DESTINY-Breast06 is a Phase 3 trial of trastuzumab deruxtecan (T-DXd, Enhertu) versus physician's-choice chemotherapy in HR-positive, HER2-low or HER2-ultralow metastatic breast cancer after progression on endocrine therapy. In the HER2-low population, T-DXd improved median PFS to 13.2 vs 8.1 months (HR 0.62; p<0.0001), supporting FDA approval on January 27, 2025. Sponsor: Daiichi Sankyo / AstraZeneca.
Discover KOL Sentiment on DESTINY-Breast06 →Design — Phase 3, open-label; T-DXd (Enhertu) 5.4 mg/kg vs physician's-choice chemo, HR+ HER2-low/ultralow metastatic BC after ET, n=866 (NCT04494425). (NEJM)
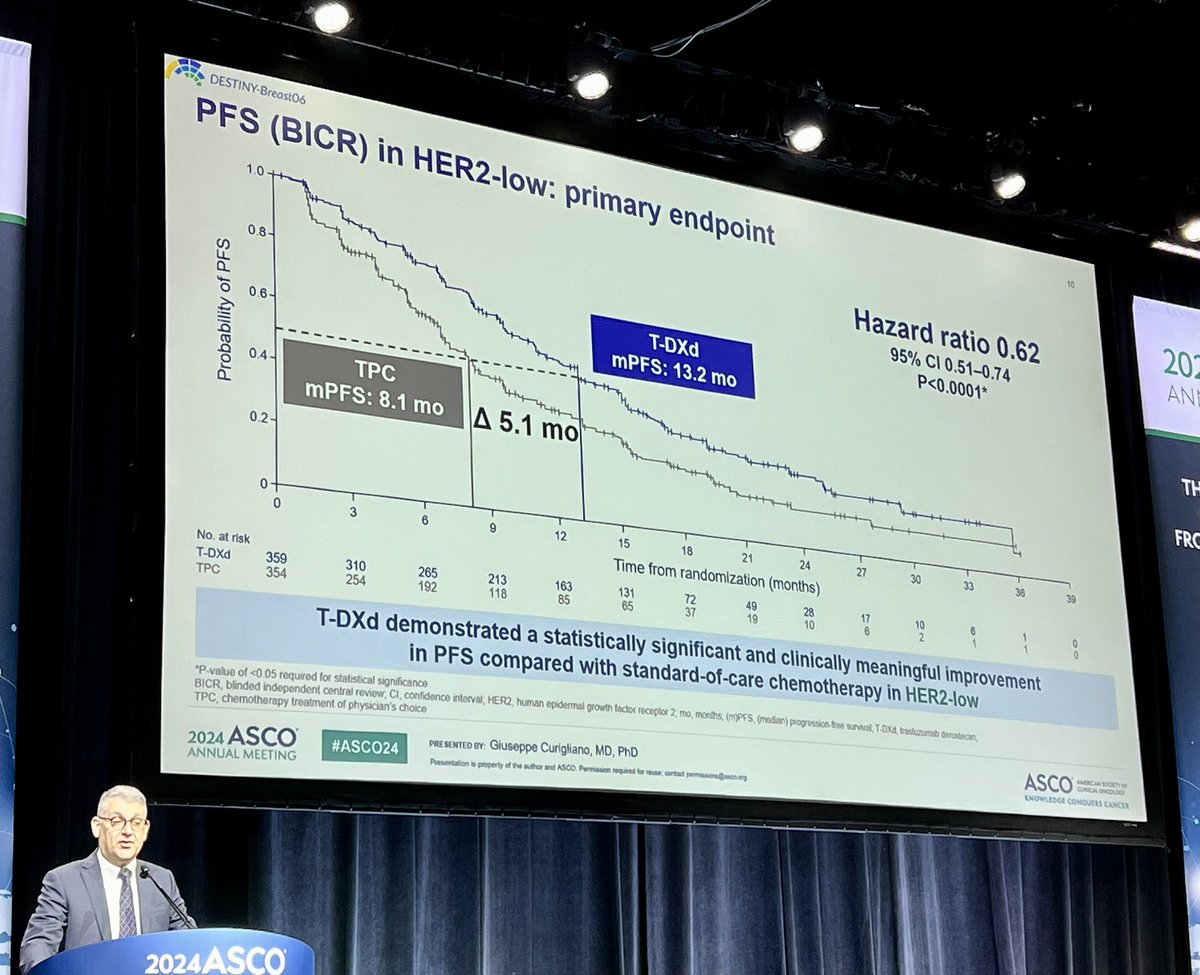
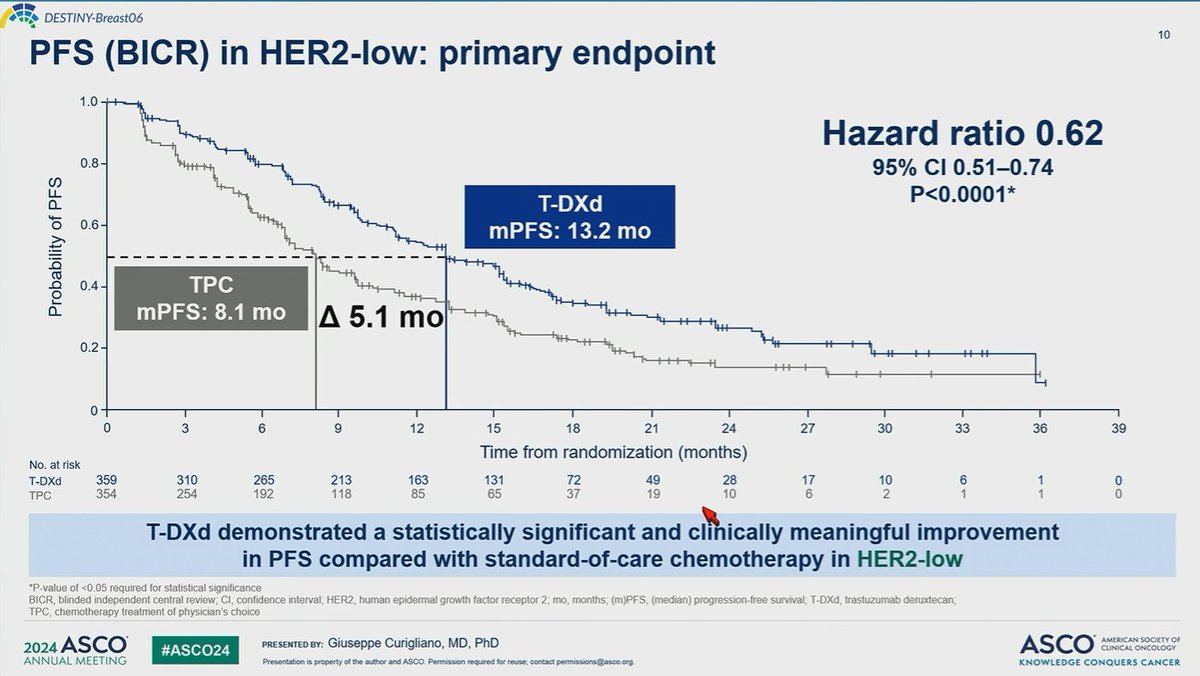
PFS (HER2-low, primary) — Median 13.2 vs 8.1 months; HR 0.62 (95% CI 0.52-0.75; p<0.0001). (NEJM)
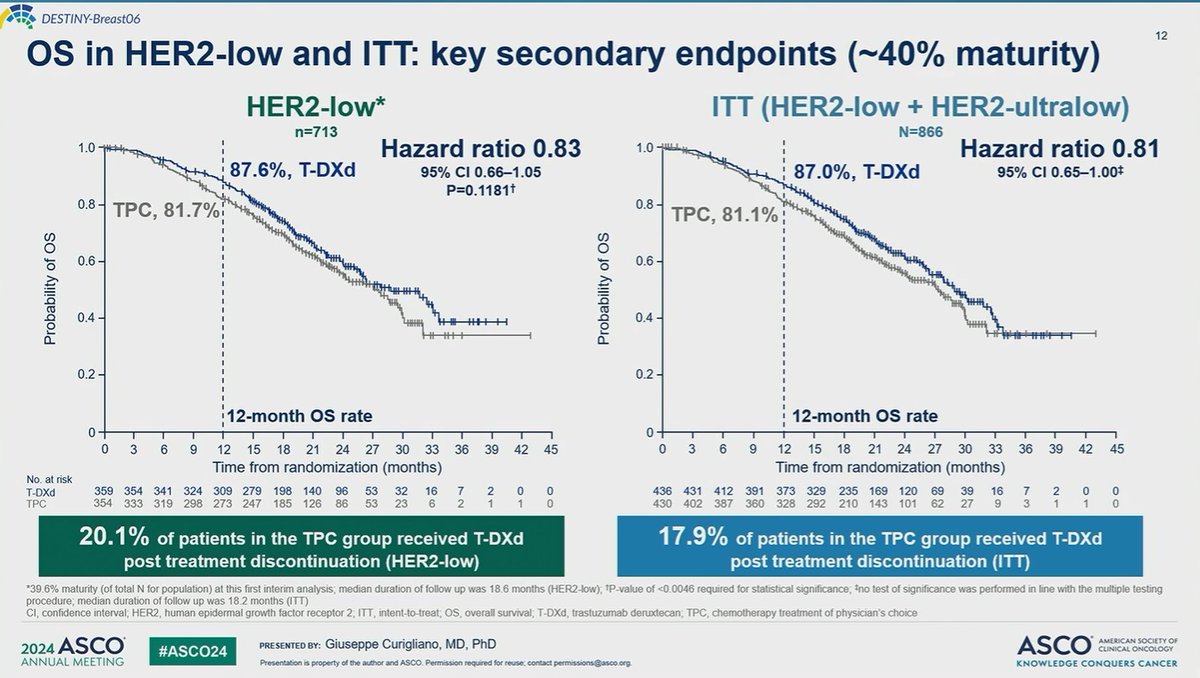
Overall survival — Immature at PFS final analysis (cutoff Mar 18, 2024, ~39% events); interim 12-mo OS 87.0% vs 81.1% (ITT). (interim)
Safety — Grade >=3 TRAEs 40.6% vs 31.4% (median treatment nearly 2x longer: 11.0 vs 5.6 mo); ILD monitored per class labeling. (NEJM)
Regulatory — FDA approved January 27, 2025; first HER2-directed therapy active in HER2-ultralow disease. (FDA.gov)
Sponsor / Drug — Daiichi Sankyo / AstraZeneca; T-DXd (Enhertu), a HER2-directed antibody-drug conjugate. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.











Top 10 by impressions - click to view on X
NEWS FROM INDUSTRY Results from the DESTINY-Breast06 trial indicate that trastuzumab deruxtecan🧪could become a new standard of care for #HER2 -low 🧬and HER2-ultralow metastatic...
#ASCO24 DESTINY-Breast06: T-DXd vs TPC in pts with HR+/ HER2-low or HER2-ultralow PFS Low➡️13.2 vs 8.1 mo Ultralow➡️13.2 vs 8.3 mo ORR Low➡️56.5 vs 32.2% Ultralow➡️61.8 vs...
