Resectable gastric cancer (preoperative-only regimen selection) — Dutch investigator-initiated cooperative group (16 Netherlands centers)
Discover KOL Sentiment on CRITICS-II →Design - Randomized Phase 2 pick-the-winner: preoperative chemotherapy alone vs chemotherapy + chemoradiotherapy vs chemoradiotherapy alone, resectable gastric cancer, 16 Dutch centers (NCT02931890); primary 1-year event-free survival.
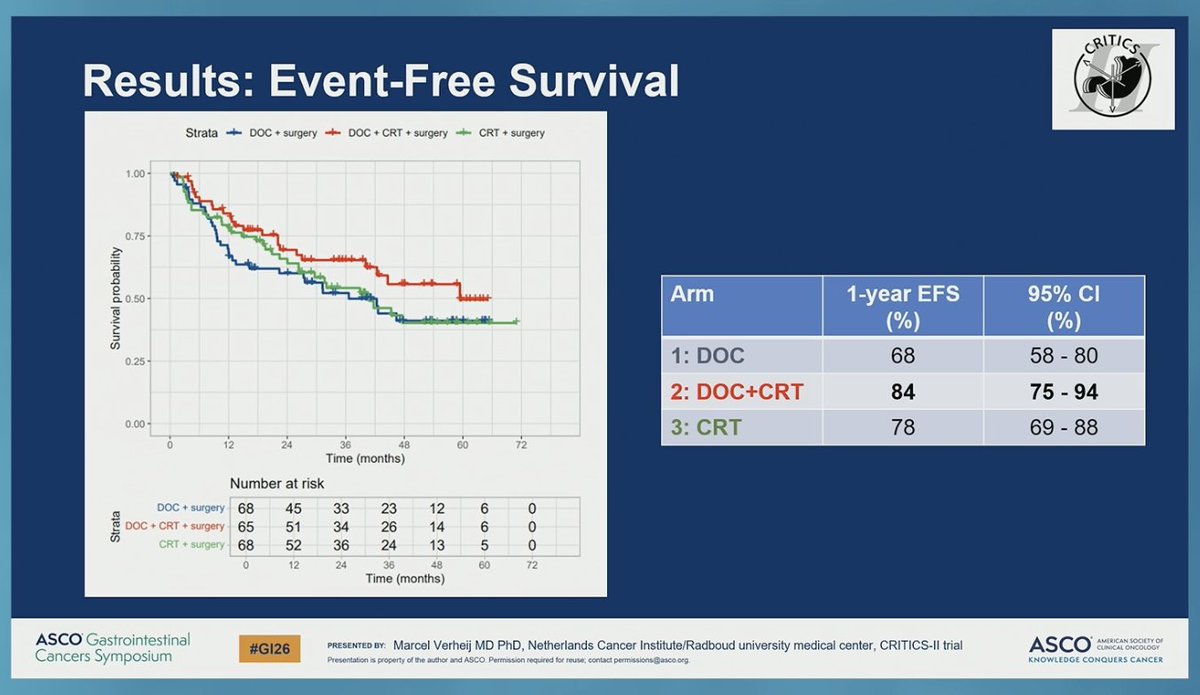
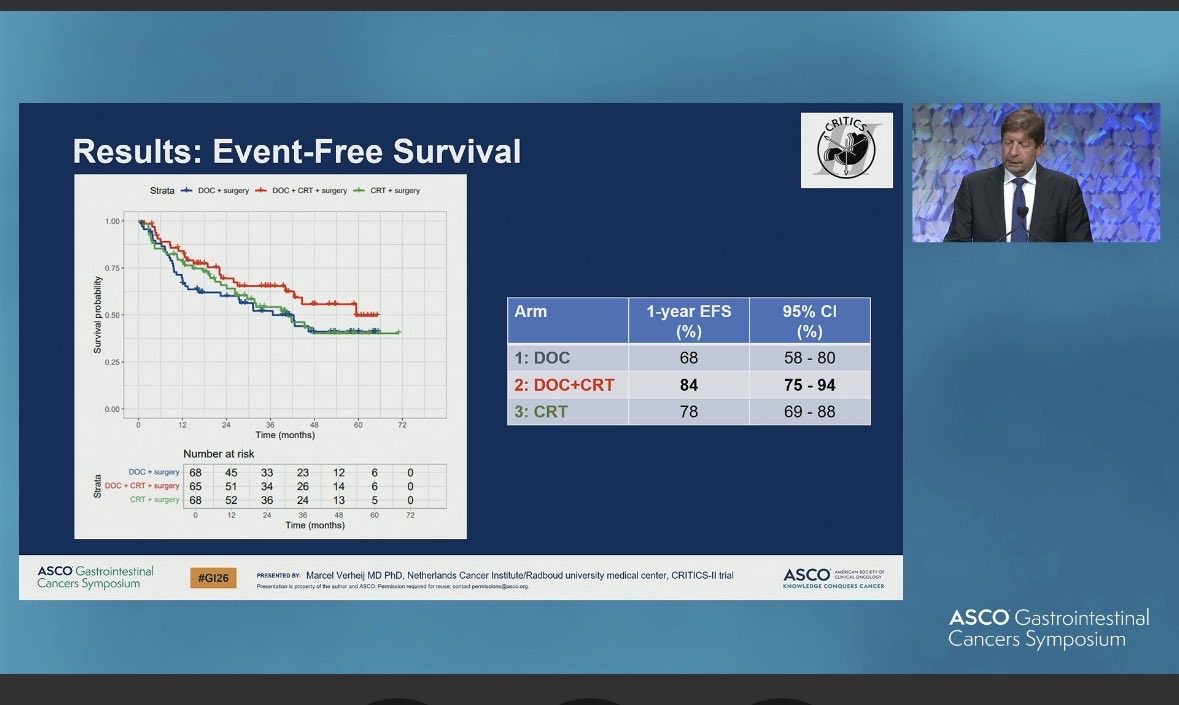
1-yr EFS (primary) - Chemotherapy alone 68% (below the 75% threshold); chemotherapy + chemoradiotherapy 84%; chemoradiotherapy alone 78%. Winner = chemotherapy + chemoradiotherapy (median follow-up 40.4 months).
