[Slide 1]
!
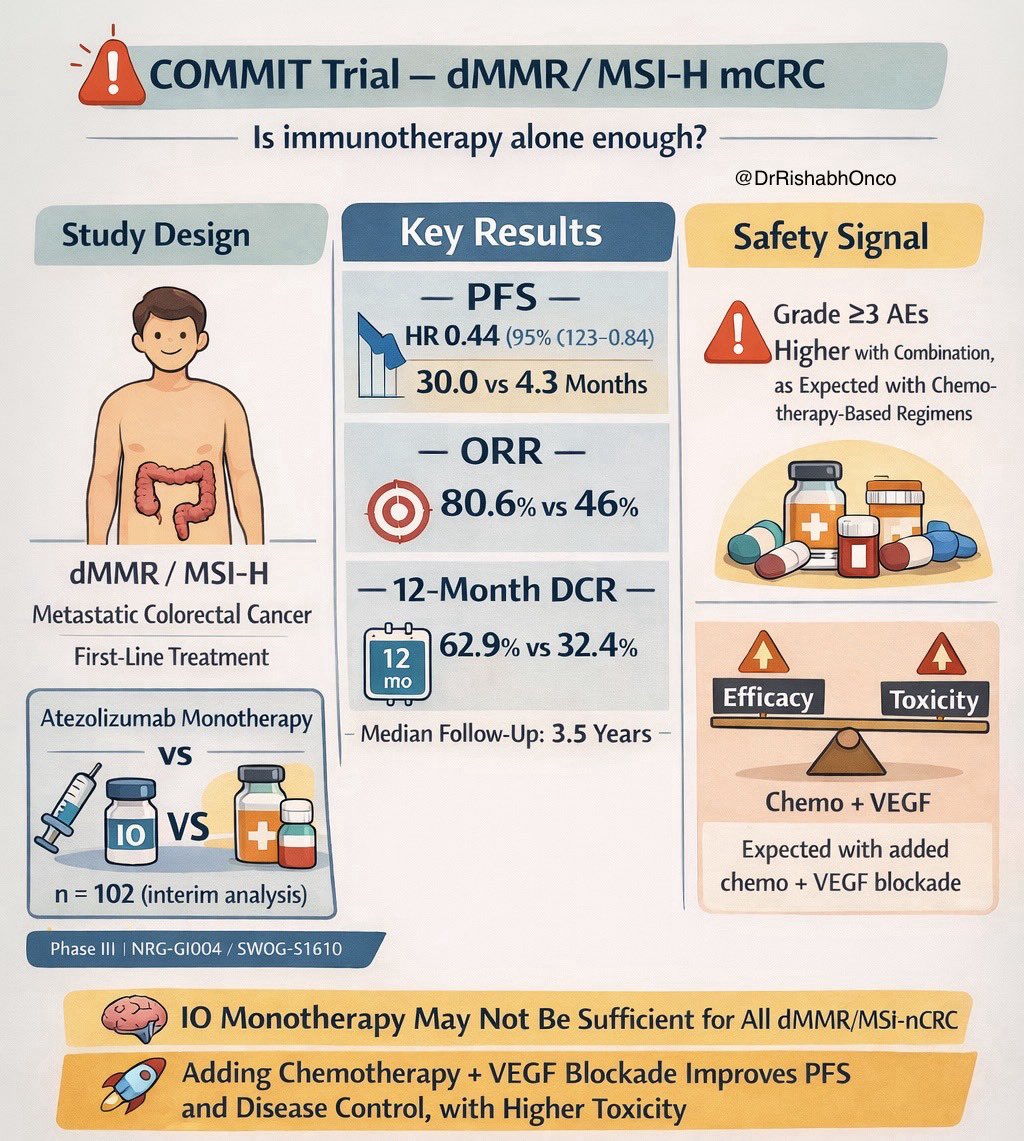
COMMIT Trial - dMMR/MSI-H mCRC
Is immunotherapy alone enough?
@
DrRishabhOnco
Study Design
Key Results
Safety Signal
— PFS -
Grade ≥3 AEs
HR 0.44 (95% (123-0.84)
!
