Limited-stage SCLC - AstraZeneca
Discover KOL Sentiment on ADRIATIC →



















Top 10 by impressions - click to view on X
🔥🚨@OncoAlert Hot Off the Press BIG NEWS Press Release by @AstraZeneca #ADRIATIC phase 3 trial of #Durvalumab vs #Placebo after...
Overheard at Best of #ASCO24 Albuquerque: “Wait. Are you that doctor that dances while giving updates on lung cancer?” Why yes, that’s me 😂
📢🚨#ASCO24 plenary @DavidRSpigel - pivotal ADRIATIC ph III trial; adjuvant durvalumab arm after chemoradiotherapy (cCRT) ± PCI in small cell #lungcancer; ⬆️...
Ready backstage for LAURA and ADRIATIC!!! #ASCO24 plenary! @RamalingamMD @DavidRSpigel @LaurenByersMD
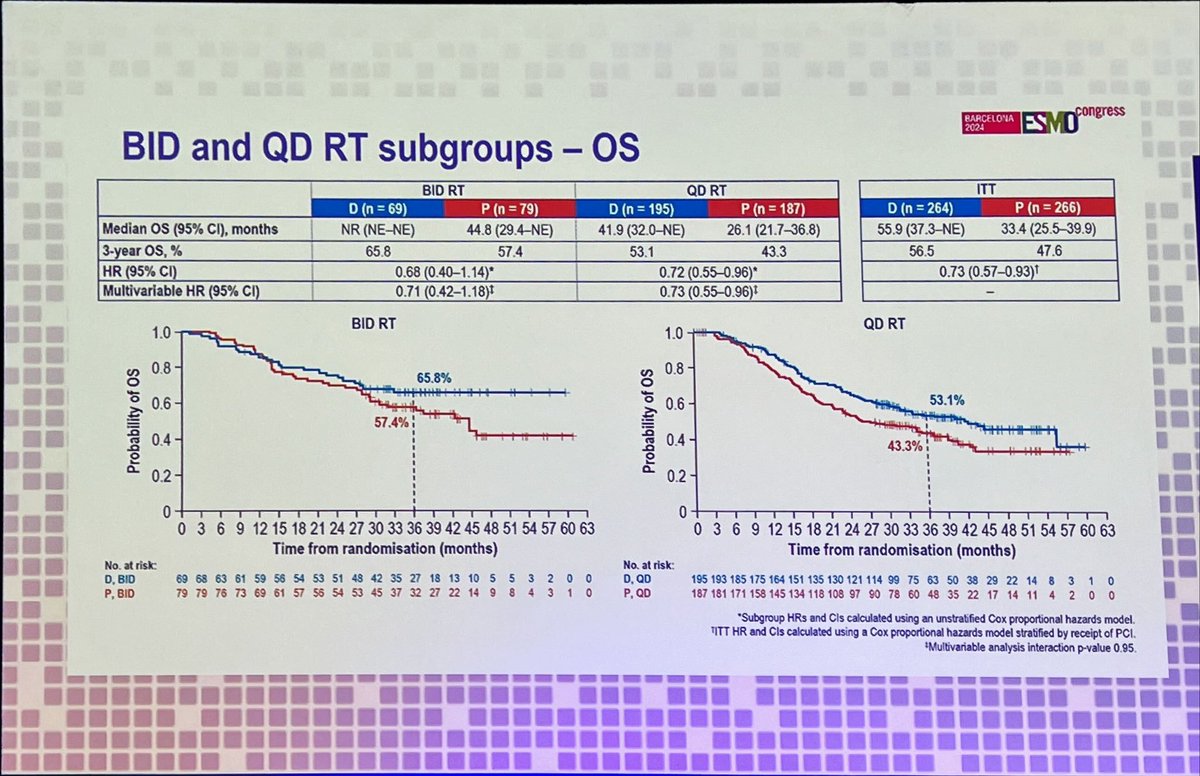
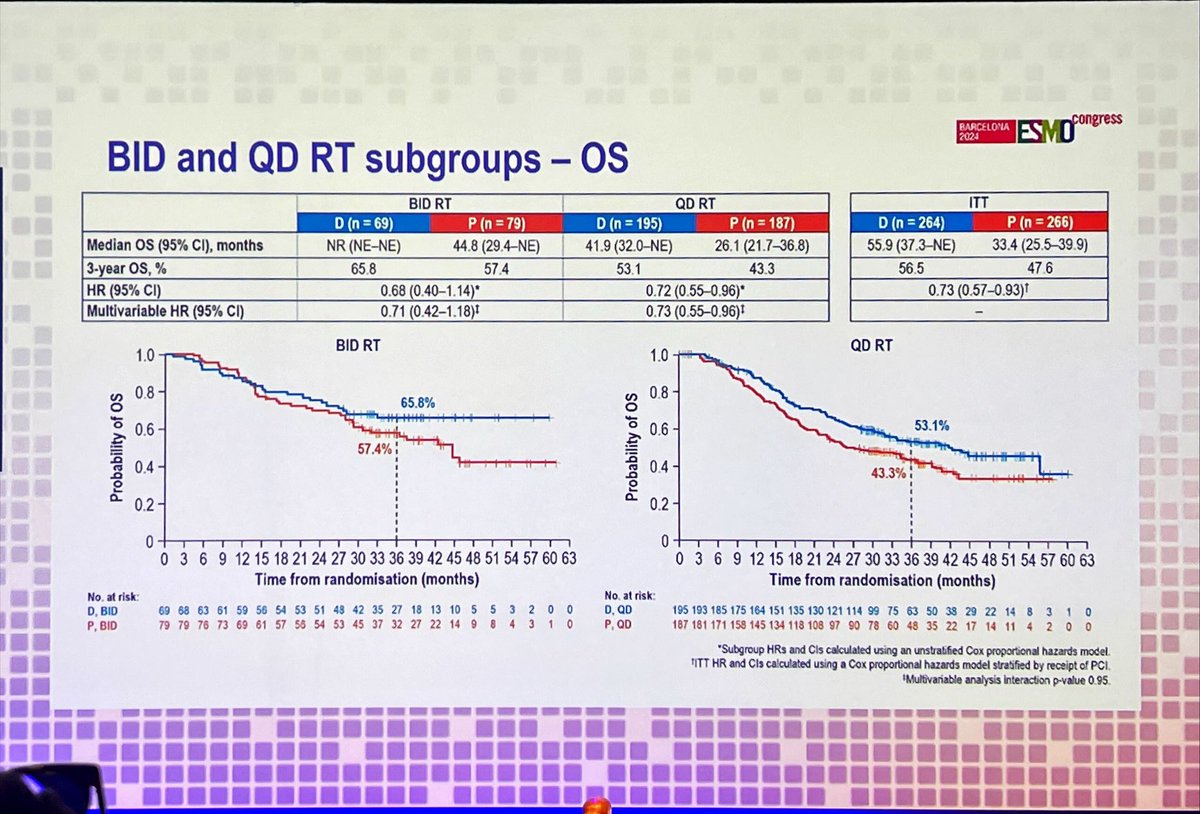
Key slide from the ADRIATIC presentation at #ESMO24 3-yr OS rates: ▶️ BD RT: 65.8% (durva) vs 57.4% (placebo) ▶️ OD RT: 53.1% (durva) vs 43.3% (placebo) ➡️ survival superior with BD...