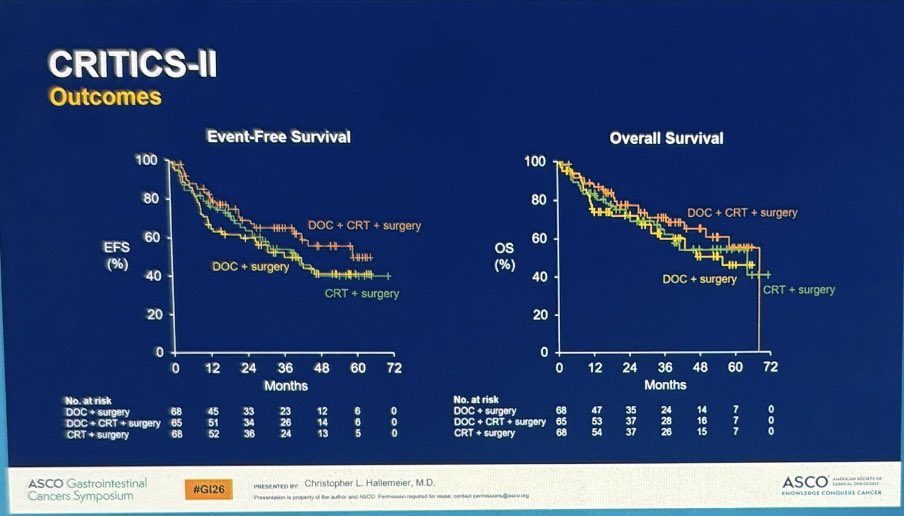
1-yr OS - Chemotherapy alone 74%; chemotherapy + chemoradiotherapy 89%; chemoradiotherapy alone 84% (design not powered for a formal OS comparison).
Interpretation - Phase 2 pick-the-winner selects a regimen for Phase 3 - it informs trial design, not current practice; re-focuses attention on preoperative chemoradiotherapy after the negative CRITICS-I Phase 3.
Regulatory - Investigational / academic - no FDA action; not practice-defining.
Sponsor - Netherlands Cancer Institute (investigator-initiated cooperative group).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.














Top tweets by impressions — click to view on X
🚨 Resectable Gastric Cancer | #GI26
CRITICS-II answers a key question
What is the best preoperative strategy when adjuvant therapy is omitted?
🧪 Trial design
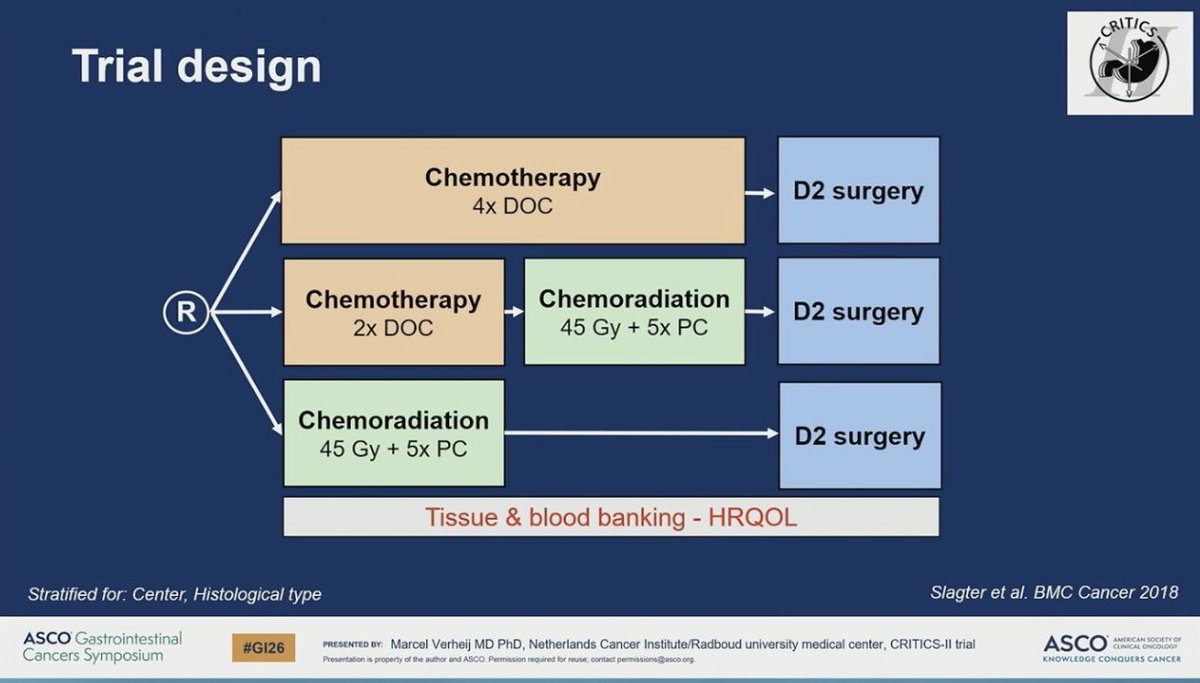
