PATINA (AFT-38) is a Phase 3 trial showing that adding palbociclib (IBRANCE; Pfizer) to first-line maintenance trastuzumab (with or without pertuzumab) plus endocrine therapy extends median PFS to 44.3 vs 29.1 months (HR 0.74) in HR+/HER2+ metastatic breast cancer. On this basis the FDA approved the regimen in June 24, 2026 as first-line maintenance therapy.
FDA APPROVED June 24, 2026 — first-line maintenance, HR+/HER2+ metastatic breast cancer
The FDA approved palbociclib (IBRANCE, Pfizer) in combination with trastuzumab (with or without pertuzumab) and endocrine therapy as first-line maintenance treatment, following induction, for HR-positive, HER2-positive locally advanced or metastatic breast cancer — based on the PATINA (AFT-38) trial.
[Slide 1]
SAN ANTONIO
BREAST CANCER
AFT-38 PATINA Study Design
SYMPOSIUM
UT Health
AACR
Men Cancer Center
-
Registration
Key eligibility criteria
Palbociclib (125 mg PO QD
Histologically confirmed
D1-D21)
HR+,HER2+ mBC
Completion of induction
N=518
Trastuzumab I pertuzumab +
No prior treatment in the
chemotherapy and no
endocrine therapy*
advanced setting beyond
evidence of disease
R
Until PD
or
induction treatment
progression (i.e., CR, PR,
1:1
toxicity
.
6-8 cycles of treatment,
or SD)
including trastuzumab +
Trastuzumab + pertuzumab +
endocrine therapy*
pertuzumab and
taxane/vinorelbine
Stratification factors
Pertuzumab use (yes vs no)
The non-pertuzumab option is limited to up to 20% of the population
Prior anti-HER2 therapy in the (neo)adjuvant setting (yes vs no, including de novo)
Response to induction therapy (CR or PR vs SD) by investigator assessment
Type of endocrine therapy (fulvestrant vs aromatase inhibitor)
*Trastuzumab and pertuzumab were administered per SOC. Endocrine therapy options include an aromatase inhibitor or fulvestrant. Factors used in stratified analyses.
CR=complete response; D=day; HER2=human epidermal growth factor receptor 2; HR=hormone receptor; mBC=metastatic breast cancer; PD=progressive disease; PO=orally;
PR=partial response; QD=once a day; R=randomization; SD=stable disease; SOC=standard of care.
---
[Slide 2]
SAN ANTONIO
BREAST CANCER
Conclusions
SYMPOSIUM
UT Health
AACR
lan Antonio
American Association
Care -
Mays Cancer Center
Our results reinforce the strong scientific rationale for overcoming
resistance to anti-HER2 therapy and endocrine therapy by adding CDK4/6
inhibition
The addition of palbociclib to anti-HER2 and endocrine therapy
demonstrated a statistically significant improvement in PFS in patients
diagnosed with HR+,HER2+ advanced breast cancer in the first-line
metastatic setting
Palbociclib added to anti-HER2 and endocrine therapy had a manageable
toxicity profile and without new safety signals
CDK4/6=cyclin-dependent kinase 4/6; HER2=human epidermal growth factor receptor 2; HR=hormone receptor; PFS=progression-free survival.
[Slide 1]
SAN ANTONIO
BREAST CANCER
SYMPOSIUM
SAN ANTONIO
BREAST CANCER
Implications to Clinical Practice
SYMPOSIUM
UT Health
AACR
-
-
Ment -
The AFT-38 PATINA phase III study demonstrates a clinically meaningful
improvement in PFS among patients diagnosed with HR+, HER2+
breast cancer
Median PFS increased from 29.1 to 44.3 months (A15.2 months)
Manageable toxicity
Palbociclib added to anti-HER2 and endocrine therapy may
represent a new standard of care for patients diagnosed with
HR+, HER2+ advanced breast cancer
HER2=human epidermal growth factor receptor 2; HR=hormone receptor; PFS=progression-free survival.
