NSCLC brain metastases - Novocure
Discover KOL Sentiment on METIS →













Top 10 by impressions - click to view on X
#ASCO24 Lung cancer is not just invading the plenaries...but other tracks as well! Looking forward to discussing 2 NSCLC abstracts in the CNS orals: - High-dose almonertinib in...
#ASCO24 Lung cancer is not just invading the plenaries...but other tracks as well! Looking forward to discussing 2 NSCLC abstracts in the CNS orals: - High-dose almonertinib in...
The chair of the @NRGonc Brain Tumor Scientific Core Committee, legendary #RadOnc Dr. Minesh Mehta presenting the Phase 3 METIS RCT at #ASCO24: for...
The chair of the @NRGonc Brain Tumor Scientific Core Committee, legendary #RadOnc Dr. Minesh Mehta presenting the Phase 3 METIS RCT at #ASCO24: for...
Dr. Minesh Mehta, Miami Cancer Institute, presents global phase III MÉTIS trial results at @ASCO #ASCO24 showing impressive efficacy with TTF against brain metastases from...
Data from our positive phase 3 METIS clinical trial, which investigated the use of Tumor Treating Fields therapy in the treatment of brain metastases from non-small cell lung cancer, will be...
@DrJNaidoo @ASCO @CancerCentreIre @FordePatrick @gerryhanna @JulieBrahmer @HendriksLizza @Alfdoc2 @JordiRemon...
💥 New options for #NSCLC with 🧠 Mets - ACHIEVE trial--> 💊 Almonertinib 165mg QD ✅ mPFS 20.5m, 🧠PFS NR ✅ ORR 88.9% - METIS trial--> TTFields +BSC pts...
💥 New options for #NSCLC with 🧠 Mets - ACHIEVE trial--> 💊 Almonertinib 165mg QD ✅ mPFS 20.5m, 🧠PFS NR ✅ ORR 88.9% - METIS trial--> TTFields +BSC pts...

💡Don’t miss Dr. Minesh Mehta’s oral with results from the phase 3 #METIS trial highlighting the effectiveness of TTFields therapy for #NSCLC 👇...
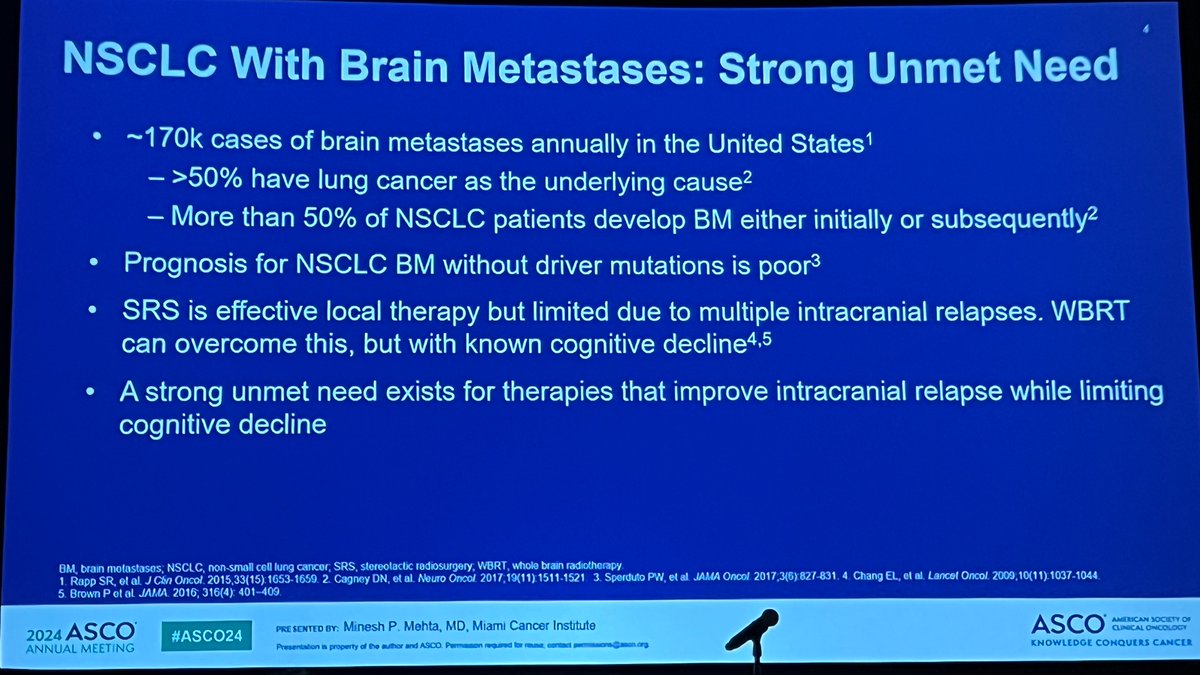
