IsKia is a Phase 3 trial testing whether adding isatuximab (Sarclisa) to carfilzomib, lenalidomide and dexamethasone (Isa-KRd) deepens responses versus KRd as pre- and post-transplant therapy in transplant-eligible newly diagnosed multiple myeloma. Isa-KRd met its primary endpoint, raising post-consolidation MRD-negativity (NGS 10^-5) to 77% vs 67% (p=0.049). The frontline Isa-KRd regimen is investigational. Sponsor: European Myeloma Network / Sanofi.
Discover KOL Sentiment on IsKia →Design — Phase 3, randomized (1:1), multicenter; Isa-KRd vs KRd across induction -> ASCT (MEL200) -> full-dose + light consolidation, transplant-eligible NDMM (<70 yr), n=302 across 42 sites (NCT04483739). (ASH 2023, Gay et al.)
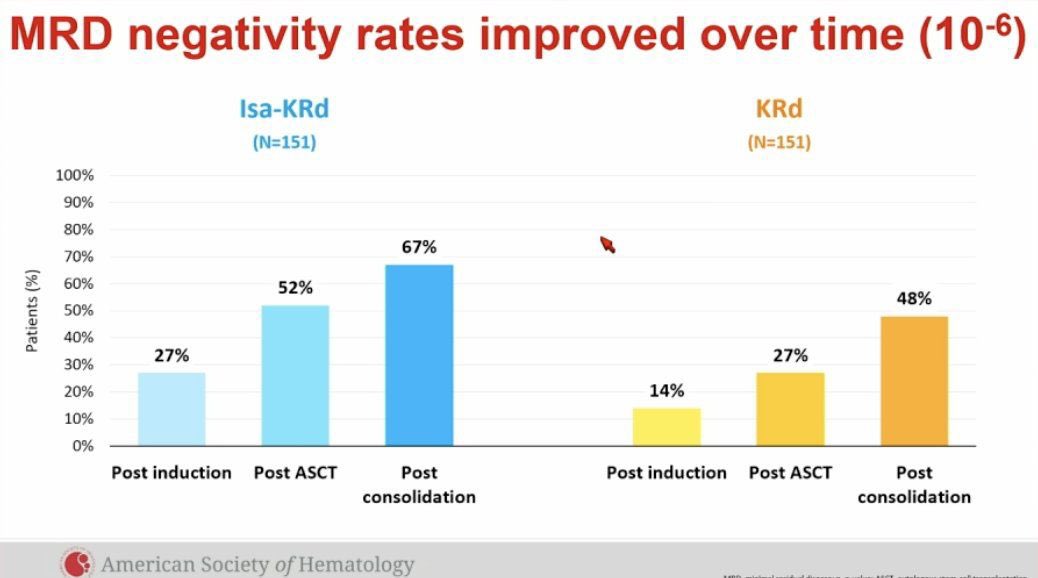
MRD-negativity (primary, NGS 10^-5) — MET — post-consolidation 77% (Isa-KRd) vs 67% (KRd); OR 1.67; p=0.049. At 10^-6: 67% vs 48% (OR 2.29; p<0.001). (ASH 2023)
Deepening / sustained MRD — Post-induction 45% vs 26% and post-ASCT 64% vs 49% (10^-5) (ASH 2023); 1-year sustained MRD-neg (10^-6) 52% vs 38%, and in very-high-risk (>=2 HRCAs) 62% vs 20% (ASCO 2025, JCO 7502).