This presentation is the intellectual property or the author/presenter. Contact them at Dto for permission to reprint and/or distribute
[Slide 1]
BRINGING THE WORLD OF EP TOGETHER
SAN ANTONIO
BREAST CANCER
SYMPOSIUM
Secondary endpoint: Overall Survival
SAN ANTONIO
BREAST CANCER
SYMPOSIUM
(interim analysis)
UT Health
AACR
-
- -
100
90
80
70
60
Final overall survival
50
analysis requires 247
Palbociclib Anti-
Anti-HER2 and
40
HER2 and ET
ET
events. Only 119
Events
58/261
61/257
30
Median in mos (95% CI)
NE (71.6 NE)
77 (72-NE)
observed thus far.
3-yr os, %. 95% CI
87 (82.8-91.2)
84.7 (80-89.3)
20
5-yr OS, %. 95% CI
74.3 (67.7-80.9)
69.8 (62.4-77.2)
10
Hazard ratio (95% CI)
0.86 (0.6-1.24)
0
0
6
12
18
24
30
36
42
48
54
60
66
72
78
84
Time (months)
"Kaplan-
Patients at-Risk
Meier method: Unstratified
Palbo HER2 ET
261
255
248
239
229
220
207
187
146
101
60
22
7
I
0
Cox model; Cl=confidence
HER2 ET
257
235
228
221
215
197
188
167
125
90
49
22
6
0
interval: NE=not evaluable;
OS=overall survival;
DECEMBER 10-14,2024 * SAN ANTONIO
---
[Slide 2]
BRINGING THE WORLD OF EP TOGETHER
2
SAN ANTONIO
BREAST CANCER
SYMPOSIUM
SAN ANTONIO
BREAST CANCER
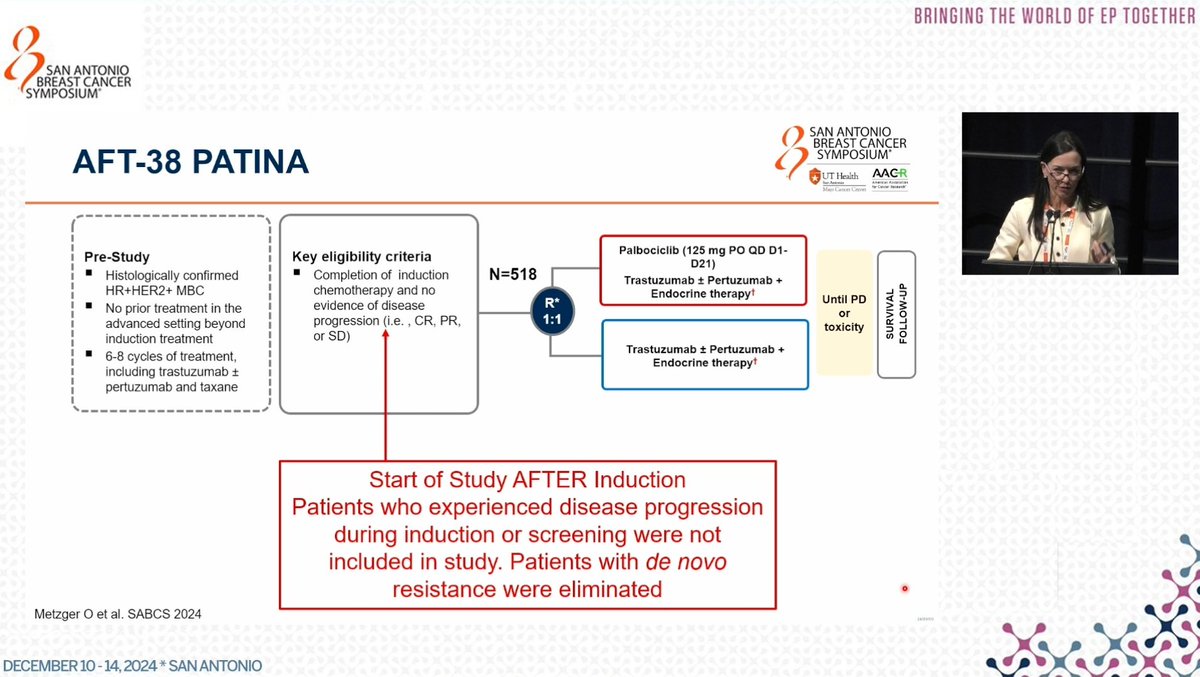
AFT-38 PATINA
SYMPOSIUM
UT Health
AACR
Key eligibility criteria
Palbociclib (125 mg PO QD D1-
Pre-Study
D21)
Histologically confirmed
Completion of induction
N=518
Trastuzumab + Pertuzumab +
HR+HER2+ MBC
chemotherapy and no
Endocrine therapy
R*
Until PD
No prior treatment in the
evidence of disease
or
advanced setting beyond
progression (i.e. , CR, PR,
1:1
toxicity
induction treatment
or SD)
Trastuzumab * Pertuzumab +
6-8 cycles of treatment,
Endocrine therapy
including trastuzumab I
pertuzumab and taxane
Start of Study AFTER Induction