METIS is a pivotal Phase 3, randomized, controlled trial evaluating Tumor Treating Fields (TTFields) therapy combined with best supportive care (BSC) versus BSC alone for patients with 1-10 newly diagnosed brain metastases from NSCLC following stereotactic radiosurgery (SRS). The trial enrolled 298 adult patients across 78 sites in 13 countries and met its primary endpoint, demonstrating a statistically significant delay in time to intracranial progression. METIS is the first Phase 3 trial to show that TTFields therapy significantly delays intracranial progression in NSCLC brain metastases without adding systemic toxicity or neurocognitive side effects.
Phase 3, international, open-label, 1:1 randomized trial in adults with 1-10 newly diagnosed brain metastases from NSCLC post-SRS. TTFields therapy delivered at 150kHz. Patients stratified by number of brain metastases (1-4 vs 5-10), prior systemic therapy, and tumor histology. Patients with known actionable tumor mutations were excluded. Crossover to TTFields permitted after confirmed second intracranial progression.
Adults with 1-10 newly diagnosed brain metastases from NSCLC who had undergone stereotactic radiosurgery. Both arms permitted continued systemic anti-cancer therapy for the primary NSCLC at the treating physician's discretion. Supportive care included steroids, anti-epileptic drugs, anticoagulants, and symptom management medications. Median age 63-64 years, majority male, most with adenocarcinoma histology and Karnofsky PS 80+.
TTFields therapy at 150kHz combined with best supportive care (n=149) versus best supportive care alone (n=149), both following stereotactic radiosurgery of brain metastases. Treatment continued until disease progression or unacceptable toxicity. Median TTFields therapy duration was 16 weeks with median usage of 67%.
Primary endpoint: time to first intracranial progression (TTIP) measured from first SRS to intracranial progression (RANO-BM criteria) or neurological death. Secondary endpoints: time to distant intracranial progression, time to neurocognitive failure, overall survival, radiological response rate (MRI), time to second intracranial progression, quality of life, and adverse events.