PFS / OS — Immature at primary analysis (median follow-up ~35 months); longer follow-up needed to link deep MRD-negativity to survival. (ASH 2023)
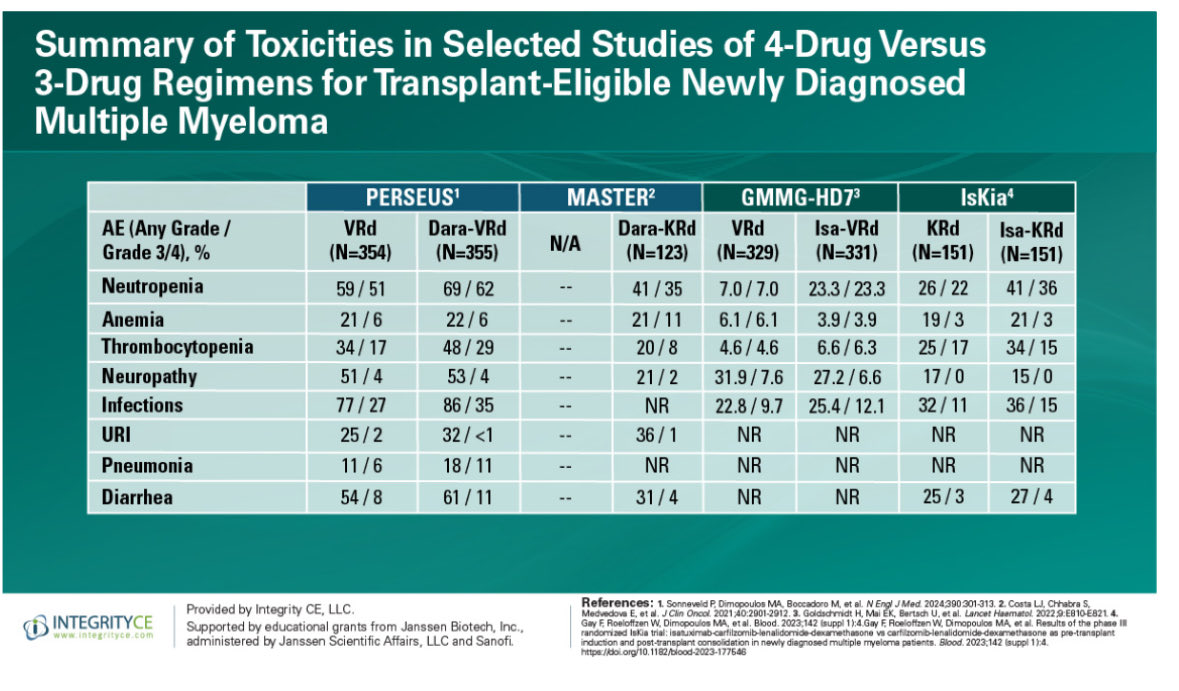
Safety — Grade 3/4 neutropenia 36% vs 22% (p=0.008); any-grade infusion reactions 20% vs 1%; treatment discontinuation 17% vs 10%; 4 vs 1 deaths (3 infection-related). (ASH 2023)
Regulatory — INVESTIGATIONAL — frontline transplant-eligible Isa-KRd is NOT FDA approved. Isatuximab (Sarclisa) is approved in R/R MM and, per IMROZ, in transplant-ineligible NDMM (Isa-VRd). (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.






















Top 10 by impressions - click to view on X
My thoughts while attending the plenary session of Isa-KRd versus KRD: Appreciation/respect for investigators involved, while still feeling shame that the best my beloved subspecialty can bring to...
My thoughts while attending the plenary session of Isa-KRd versus KRD: Appreciation/respect for investigators involved, while still feeling shame that the best my beloved subspecialty can bring to...
IsKia the way to go? MRD as the primary endpoint: 1️⃣ precludes reg approval for isakrd - maybe IMROZ will get Isa into frontline? 2️⃣ sets the stage for understanding how change in MRD corresponds...
🔥🔥 Tune in for our #ASH23 #Myeloma recap with @bdermanmd! We discuss: PERSEUS ISKIA GMMG ReLApsE KarMMa-3 OS data @iStopMM serum FLC ratio...
#ASH23 plenary abstract on the Iskia trial presented by Dr. Gay: Not without bumps on the road and still a long way to the finish line, but I find fascinating to see how MRD has...