Patients who experienced disease progression
during induction or screening were not
included in study. Patients with de novo
resistance were eliminated
Metzger o et al. SABCS 2024
DECEMBER 10 14, 2024 * SAN ANTONIO
[Slide 1]
&
SAN ANTONIO
BREAST CANCER
SYMPOSIUM
SAN ANTONIO
BREAST CANCER
Implications to Clinical Practice
SYMPOSIUM
UT Health
AACR
-
MayCamerCom
The AFT-38 PATINA phase III study demonstrates a clinically meaningful
improvement in PFS among patients diagnosed with HR+,HER2+
breast cancer
Median PFS increased from 29.1 to 44.3 months (A15.2 months)
Manageable toxicity
Palbociclib added to anti-HER2 and endocrine therapy may
represent a new standard of care for patients diagnosed with
HR+,HER2+ advanced breast cancer
HER2=human epidermal growth factor receptor 2: HR=hormone receptor PFS=progression-free survival.
This presentation is the intelectual property of the author/presenter Contact them at Other CL for permission to reprint and/or distribute
---
[Slide 2]
SAN ANTONIO
BREAST CANCER
Conclusions
SYMPOSIUM
UT Health
AACR
Sex Annoid
American Association
Mays Cancer Center
for Cancer Research
Our results reinforce the strong scientific rationale for overcoming
resistance to anti-HER2 therapy and endocrine therapy by adding CDK4/6
inhibition
The addition of palbociclib to anti-HER2 and endocrine therapy
demonstrated a statistically significant improvement in PFS in patients
diagnosed with HR+,HER2+ advanced breast cancer in the first-line
metastatic setting
Palbociclib added to anti-HER2 and endocrine therapy had a manageable
toxicity profile and without new safety signals
CDK4/6=cyclin-dependent kinase 4/6; HER2=human epidermal growth factor receptor 2; HR=hormone receptor; PFS=progression-free survival.