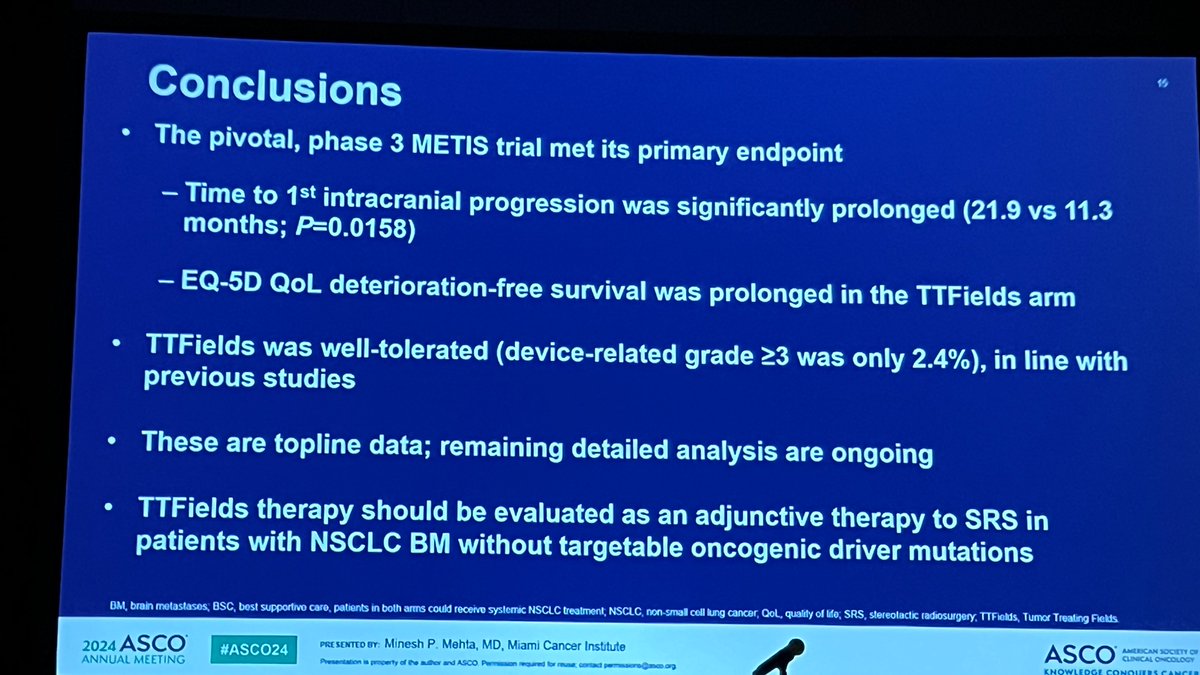
METIS met its primary endpoint. Initial data (ASCO 2024): median TTIP was 21.9 months with TTFields + BSC vs 11.3 months with BSC alone (HR 0.67; p=0.016). Final results (ASTRO 2025): using Fine-Gray competing risks model, HR was 0.72 (95% CI: 0.53-0.98; p=0.044), representing a 28% relative risk reduction. Median TTIP was 15.0 months vs 7.5 months. In the subgroup receiving immune checkpoint inhibitors (n=118), the benefit was more pronounced: TTIP HR 0.63, distant intracranial progression HR 0.41.
At final analysis, there was no significant difference in overall survival between the TTFields and control arms. Median OS was 11.3 months (95% CI: 8.6-13.8) with TTFields vs 10.6 months (95% CI: 6.8-14.1) with BSC alone (HR 1.04; 95% CI: 0.76-1.43; p=0.763). Radiographic response rate was also not significantly different: 49.0% (95% CI: 38.6%-59.4%) vs 46.0% (95% CI: 37.0%-55.2%; p=0.659). Time to neurocognitive failure was similar between arms.
TTFields therapy was well-tolerated with no additive systemic toxicity. Grade 1/2 skin issues were the most common device-related adverse events, with device-related AEs occurring in 50.4% of patients. Grade 3+ AEs occurred in 32.6% of TTFields patients vs 29.1% in the control arm. Device-related Grade 3+ AEs were rare at only 1.6%. Device discontinuation due to AEs occurred in 5.4% of patients. One death was reported among device-related serious AEs (1.6%). Importantly, TTFields did not cause quality of life deterioration and showed improvements in deterioration-free survival.
METIS establishes TTFields as the first device-based therapy to demonstrate a statistically significant delay in intracranial progression for NSCLC brain metastases after SRS, without adding systemic toxicity or neurocognitive impairment. The combination with immune checkpoint inhibitors showed enhanced intracranial benefit (HR 0.63 for TTIP, HR 0.41 for distant intracranial progression), suggesting a potential synergy worth further investigation. Key clinical debates include the lack of OS benefit, the device compliance burden (median usage 67%, median duration 16 weeks), the cost and quality-of-life impact of wearing the device, and whether TTFields should be integrated into routine post-SRS management. Novocure planned FDA premarket approval application submission following the ASTRO 2025 presentation.