Higher with Combination,
30.0 vs 4.3 Months
as Expected with Chemo-
therapy-Based Regimens
- ORR -
80.6% vs 46%
dMMR/MSI-H
- 12-Month DCR -
Metastatic Colorectal Cancer
0-0
First-Line Treatment
12
62.9% vs 32.4%
mo
Efficacy
Toxicity
Atezolizumab Monotherapy
- Median Follow-Up: 3.5 Years -
vs
Chemo + VEGF
IO
VS
+
Expected with added
chemo + VEGF blockade
n = 102 (interim analysis)
Phase III I NRG-GI004 / SWOG-S1610
IO Monotherapy May Not Be Sufficient for All dMMR/MSi-nCRC
Adding Chemotherapy + VEGF Blockade Improves PFS
and Disease Control, with Higher Toxicity
[Slide 1]
NRG
Study Design
ONCOLOGY
Marring Improving Check
FFX/Bevacizumab
FFX/bevacizumab
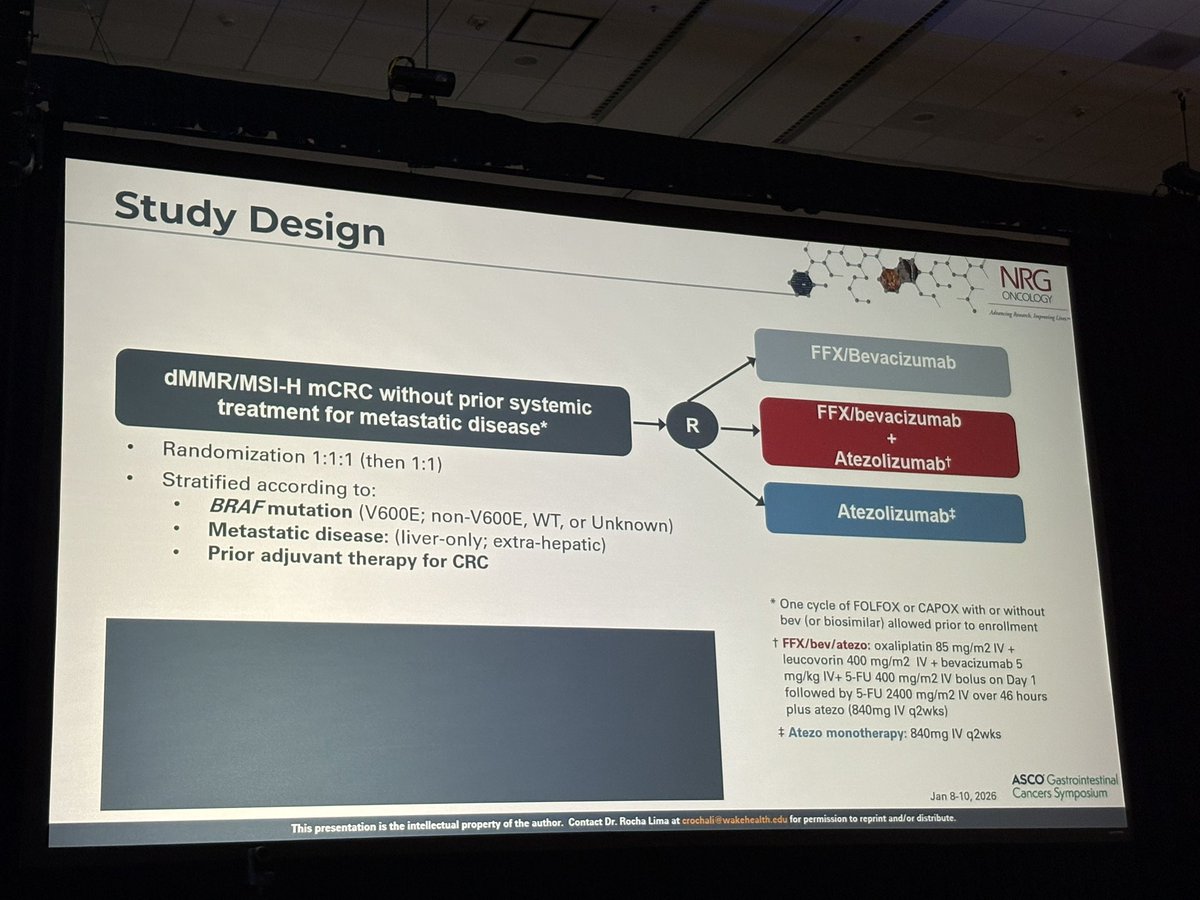
dMMR/MSI-H mCRC without prior systemic
R
+
treatment for metastatic disease*
Atezolizumab+
Randomization 1:1:1 (then 1:1)
Stratified according to:
Atezolizumab*
BRAF mutation (V600E; non-V600E, WT, or Unknown)
Metastatic disease: (liver-only; extra-hepatic)
Prior adjuvant therapy for CRC
* One cycle of FOLFOX or CAPOX with or without
bev (or biosimilar) allowed prior to enrollment
t FFX/bev/atezo: oxaliplatin 85 mg/m2 IV +
leucovorin 400 mg/m2 IV + bevacizumab 5
mg/kg IV+ 5-FU 400 mg/m2 IV bolus on Day 1
followed by 5-FU 2400 mg/m2 IV over 46 hours
plus atezo (840mg IV q2wks)
# Atezo monotherapy: 840mg IV q2wks
ASCO Gastrointestinal
Jan 8-10, 2026
Cancers Symposium
This presentation is the intellectual property of the author. Contact Dr. Rocha Lima at crochali wakehealth edu for permission to reprint and/or distribute.