---
[Slide 3]
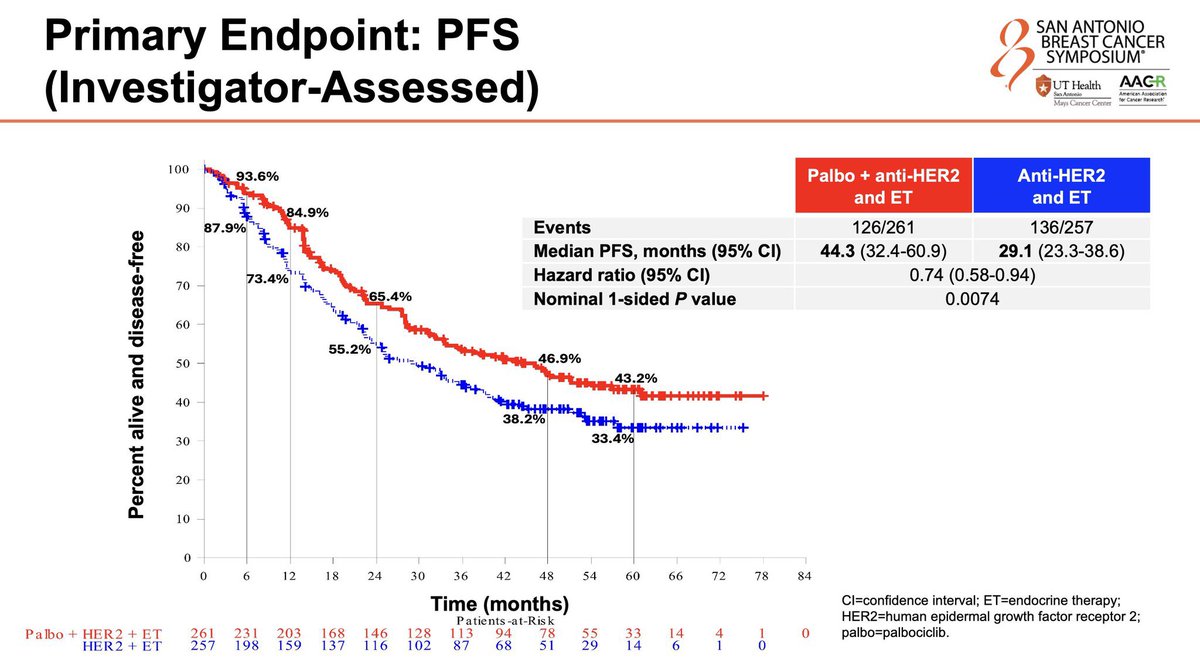
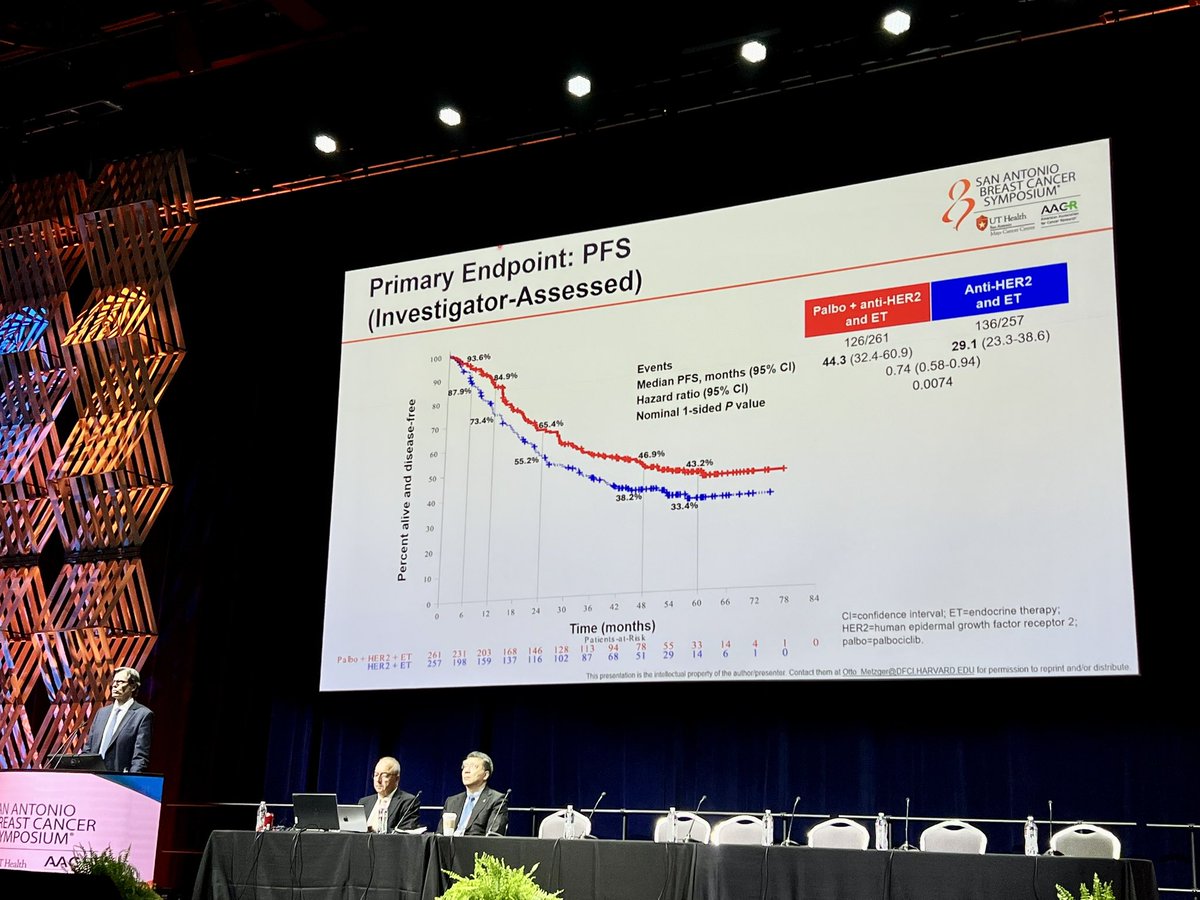
Primary Endpoint: PFS
SAN ANTONIO
BREAST CANCER
SYMPOSIUM
(Investigator-Assessed)
UT Health
AACR
San Americ
Mays Cancer Center
for Cancer Research
100
93.6%
Palbo + anti-HER2
Anti-HER2
and ET
90
and ET
84.9%
87.9%
Events
126/261
136/257
80
Median PFS, months (95% CI)
44.3 (32.4-60.9)
29.1 (23.3-38.6)
73.4%
70
Hazard ratio (95% CI)
0.74 (0.58-0.94)
65.4%
Nominal 1-sided P value
0.0074
60
55.2%
50
46.9%
43.2%
40
38.2%
HH
30
33.4%
20
10
0
0
6
12
18
24
30
36
42
48
54
60
66
72
78
84
Time (months)
Cl=confidence interval; ET=endocrine therapy;
Patients-at-Risk
HER2=human epidermal growth factor receptor 2;
Palbo + HER2
261
231
203
168
146
128
113
94
78
55
33
14
4
1
0
palbo=palbociclib.
HER2 ET
257
198
159
137
116
102
87
68
51
29
14
6
1
0
---
[Slide 4]
SAN ANTONIO
BREAST CANCER
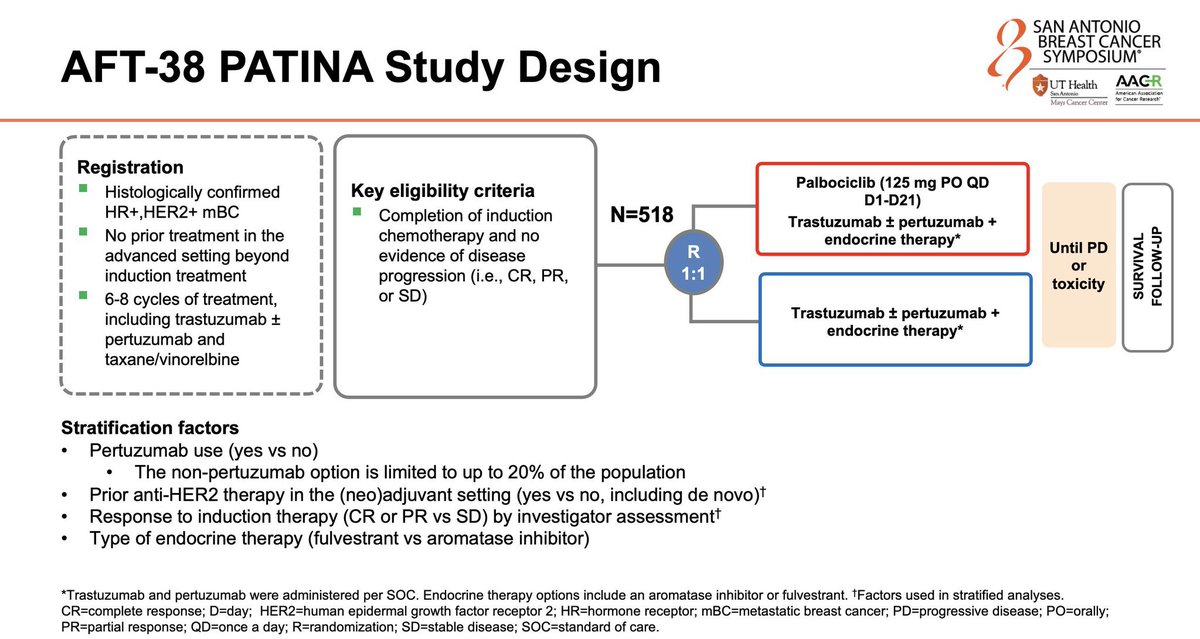
AFT-38 PATINA Study Design
SYMPOSIUM
UT Health
AACR
Sen Antonio
American Association
for Cancer Research
Mays Cancer Center
Registration
Key eligibility criteria