ITT✅, MRD@each phase✅, Analytically validated assay✅, "first pull"✅. IsKia is a model, aligned with international harmonization 👏🏼👏🏼👏🏼 #ASH23...

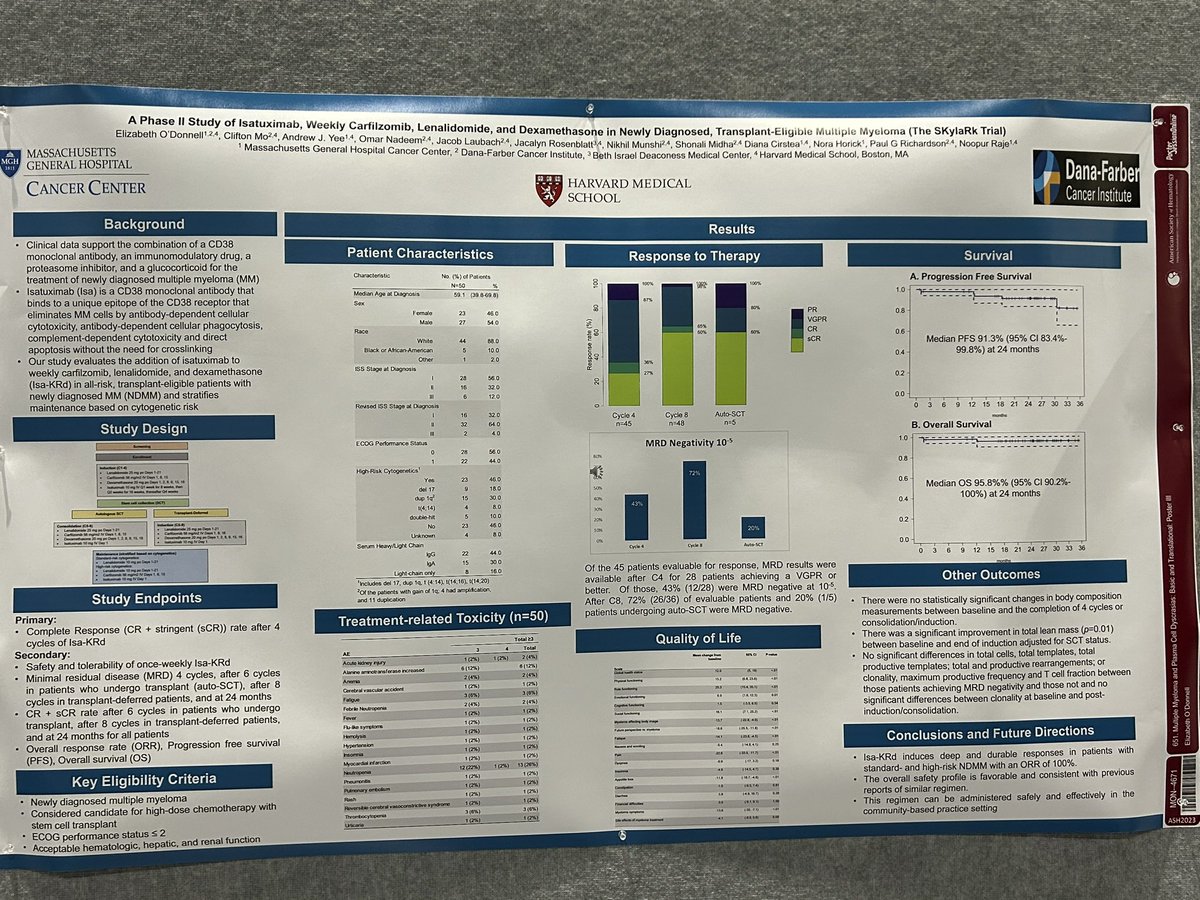
#ASH23 Dont forget to checkout the younger, American sister to the #Plenary Iskia study! The SkyLark study, Isa-KRD in TE NDMM presented by @betsyodonnellmd...