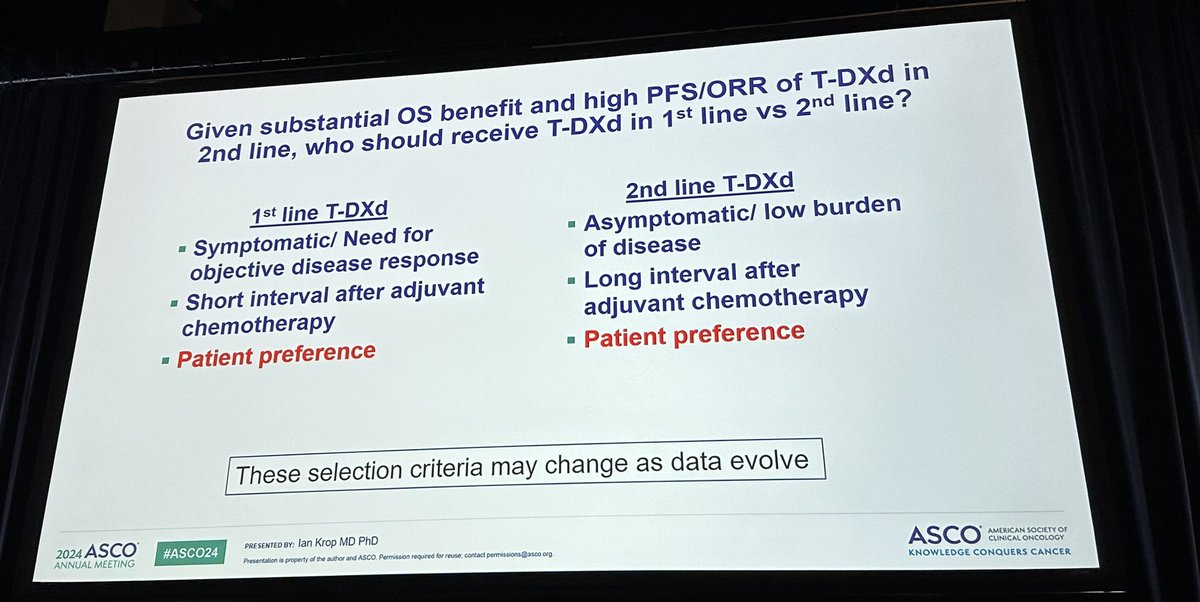
Great discussion by dr Krop @Yale: here the new algorithm for the management of hormone receptor-positive/HER2-negative advanced #BreastCancer after #ASCO24...
T-DXd is now approved for the 1L cytotoxic treatment of patients with HR+/HER2-low or #ultralow MBC, based on the results of DB06. Best suited in this 1L setting for pts with...

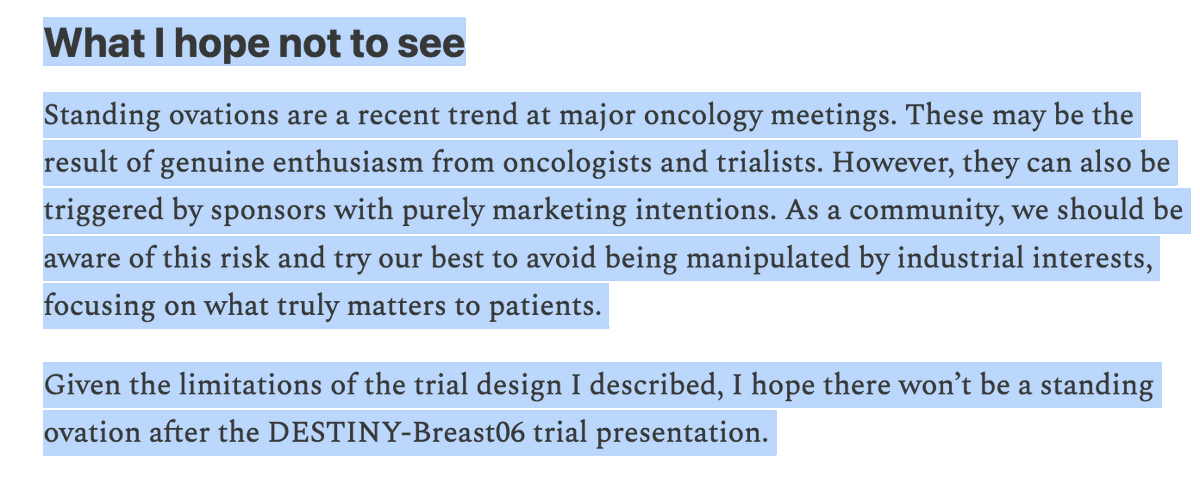
In today's post of Drug Development Letter, check out why I hope there won’t be a standing ovation after the DESTINY-Breast06 trial presentation at ASCO-2024❗️ subscribe for...