Palbociclib (125 mg PO QD
Histologically confirmed
D1-D21)
HER2+ mBC
Completion of induction
N=518
Trastuzumab + pertuzumab +
No prior treatment in the
chemotherapy and no
endocrine therapy*
advanced setting beyond
R
Until PD
evidence of disease
or
induction treatment
progression (i.e., CR, PR,
1:1
toxicity
SURVIVAL
FOLLOW-UP
6-8 cycles of treatment,
or SD)
including trastuzumab +
Trastuzumab + pertuzumab +
pertuzumab and
endocrine therapy*
taxane/vinorelbine
Stratification factors
Pertuzumab use (yes VS no)
The non-pertuzumab option is limited to up to 20% of the population
Prior anti-HER2 therapy in the (neo)adjuvant setting (yes VS no, including de novo)+
Response to induction therapy (CR or PR VS SD) by investigator assessment
Type of endocrine therapy (fulvestrant VS aromatase inhibitor)
*Trastuzumab and pertuzumab were administered per SOC. Endocrine therapy options include an aromatase inhibitor or fulvestrant. Factors used in stratified analyses.
CR=complete response; D=day; HER2=human epidermal growth factor receptor 2; HR=hormone receptor; mBC=metastatic breast cancer; PD=progressive disease; PO=orally;