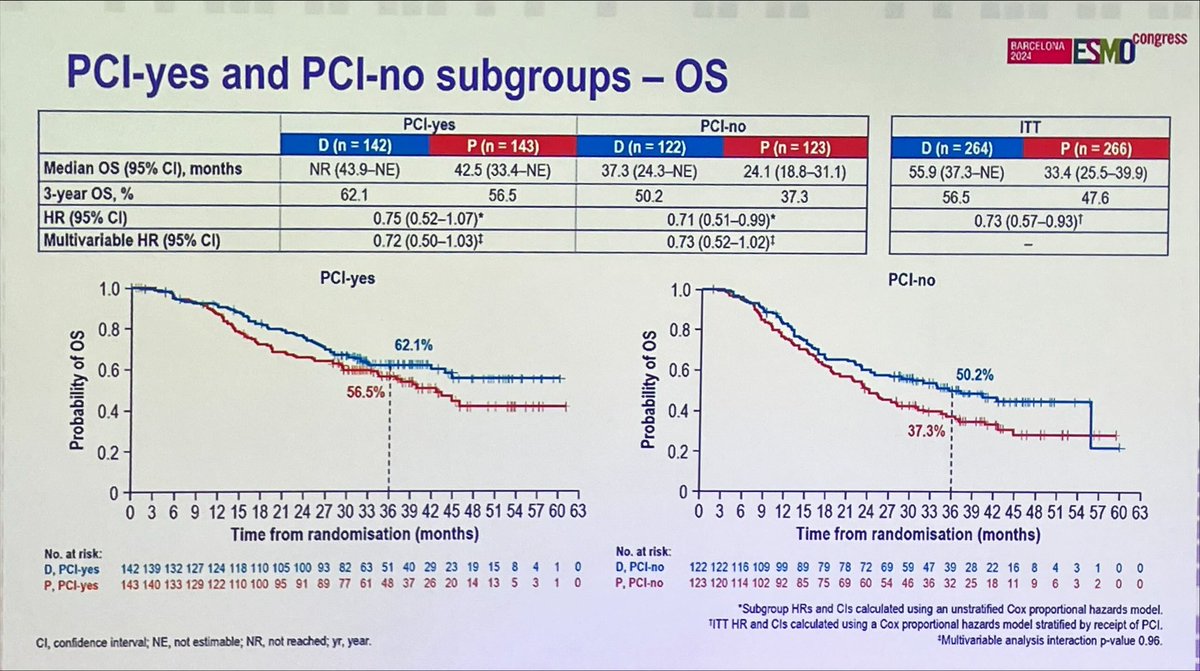
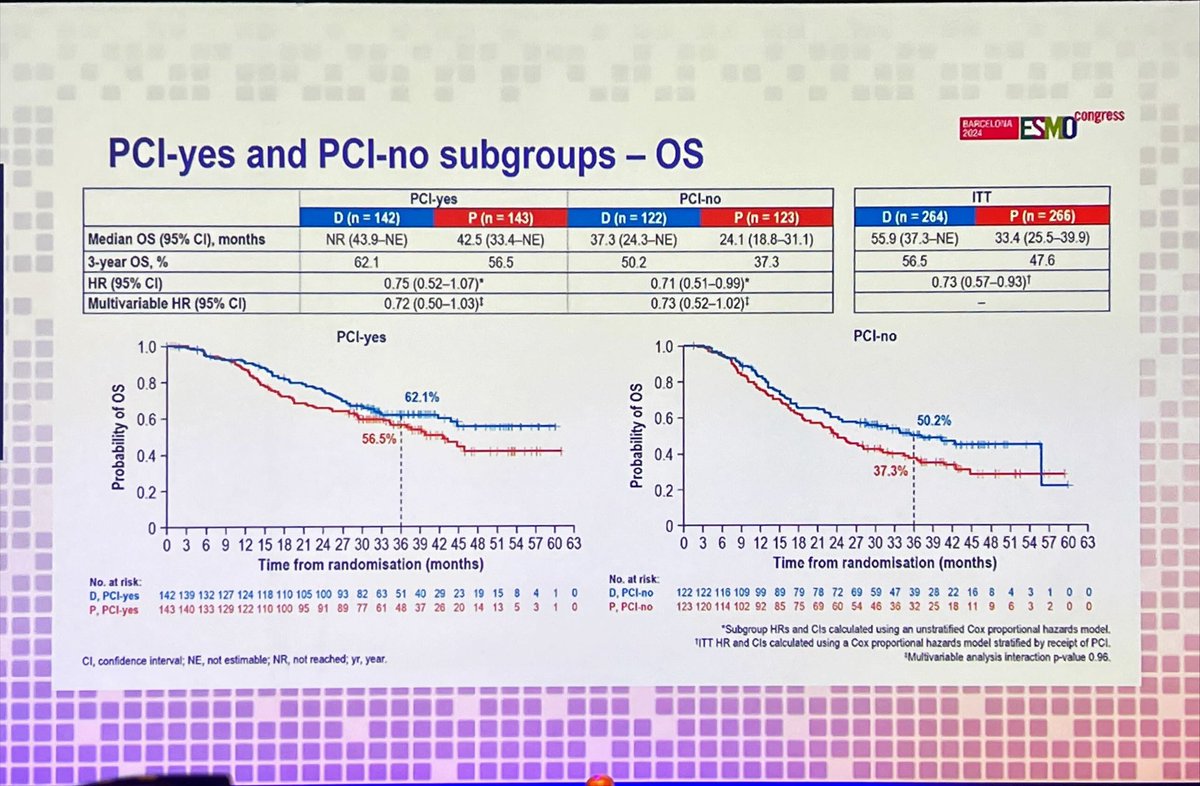
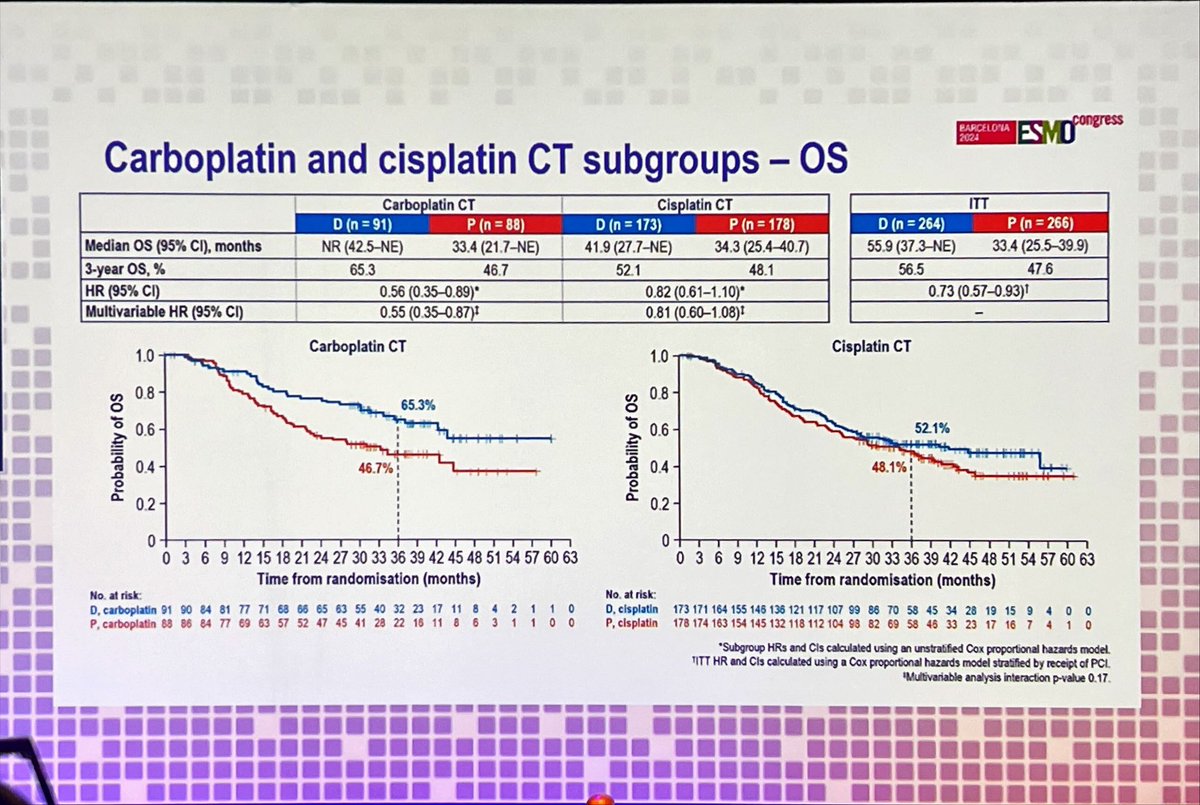
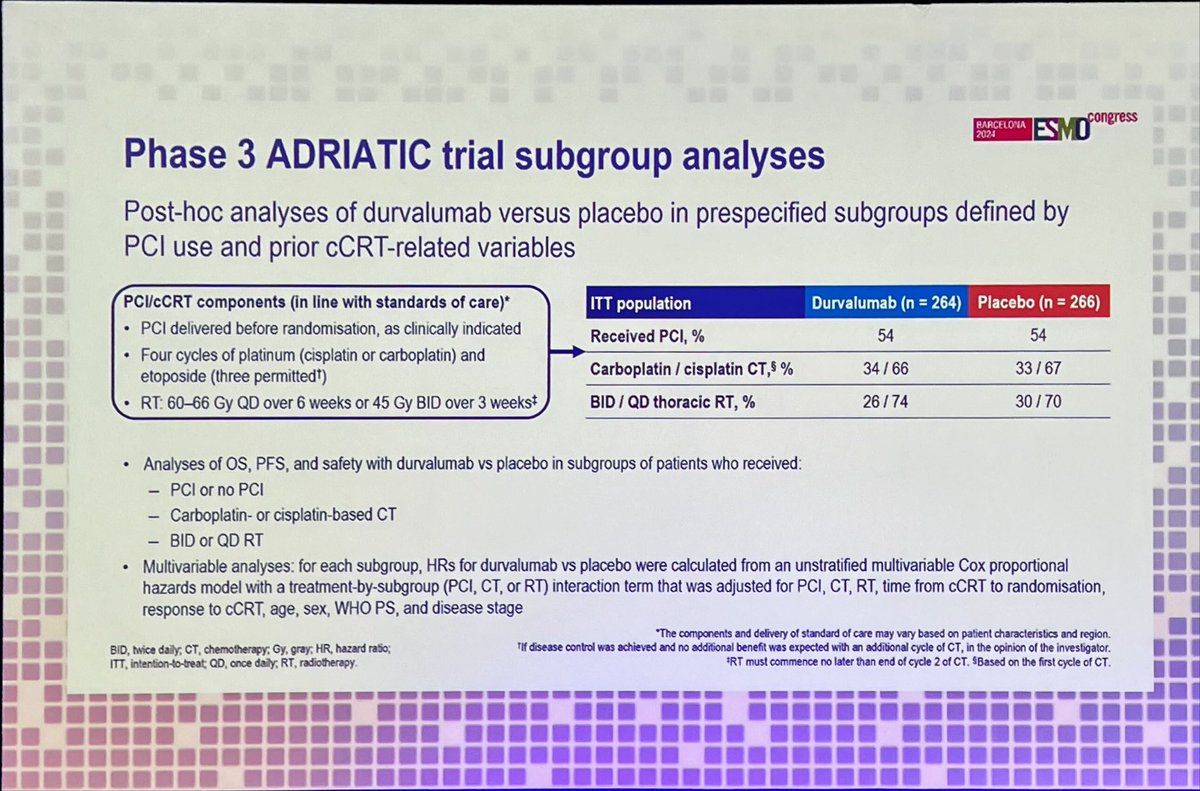
🧐 Subgroup analysis in ADRIATIC trial on consolidation durvalumab in LS-SCLC, specifically looking at the role of PCI, cis vs carbo, QD vs. BID radiation regimen. Additionally simultaneous...

ADRIATIC: relative Durva benefit in pre-specified subgroups 👉PCI: ⬆️ OS overall, but similar Durva benefit 👉Carbo v Cis: Non sig ⬆️ OS benefit 👉BD v OD RT: Comparable OS benefit 🤔 PCI in LS-SCLC...

Dr Senan presents ADRIATIC post hoc prespecified subsets. PCI delivered before randomization. Similar durva benefits for PCI Y/N. Strong durva benefit for carbo but not cis. Strong durva benefit for...