Giuseppe Curigliano (@curijoey) presents DB06. Among pts with endocrine-refractory HR+ HER2-low/ultralow MBC, 1L T-DXd significantly & meaningfully improved PFS over chemo (13.2 vs...
ASCO 2024: @DaiichiSankyoUS leadership comments on DESTINY-Breast06 at #ASCO24. Full video:

Ian Krop #ASCO24 discussed imp DB06 data. Decisions 1st v 2nd line based on disease extent/aggressiveness of dse. He is sold on ultralow - I am perhaps more conservative but the...

$AZN #DaiichiSankyo Destiny-Breast06 ENHERTU (T-DXd) demonstrated a mPFS of 13.2mo in HR+ HER2-low and HER2-ultralow metastatic breast cancer after >= 1 lines of endocrine...
Post-DB06 nomenclature for HER2, from the @myESMO Consensus Statements on HER2-low breast cancer
DESTINY-Breast06 is a Phase III, randomized, open-label trial that established trastuzumab deruxtecan (T-DXd, Enhertu) as a new standard of care for patients with HR-positive, HER2-low or HER2-ultralow metastatic breast cancer following progression on endocrine therapy. The trial randomized 866 patients (713 HER2-low, 153 HER2-ultralow) to T-DXd 5.4 mg/kg Q3W versus physician's choice chemotherapy. DESTINY-Breast06 is the first trial to demonstrate efficacy of a HER2-directed therapy in the HER2-ultralow population, fundamentally redefining the HER2 classification spectrum and moving T-DXd earlier in the treatment paradigm, prior to chemotherapy.
Phase III, global, randomized (1:1), open-label, multicenter trial (NCT04494425) in patients with HR-positive, HER2-low (IHC 1+ or IHC 2+/ISH-) or HER2-ultralow (IHC 0 with membrane staining) advanced or metastatic breast cancer. HER2 status was determined centrally using the Ventana PATHWAY anti-HER-2 (4B5) Rabbit Monoclonal Primary Antibody assay. Patients were chemotherapy-naive in the metastatic setting and had received at least one prior line of endocrine-based therapy. Stratified by prior CDK4/6 inhibitor use, HER2 expression level, and prior taxane exposure.
Adults with HR-positive, HER2-low or HER2-ultralow advanced/metastatic breast cancer who were chemotherapy-naive in the metastatic setting. Eligible patients had received 2 or more lines of endocrine therapy for metastatic disease, or 1 line of endocrine therapy with progression within 6 months of starting first-line ET plus CDK4/6 inhibitor, or disease recurrence within 24 months of starting adjuvant ET. Prior CDK4/6 inhibitor use in 90% of patients. Median age 57 years; approximately 40% ECOG PS 1 or higher; approximately 30% de novo metastatic.
T-DXd 5.4 mg/kg intravenously every 3 weeks (n=436) versus physician's choice single-agent chemotherapy (n=430): capecitabine (60%), nab-paclitaxel (24%), or paclitaxel (16%).
Primary endpoint: PFS by BICR (RECIST v1.1) in the HER2-low population. Key secondary endpoints: PFS by BICR in the overall ITT population (HER2-low + HER2-ultralow), OS in the HER2-low population, OS in the overall population. Other secondary endpoints: ORR, DOR, time to subsequent treatments, safety, and patient-reported outcomes.