PR=partial response; QD=once a day; R=randomization; SD=stable disease; SOC=standard of care.
[Slide 1]
QUESTIONS AHEAD OF
DESTINY-Breast09 AT ASCO 2025
1. How strong will the benefit be?
1. PATINA vs. CLEOATRA
2. Is sequential T-Dxd use an option?
1. os differential between 1st line - 2nd line
3. What to give after T-Dxd?
4. Proionged T-Dxd use and managing
ILD risk
[Slide 1]
SAN ANTONIO
Primary Endpoint: PFS
BREAST CANCER
SYMPOSIUM
UT Health AACR
(Investigator-Assessed)
butes
-
I I I
100
Palbo + anti-HER2
Anti-HER2
93.6%
and ET
and ET
90
84.9%
Events
126/261
136/257
87.9%
so
Median PFS, months (95% CI)
44.3 (32.4-60.9)
29.1 (23.3-38.6)
73.4%
Hazard ratio (95% CI)
0.74 (0.58-0.94)
70
Percent alive and disease-free
65.4%
Nominal 1-sided P value
0.0074
60
55.2%
46.9%
50
43.2%
40
38.2%
33.4%
30
20
10
0
0
6
12
18
24
30
36
42
48
54
60
66
72
78
84
Time (months)
Cl=confidence Interval; ET=endocrine therapy;
Patients-at-Risk
HER2=human epidermal growth factor receptor 2;
Pabo . HER2 ET
261
231
203
168
146
128
113
94
78
55
33
14
4
I
0
palbo=palbociclib.