AEs & QOL Key takeaway: manageable AE profiles w/ quads → preserved QOL Safety analysis: Tolerable AE profiles support use of upfront quad tx for appropriate pts w/ TE NDMM NCCN...

IsKia EMN24 study plenary presented by Dr Francesca Gay Phase 3 trial with IsaKRd vs KRd shows higher post consolidation MRD negativity rates with excellent introduction by @PlasmaCellPete...

@ManniMD1 Yet there is a lot to learn from nuances of ISKIA/EMN24. Just two quick (premature example): 1) do ISS 1 patients really need a quardruplet (MRD HR ratios were pretty close to 1 in...
IsKia is a Phase III, randomized trial evaluating the addition of isatuximab (Sarclisa) to carfilzomib, lenalidomide, and dexamethasone (Isa-KRd) versus KRd alone as pre-transplant induction and post-transplant consolidation in transplant-eligible patients with newly diagnosed multiple myeloma. The trial enrolled 302 patients across 42 sites and demonstrated that the Isa-KRd quadruplet significantly increased MRD negativity rates at both 10-5 and 10-6 thresholds, with the benefit retained across all subgroups including high-risk and very high-risk patients.
Phase III, randomized, multicenter trial (NCT04483739). Patients randomized 1:1 to Isa-KRd or KRd. Four phases: (1) Induction: 4 cycles of Isa-KRd or KRd; (2) Mobilization + MEL200 + ASCT; (3) Full-dose consolidation: 4 cycles; (4) Light consolidation: 12 cycles with reduced dosing. Isatuximab 10 mg/kg IV on days 1, 8, 15, 22 cycle 1, then days 1, 15 cycles 2-4 (induction/consolidation), days 1, 15 (light consolidation). Carfilzomib 20/56 mg/m2, lenalidomide 25 mg (full-dose) or 10 mg (light), dexamethasone 40 mg (full-dose) or 20 mg (light). Stratified by centralized FISH cytogenetic risk.
Transplant-eligible adults under 70 years of age with newly diagnosed multiple myeloma (stages I-IV). 43% vs 41% had R2-ISS stage III/IV disease; 9% vs 11% had 2 or more high-risk cytogenetic abnormalities (del(17p), t(4;14), t(14;16), 1q+). Median age 61 (Isa-KRd) and 60 (KRd). Written informed consent required.
Arm A: Isatuximab + carfilzomib + lenalidomide + dexamethasone (Isa-KRd) through induction, ASCT, full-dose consolidation, and light consolidation. Arm B: Carfilzomib + lenalidomide + dexamethasone (KRd) alone through all phases. 83% of Isa-KRd patients completed induction and consolidation vs 90% of KRd.
Primary endpoint: MRD negativity rate by NGS at 10-5 threshold after post-ASCT full-dose consolidation. Key secondary endpoints: MRD negativity after induction, PFS, overall response rate, duration of response, 1-year sustained MRD negativity, OS, and safety.
The primary endpoint was met: post-consolidation MRD negativity (10-5) was 77% for Isa-KRd vs 67% for KRd (OR 1.67; p=0.049). At the stricter 10-6 threshold: 67% vs 48% (OR 2.29; p<0.001). MRD negativity improved over treatment phases: post-induction 45% vs 26% (10-5, OR 2.34; p<0.001), post-ASCT 64% vs 49% (10-5, OR 1.93; p=0.006). 1-year sustained MRD negativity (10-6): 52% vs 38% (OR 1.82; p=0.012). In very high-risk patients (2+ HRCAs), 1-year sustained MRD (10-6) was 62% vs 20% (OR 6.3). Post-consolidation response: VGPR or better 94% in both arms; CR or better 74% vs 72%; sCR 64% vs 67%.