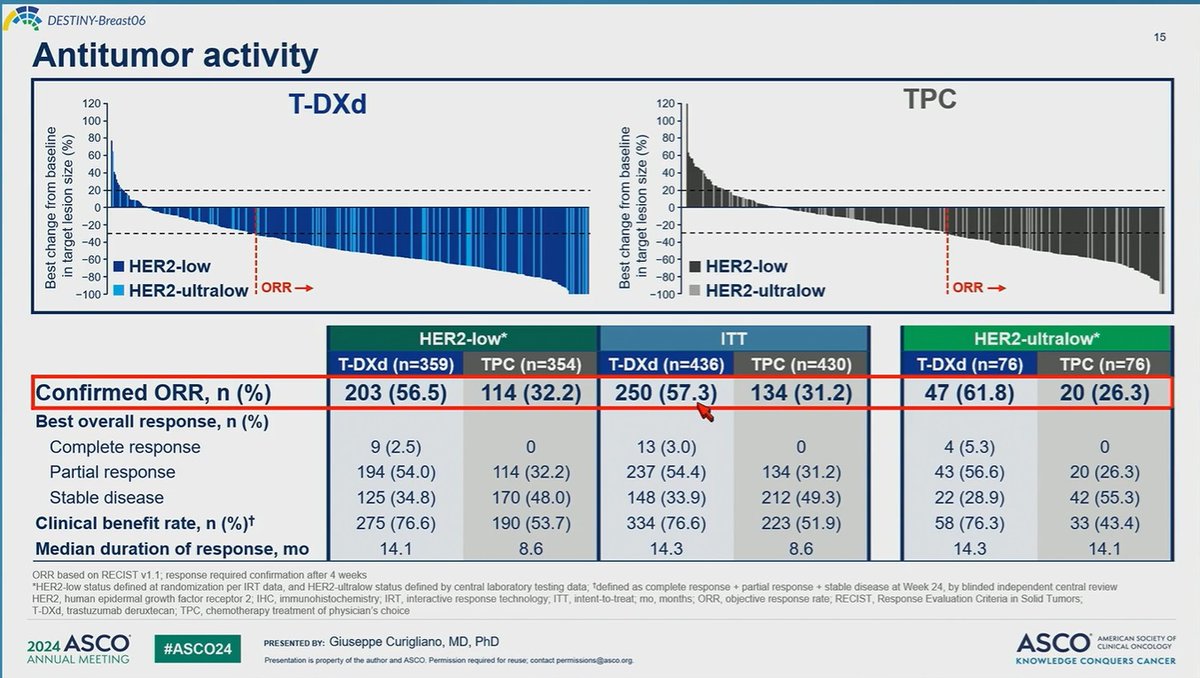
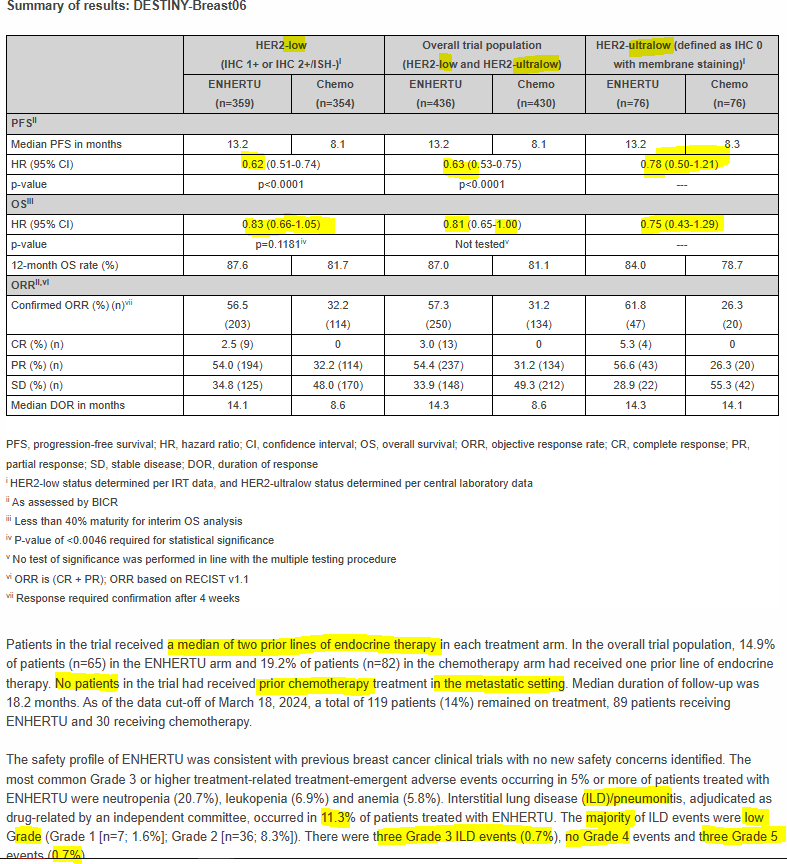
T-DXd demonstrated a statistically significant improvement in PFS versus chemotherapy. In the HER2-low population (primary endpoint), median PFS was 13.2 months with T-DXd versus 8.1 months with chemotherapy (HR 0.62; 95% CI: 0.52-0.75; p<0.0001), representing a 38% reduction in the risk of disease progression or death. In the overall ITT population, median PFS was 13.2 vs 8.1 months (HR 0.64; 95% CI: 0.54-0.76; p<0.0001). Confirmed ORR by BICR was 57.3% with T-DXd versus 31.2% with chemotherapy in the ITT population.