Agree, practice-changing clear improvement in efficacy, and that doesn't happen often enough in SCLC!! Kudos!!👏🎉

Second practice changing trial of the day: ADRIATIC Durva consolidation vs plb after cCRT in LS-SCLC. Dual P. endpoints OS/PFS meet (3-y FUP): 24 mo OS gain (median 55.9 vs 33.4, HR 0.73) and 24%...
ADRIATIC is a Phase 3, randomized, double-blind, placebo-controlled trial evaluating durvalumab (Imfinzi) as consolidation therapy in patients with limited-stage small cell lung cancer (LS-SCLC) who had not progressed following concurrent platinum-based chemoradiotherapy (cCRT). The trial enrolled 730 patients across 164 centers in 19 countries, randomized 1:1:1 to durvalumab monotherapy, durvalumab plus tremelimumab, or placebo. Results demonstrated that consolidation durvalumab significantly improved both overall survival and progression-free survival compared to placebo, representing the first major therapeutic advance in LS-SCLC in over 30 years. NCCN guidelines now recommend durvalumab consolidation therapy for LS-SCLC patients without progression after cCRT.
ADRIATIC is a Phase 3, randomized, double-blind, placebo-controlled, multicenter global trial (NCT03703297). Patients were randomized 1:1:1 to durvalumab 1,500 mg Q4W, durvalumab 1,500 mg + tremelimumab 75 mg Q4W (4 doses then durvalumab alone), or placebo Q4W for up to 24 months, stratified by disease stage (I/II vs III) and prior prophylactic cranial irradiation (PCI).
The trial enrolled 730 adult patients with stage I-III LS-SCLC (including stage I/II inoperable disease) with WHO/ECOG PS 0-1 whose disease had not progressed following concurrent platinum-based chemoradiotherapy. Prior PCI was permitted before randomization.
Durvalumab 1,500 mg IV every 4 weeks as consolidation monotherapy (n=264) versus placebo Q4W (n=266), administered until disease progression, unacceptable toxicity, or a maximum of 24 months. A third arm of durvalumab plus tremelimumab (n=200) remains blinded for future analysis.
Dual primary endpoints were overall survival (OS) and progression-free survival (PFS) assessed by blinded independent central review (BICR) per RECIST v1.1 for durvalumab vs placebo. Secondary endpoints included objective response rate (ORR), duration of response (DoR), OS/PFS landmark rates, and safety.
Durvalumab significantly improved PFS compared to placebo with an HR of 0.76 (95% CI: 0.61-0.95; p=0.0161). Median PFS was 16.6 months with durvalumab vs 9.2 months with placebo, a 7.4-month improvement. The 24-month PFS rate was 46.2% for durvalumab versus 34.2% for placebo (p=0.02).
Durvalumab demonstrated a statistically significant OS improvement with an HR of 0.73 (95% CI: 0.57-0.93; p=0.0104), representing a 27% reduction in the risk of death. Median OS was 55.9 months with durvalumab vs 33.4 months with placebo, a 22.5-month improvement. The 3-year OS rate was 56.5% for durvalumab versus 47.6% for placebo (p=0.01).
The safety profile was manageable and consistent with known durvalumab toxicity. Overall Grade 3-4 AE rates were similar between arms (24.4% durvalumab vs 24.2% placebo). The most common adverse reactions were pneumonitis/radiation pneumonitis (22.9% vs 23.4%) and fatigue. Treatment discontinuation due to AEs occurred in 16.4% of durvalumab patients vs 10.6% placebo, with hypothyroidism notably higher in the durvalumab arm (16.0% vs 3.8%).
Durvalumab consolidation after cCRT is now the new standard of care for LS-SCLC, representing the first major therapeutic advance in this setting in over 30 years. The FDA approved Imfinzi (durvalumab) on December 4, 2024 for adults with LS-SCLC whose disease has not progressed following concurrent platinum-based chemotherapy and radiation therapy. KOLs including Dr. David Spigel and Dr. Stephen Liu have described the results as immediately practice-changing, with Dr. Liu noting that durvalumab makes the possibility of cure a reality for more patients with LS-SCLC.