HER2 ET
257
198
159
137
116
102
87
68
51
29
14
6
I
0
This presentation is the intellectual property of the authoripresenter Contact them at Offe for permission to reprint and/or distribute
i
,
,
PATINA is a clinical trial evaluating Palbociclib + anti-HER2 therapy + endocrine therapy in HR+/HER2+ metastatic breast cancer. Sponsored by Pfizer / Genentech. KOL discussion spans multiple conferences with 53 tracked posts from 30 oncology opinion leaders generating 202.9K total impressions.
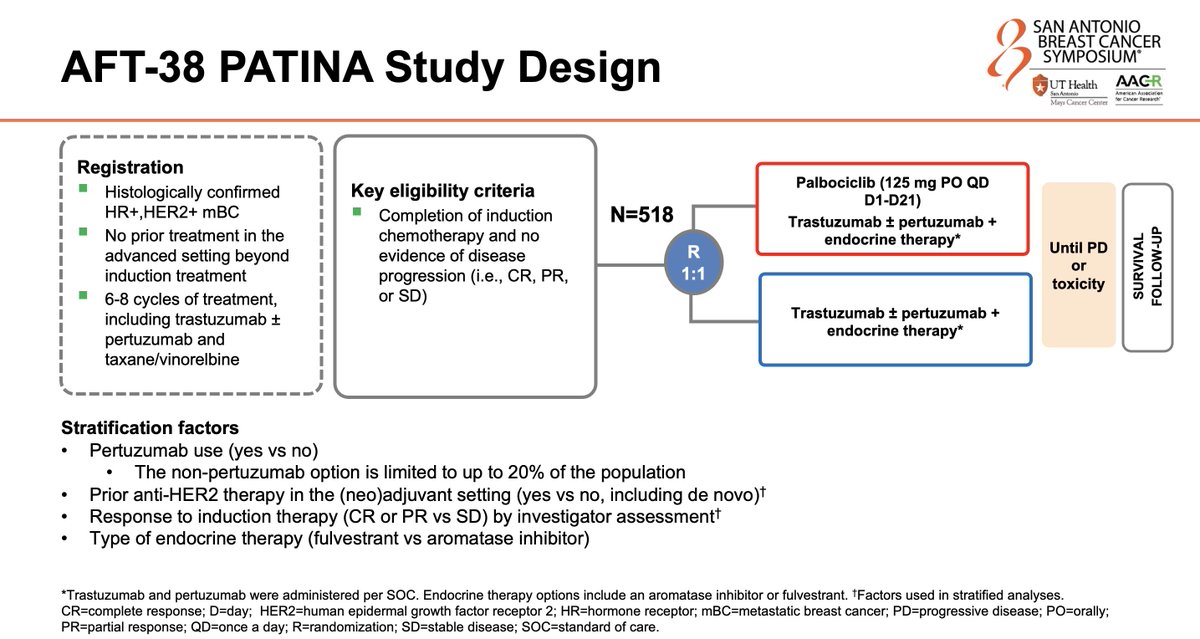
Phase 3, randomized (1:1), open-label, international trial evaluating palbociclib added to maintenance anti-HER2 and endocrine therapy after induction chemotherapy in HR+/HER2+ metastatic breast cancer. Sponsored by Alliance Foundation Trials.
Population
Adults with HR-positive, HER2-positive metastatic breast cancer who completed 4-8 cycles of induction chemotherapy plus HER2-targeted therapy without disease progression.
Interventions
Ibrance (palbociclib) plus anti-HER2 therapy (trastuzumab with or without pertuzumab) plus endocrine therapy versus anti-HER2 therapy plus endocrine therapy alone.