PFS and OS data are not yet mature due to relatively short median follow-up (35 months at latest data cut). A meta-analysis of isatuximab regimens in NDMM reported an overall 34% reduction in progression or death risk (HR 0.66; 95% CI 0.52-0.84; p=0.001). Longer follow-up is needed to establish the correlation between the deep MRD negativity achieved and survival outcomes.
Any-grade hematologic toxicity: 55% (Isa-KRd) vs 44% (KRd). Neutropenia: 41% vs 26% any-grade; 36% vs 22% G3/4 (p=0.008). Thrombocytopenia: 34% vs 25% any-grade; 15% vs 17% G3/4. Non-hematologic toxicity: 90% vs 85% any-grade. Infusion reactions: 20% vs 1% any-grade; 3% vs 0% G3/4. Infections (excl. COVID): 36% vs 32% any-grade; 15% vs 11% G3/4. COVID-19: 26% vs 19%. Cardiac disorders: 7% vs 13% (lower with Isa-KRd). Treatment discontinuation: 17% vs 10% overall; 6% vs 5% due to AEs. Deaths: 4 (Isa-KRd) vs 1 (KRd), including 3 infection-related deaths in Isa-KRd. During light consolidation: 2 treatment-related deaths in Isa-KRd (pulmonary embolism, cerebral ischemia) vs 0 in KRd.
IsKia demonstrates that adding isatuximab to a carfilzomib-based quadruplet significantly deepens MRD responses in transplant-eligible NDMM, particularly at the stringent 10-6 threshold where the benefit was most pronounced (OR 2.29). The advantage was especially striking in very high-risk patients with 2+ HRCAs (62% vs 20% sustained MRD negativity). Isa-KRd is not FDA approved based on IsKia; isatuximab (Sarclisa) holds approvals in other settings (Isa-VRd for NDMM, Isa-Pd for RRMM). Key debates include whether anti-CD38 quadruplets should use daratumumab-VRd (PERSEUS/GRIFFIN) or isatuximab-KRd (IsKia), the carfilzomib vs bortezomib backbone question, whether 10-6 MRD negativity will translate to OS benefit, and feasibility of MRD-guided treatment discontinuation.
IsKia (also known as EMN24; NCT04483739) is a Phase 3, randomized, multicenter trial that enrolled 302 transplant-eligible adults under 70 with newly diagnosed multiple myeloma across 42 sites. It compares isatuximab plus carfilzomib, lenalidomide and dexamethasone (Isa-KRd) with KRd alone, given as pre-transplant induction and post-transplant consolidation.
IsKia met its primary endpoint. After post-transplant consolidation, minimal residual disease (MRD) negativity by next-generation sequencing at the 10^-5 threshold was 77% with Isa-KRd versus 67% with KRd (OR 1.67; p=0.049). At the deeper 10^-6 threshold, MRD-negativity was 67% versus 48% (OR 2.29; p<0.001).
No. The frontline transplant-eligible Isa-KRd regimen studied in IsKia is investigational and not FDA approved. Isatuximab (Sarclisa) is FDA approved for relapsed/refractory multiple myeloma and, based on the IMROZ trial, with VRd for transplant-ineligible newly diagnosed myeloma — but not as Isa-KRd for transplant-eligible patients.
Yes. The improvement in MRD-negativity with Isa-KRd was retained across subgroups, including high-risk and very-high-risk disease. Among very-high-risk patients (2 or more high-risk cytogenetic abnormalities), 1-year sustained MRD-negativity at 10^-6 was 62% with Isa-KRd versus 20% with KRd.
Isa-KRd added hematologic and infusion-related toxicity: Grade 3/4 neutropenia occurred in 36% versus 22% (p=0.008) and any-grade infusion reactions in 20% versus 1%. Treatment discontinuation was 17% versus 10%, and there were 4 versus 1 deaths (including three infection-related deaths). PFS and OS were immature at the primary analysis.
