At the time of PFS final analysis (data cutoff March 18, 2024), OS data were immature with approximately 39% of events (335 deaths across both arms in the ITT population). Interim 12-month OS rates in the ITT population were 87.0% with T-DXd versus 81.1% with chemotherapy (HR 0.81; 95% CI: 0.65-1.00). Of note, 17.9% of patients in the chemotherapy arm received T-DXd after treatment discontinuation, which may confound OS analysis. Mature OS data are pending.
The safety profile was consistent with prior T-DXd trials. Grade 3 or higher treatment-related AEs occurred in 40.6% of T-DXd patients versus 31.4% with chemotherapy, though median treatment duration was nearly twice as long (11.0 vs 5.6 months). The most common grade 3+ AEs with T-DXd were neutropenia (20.7%), leukopenia (6.9%), and anemia (5.8%). ILD/pneumonitis occurred in 11.3% of T-DXd patients (Grade 1: 1.6%, Grade 2: 8.3%, Grade 3: 0.7%, Grade 4: 0%, Grade 5: 0.7% [3 fatal events]). Any-grade nausea occurred in 65.9%. AE-associated treatment discontinuation was 14.3% vs 9.4%. LVEF decrease was observed in 8.1% with T-DXd (mostly Grade 2) vs 2.9% with chemotherapy, but no cardiac failure occurred with T-DXd.
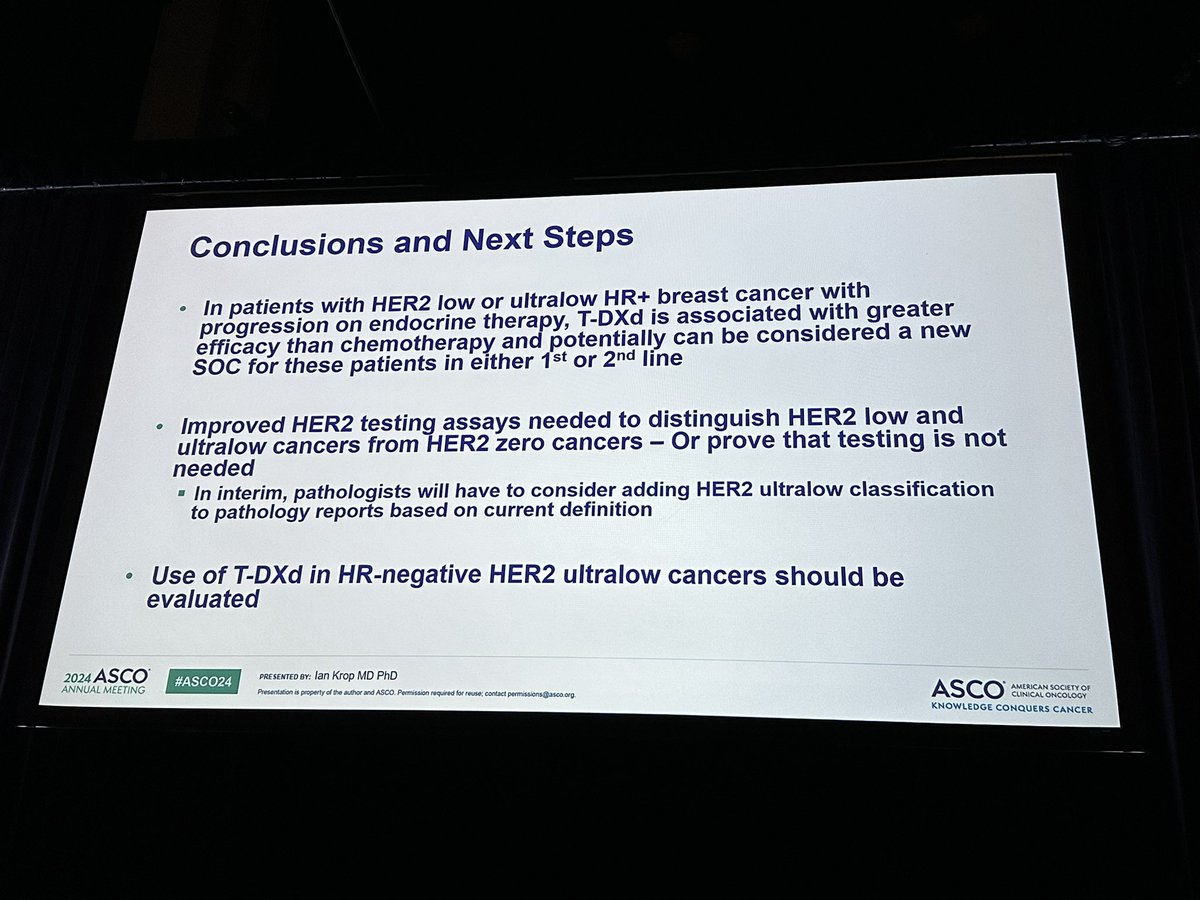
DESTINY-Breast06 establishes T-DXd as a new standard of care for HR-positive, HER2-low and HER2-ultralow metastatic breast cancer following endocrine therapy progression, prior to chemotherapy. The trial fundamentally redefines HER2 classification by establishing the HER2-ultralow category (IHC 0 with membrane staining), requiring pathologists to distinguish faint membrane staining from truly absent staining. Key clinical debates include: (1) optimal patient selection given ILD toxicity risk, with some experts advocating gentler oral agents first for less symptomatic patients; (2) the need for improved HER2 testing assays and retesting of IHC 0 tumors; (3) sequencing of multiple ADCs (T-DXd, sacituzumab govitecan, datopotamab deruxtecan) given potential cross-resistance via shared topoisomerase I payloads; and (4) pending mature OS data to confirm the PFS benefit translates to survival gain. The prospective TRADE-DXd trial (NCT06533826) is investigating optimal ADC sequencing.
DESTINY-Breast06 is a Phase 3, randomized, open-label trial (NCT04494425) that randomized 866 patients (713 HER2-low, 153 HER2-ultralow) with HR-positive metastatic breast cancer after progression on endocrine therapy to trastuzumab deruxtecan (T-DXd, Enhertu) versus physician's-choice chemotherapy.
Yes. On January 27, 2025 the FDA approved Enhertu for unresectable or metastatic HR-positive, HER2-low (IHC 1+ or 2+/ISH-) or HER2-ultralow (IHC 0 with membrane staining) breast cancer that has progressed on prior endocrine therapy, based on DESTINY-Breast06.
In the HER2-low population (the primary endpoint), median progression-free survival was 13.2 months with T-DXd versus 8.1 months with chemotherapy (HR 0.62; 95% CI 0.52-0.75; p<0.0001).
It was the first trial to demonstrate efficacy of a HER2-directed therapy in the HER2-ultralow population (IHC 0 with membrane staining), extending the population of HR+ metastatic breast cancer patients who may benefit from T-DXd after endocrine therapy.
Trastuzumab deruxtecan (T-DXd, Enhertu) is a HER2-directed antibody-drug conjugate developed by Daiichi Sankyo and AstraZeneca.