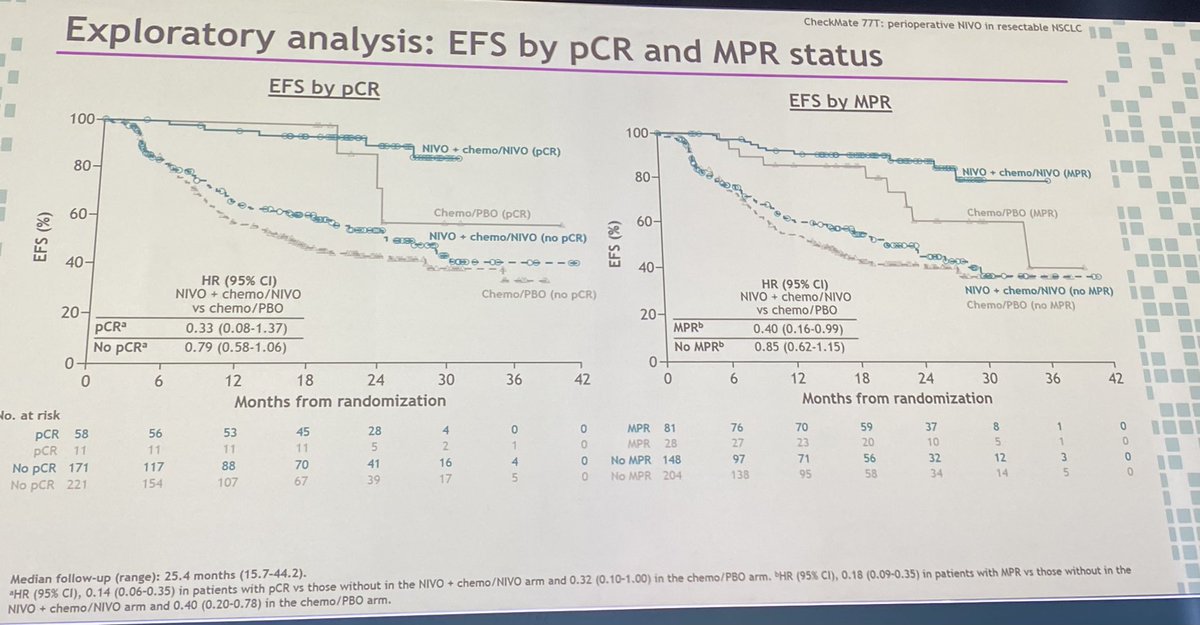
Primary endpoint: event-free survival (EFS) by blinded independent central review (BICR). Key secondary endpoints: overall survival (OS), pathological complete response (pCR) rate by blinded independent pathology review (BIPR), major pathological response (MPR) rate by BIPR, safety and tolerability.
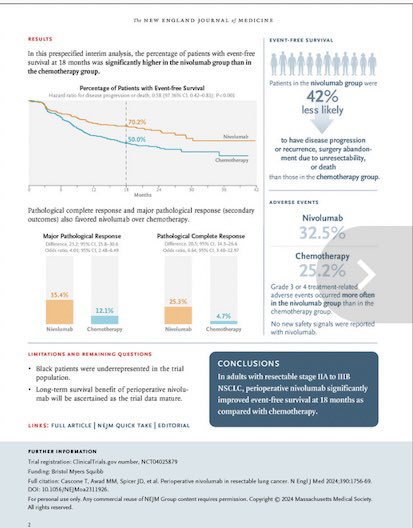
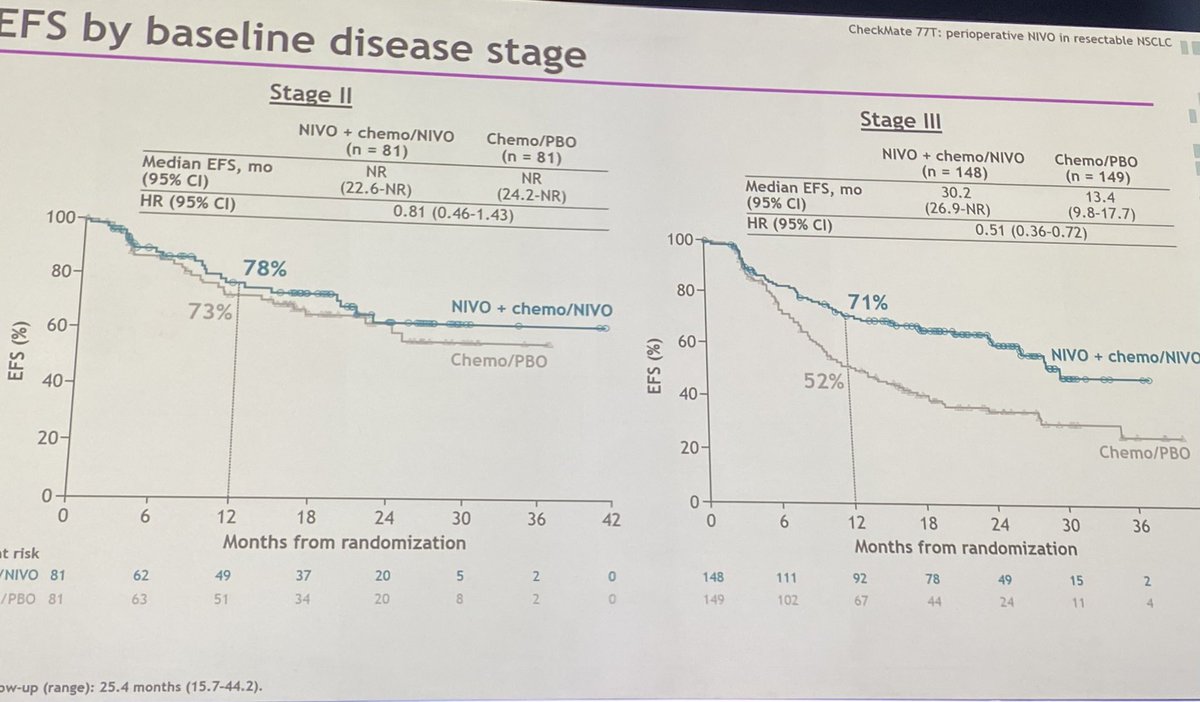
Perioperative nivolumab demonstrated a statistically significant EFS benefit versus placebo. EFS HR was 0.58 (95% CI: 0.43-0.78; p=0.00025), representing a 42% reduction in the risk of disease recurrence, progression, or death. Median EFS was not reached in the nivolumab arm versus 18.4 months with placebo. In patients who underwent surgery (78% of the nivolumab arm), EFS HR was 0.51 (95% CI: 0.37-0.72) with 1-year EFS rates of 85% versus 70%.
At the prespecified interim analysis, OS was not formally tested for statistical significance. A descriptive analysis revealed no detriment to overall survival with perioperative nivolumab. Mature OS data are pending from continued follow-up of the trial.
Grade 3-4 treatment-related AEs occurred in 32% of perioperative nivolumab patients versus 25% with placebo. Surgical cancellation due to AEs occurred in 5.3% versus 3.5%. Surgical delays due to AEs occurred in 4.5% versus 3.9%. Neoadjuvant discontinuation for AEs was 13%. During adjuvant nivolumab, permanent discontinuation occurred in 14%, most commonly due to pneumonitis (4.2%) and diarrhea (1.4%). Grade 3-4 surgery-related AEs were 12% in both arms. Grade 5 surgery-related events: 2% nivolumab versus 1% placebo.
CheckMate-77T established perioperative nivolumab as a treatment option for resectable NSCLC, joining AEGEAN (durvalumab) and CheckMate-816 (neoadjuvant-only nivolumab) as approved immunotherapy approaches in this setting. Key clinical debates include the incremental benefit of adjuvant immunotherapy over neoadjuvant-only strategies, whether pathological response can guide adjuvant treatment decisions, the choice between perioperative nivolumab (CheckMate-77T) and perioperative durvalumab (AEGEAN) in the absence of head-to-head data, and the role of PD-L1 expression in patient selection.
See the bigger picture: Physician sentiment on OPDIVO (nivolumab) across its trial portfolio →

