---
[Slide 2]
NRG
Progression-free Survival
ONCOLOGY
belowing Frown -
1.0
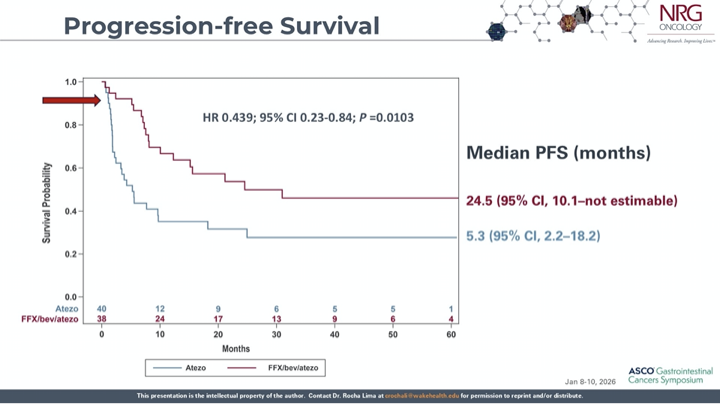
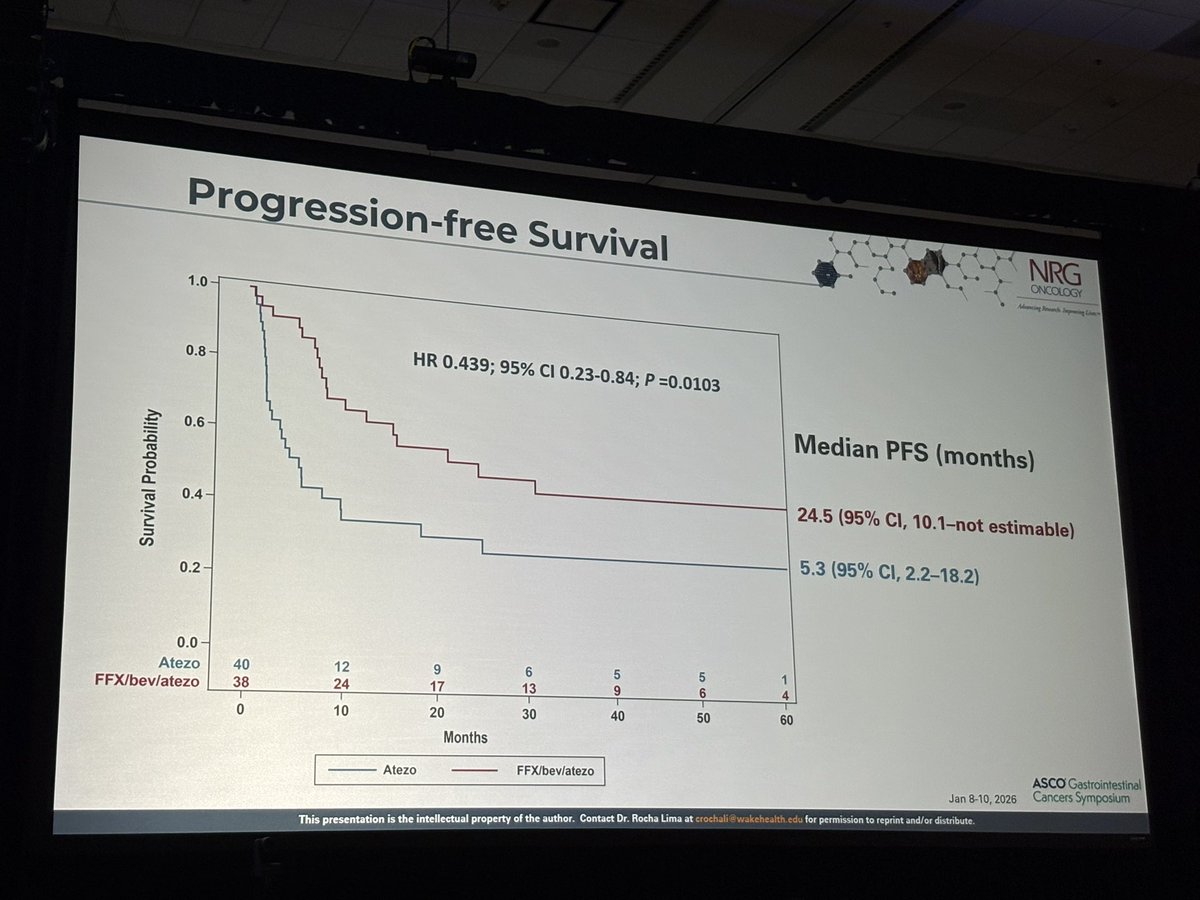
HR 0.439; 95% CI 0.23-0.84; P =0.0103
0.8
Median PFS (months)
0.6
Survival Probability
24.5 (95% CI, 10.1-not estimable)
0.4
5.3 (95% CI, 2.2-18.2)
0.2
0.0
Atezo
40
12
9
6
5
5
1
FFX/bev/atezo
38
24
17
13
9
6
4
0
10
20
30
40
50
60
Months
Atezo
FFX/bev/atezo
ASCO Gastrointestinal
Jan 8-10, 2026
Cancers Symposium
This presentation is the intellectual property of the author. Contact Dr. Rocha Lima at crochali wakehealth edu for permission to reprint and/or distribute.
---
[Slide 3]
NRG
Additional Efficacy Outcomes
ONCOLOGY
Branch Improving -
Efficacy Outcome
FFX/bev/atezo
Atezo
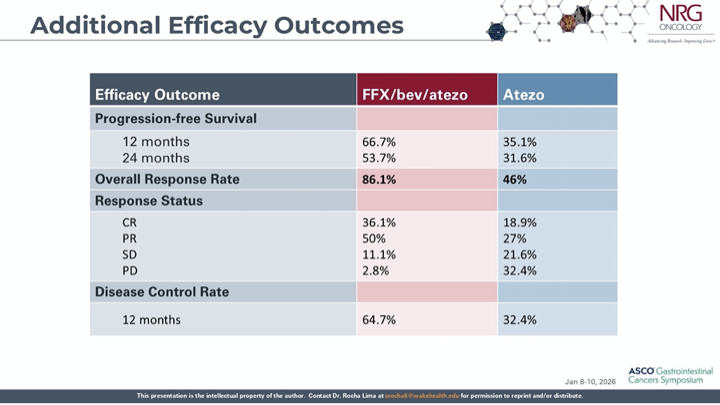
Progression-free Survival
12 months
66.7%
35.1%
24 months
53.7%
31.6%
Overall Response Rate
86.1%
46%
Response Status
CR
36.1%
18.9%
PR
50%
27%
SD
11.1%
21.6%
PD
2.8%
32.4%
Disease Control Rate
12 months
64.7%
32.4%
ASCO Gastrointestinal
Jan 8-10, 2026
Cancers Symposium
This presentation is the intellectual property of the author. Contact Dr. Rocha Lima at crochali wakehealth edu for permission to reprint and/or distribute.
---
[Slide 4]
NRG
Conclusions
ONCOLOGY
Advancing boards Importing -
The combination of FFX/bev/atezo demonstrated a statistically significant
improvement in PFS compared to atezo monotherapy in the first-line
setting for dMMR/MSI-H mCRC
HR 0.439; 95% CI 0.23-0.84, P=0.0103
FFX/bev/atezo resulted in improved complete responses and reduced
progressive disease compared to atezo monotherapy
Complete response: 36.1% vs 18.9%
Progressive disease: 2.8% vs 32.4%
Higher rates of G3-4 diarrhea, neutropenia, hypertension, and infection
observed in the FFX/bev/atezo arm
Future efforts are needed to characterize the subsets of dMMR/MSI-H CRC
that require intensification of therapy beyond single-agent PD-1/PD-L1
therapy.
Ongoing correlative analyses will hopefully provide deeper mechanistic
interpretation of the differential outcomes across treatment arms.
ASCO Gastrointestinal
Jan 8-10, 2026
Cancers Symposium
This presentation is the intellectual property of the author. Contact Dr. Rocha Lima at crochali wakehealth edu for permission to reprint and/or distribute.