PATINA (AFT-38) is a randomized Phase 3 trial testing whether adding palbociclib (IBRANCE) to first-line maintenance anti-HER2 therapy (trastuzumab, with or without pertuzumab) plus endocrine therapy improves outcomes versus anti-HER2 therapy plus endocrine therapy alone, after induction chemotherapy, in HR-positive, HER2-positive metastatic breast cancer.
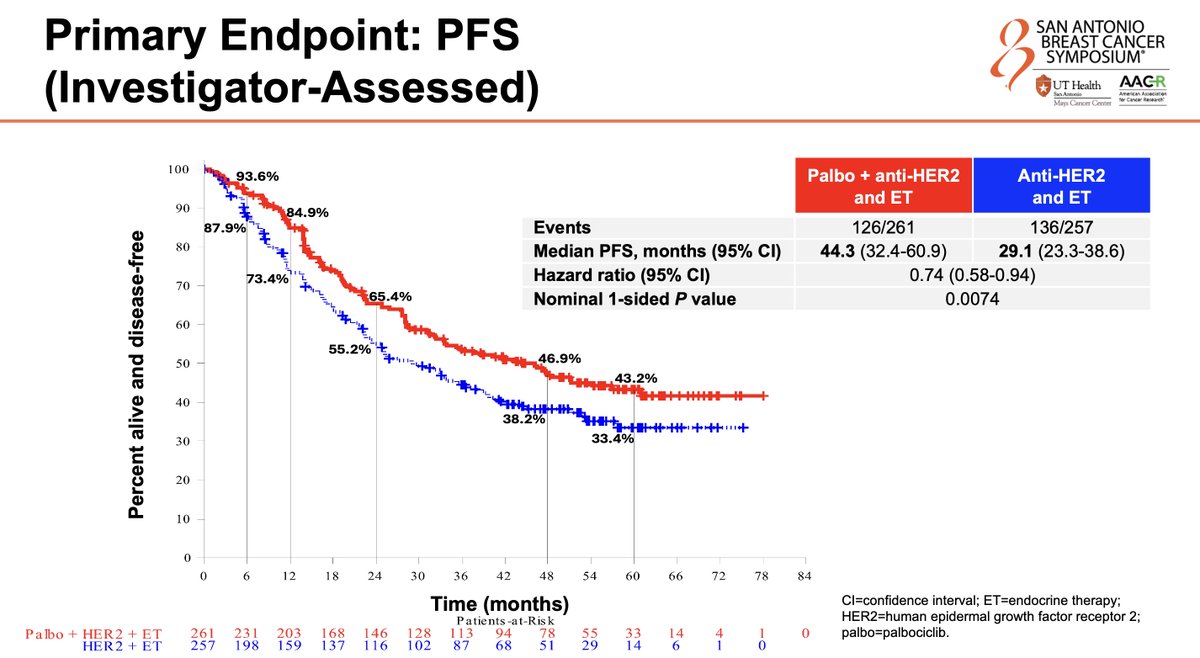
What were the PATINA progression-free survival results?
Median progression-free survival was 44.3 versus 29.1 months - about a 15-month improvement - favoring the palbociclib regimen (HR 0.74; P=.0074, reported at SABCS 2024; the FDA review cited HR 0.76, P=.0134).
Is palbociclib FDA approved for HER2-positive breast cancer?
Yes. In June 24, 2026 the FDA approved palbociclib (IBRANCE) in combination with trastuzumab, with or without pertuzumab, and endocrine therapy as first-line maintenance treatment for HR-positive, HER2-positive locally advanced or metastatic breast cancer, based on PATINA.
What is the approved PATINA regimen and dose?
Palbociclib (IBRANCE) plus trastuzumab (Herceptin), with or without pertuzumab (Perjeta), plus endocrine therapy, as maintenance following induction. The palbociclib dose is 125 mg orally once daily for 21 days, followed by 7 days off, in 28-day cycles.
Who sponsored PATINA and what is its trial identifier?
PATINA (AFT-38) was sponsored by Alliance Foundation Trials and funded by Pfizer; the principal investigator was Otto Metzger. Its ClinicalTrials.gov identifier is NCT02947685.