[Slide 1]
ASCO GI 2026
Abstract 14 COMMIT Trial
M
Triple Combo in
dMMR/MSI-H Colorectal
Cancer
Adding Chemo + Bevacizumab to Atezolizumab dramatically improves PFS
compared to Atezolizumab alone.
1
THE "MONOTHERAPY GAP"
WHY THIS TRIAL?
Single-agent checkpoint inhibitors (like
Pembrolizumab in KEYNOTE-177) are
THE COMMIT STRATEGY
standard but still leave room for
improvement
+
+
Atezolizumab
Bevacizumab
FOLFOX
Superiority?
Objective:
Boost Efficacy with Combo
2
PHASE 3 DESIGN (TREE VIEW)
Experimental
ARM A
Atezo + Bev FOLFOX
PATIENT POPULATION
Checkpoint Inhibitor Anti-VEGF Chemotherapy
Previously
Untreated
Metastatic CRC
Control
ARM B
dMMR MSI-H Only
Atezolizumab Mono
Single Agent Immunotherapy
stopped early due CheckMate results arm)
PROGRESSION-FREE SURVIVAL
4
RESPONSE & SAFETY
3
(PFS)
HR 0.44 (Huge Benefit)
OBJECTIVE RESPONSE RATE
MEDIAN PFS
Combo Arm
$6.1%
24.5 Mo
Mono Arm
46.0%
SAFETY TRADE-OFF
5.3 Mo
Grade 3-5 AEs (Combo)
83%
Grade 3-5 AEs (Mono)
44%
Combination Arm
Atezolizumab Mono
*More toxicity with more drugs.
CLINICAL TAKEAWAY
The COMMIT trial establishes FOLFOX Bevacizumab Atezolizumab as a highly active option for dMMR/MSI H mCRC,
significantly outperforming single-agent Atezolizumab However, this comes at the cost of higher toxicity.
SOURCE REFERENCE
Rocha Lima CMSP, et al. "Combination Chemotherapy, Bevactzumab, Atezolizumab
Prof. Dr. Mustafa Ozdogan
Prolongs PFS... in dMMR/MSI-H mCRC".
STANBUL MEMORIAL GOZTEPE
CANCER CENTER
Presented at: 2026 ASCO Gastrointestinal Cancers Symposium. Abstract 14.
---
[Slide 2]
NRG
Progression-free Survival
ONCOLOGY
Advancing Amount Impouning Line
1.0
HR 0.439; 95% CI 0.23-0.84; P =0.0103
0.8
Median PFS (months)
0.6
Survival Probability
24.5 (95% CI, 10.1-not estimable)
0.4
5.3 (95% CI, 2.2-18.2)
0.2
0.0
Atezo
40
12
9
6
5
5
1
FFX/bev/atezo
38
24
17
13
9
6
4
0
10
20
30
40
50
60
Months
Atezo
FFX/bev/atezo
ASCO Gastrointestinal
Jan 8-10, 2026
Cancers Symposium
Addresses the ~40% primary resistance to PD-1 monotherapy seen in KEYNOTE-177. Triplet improves PFS and ORR significantly vs. atezolizumab monotherapy — but without head-to-head data vs. pembrolizumab monotherapy. Potential option for fit dMMR/MSI-H patients prioritizing deeper responses and reduced early-progression risk. Does not supplant KEYNOTE-177 as the label-approved standard.
Median PFS was 24.5 months with atezolizumab + mFOLFOX6 + bevacizumab vs. 5.3 months with atezolizumab monotherapy (HR 0.439, 95% CI 0.23-0.84, P=0.0103). ORR: 80.6% vs. 46%. Early progression: 2.8% vs. 32.4% — triplet eliminates the ~30% primary resistance seen with atezolizumab alone. Study closed early after meeting primary endpoint.
Higher Grade ≥3 AEs with the triplet driven by chemotherapy backbone (neutropenia, peripheral neuropathy). Atezolizumab monotherapy had lower toxicity but a much higher early progression rate (32.4% vs. 2.8%).
Higher chemo-related AEs offset by dramatic drop in early progression
⚠️ Does not supplant KEYNOTE-177 but addresses primary resistance. Addresses the ~40% primary resistance to PD-1 monotherapy seen in KEYNOTE-177. Triplet improves PFS and ORR significantly vs. atezolizumab monotherapy — but without head-to-head data vs. pembrolizumab monotherapy. Potential option for fit dMMR/MSI-H patients prioritizing deeper responses and reduced early-progression risk. Does not supplant KEYNOTE-177 as the label-approved standard.