Three fully neoadjuvant approaches…
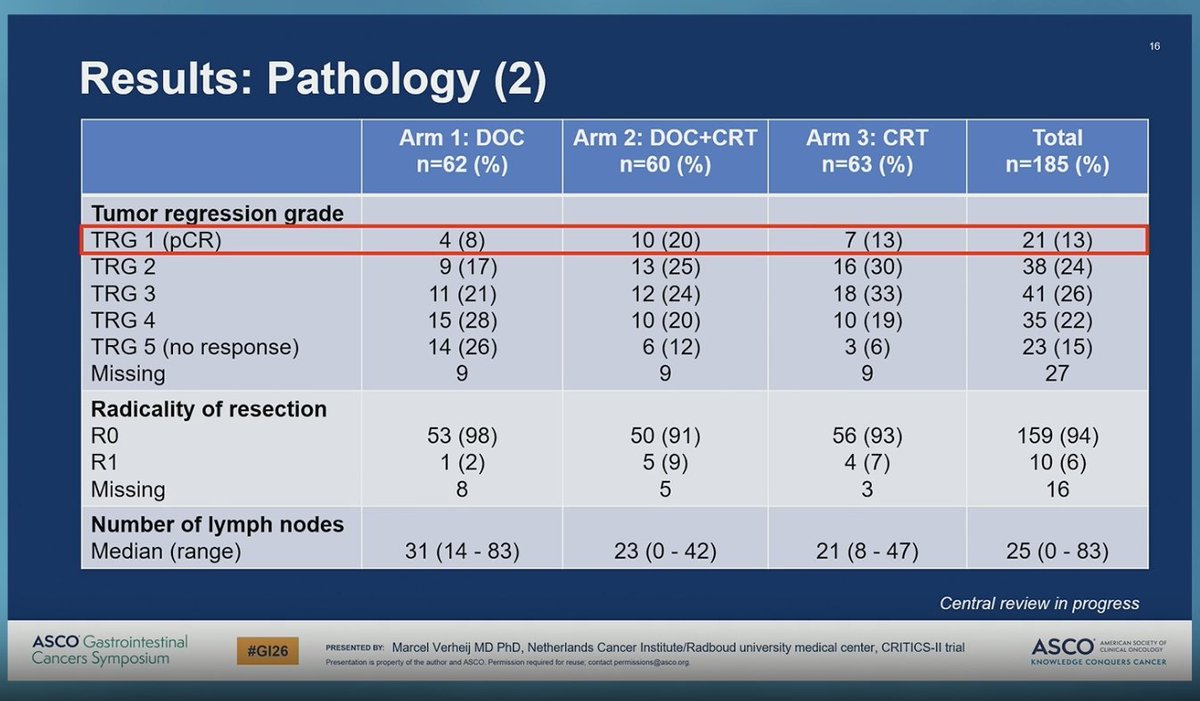
CRITICS-II: multicenter Ph2 RCT in resectable gastric ca showing preop chemo (DOC) + CRT improved 1-yr EFS & pCR (20%) v CRT or chemo alone. But w D-FLOT now SOC, q’s are:
1. Could adding…
📊 CRITICS-II at #ASCOGI26
Total neoadjuvant therapy wins the pre-op race in resectable gastric cancer 🍽️🩺
3 strategies tested head-to-head
🧪 Chemo alone
🔥 Chemoradiation alone
🚀 Chemo ➜…
Here is a great trial already in progress building off MATTERHORN & CRITICS-II (presented today)!
Japanese EPOC2031 Ph2: TNT for resectable GEJ
-FLOT + pembro + short course RT (25 Gy/5fx)
-1…
CRITICS - II: TNT for Gastric Cancer?! When do we consider chemorads #ASCOGI26 #GI26 https://t.co/bXjddANLlC
#GI26 CRITICS-II (phase II) | Resectable GC
🔀 3 neoadj strategies tested (no adj therapy):
• CT alone (failed EFS threshold)
• CT → CRT (TNT)
• CRT alone
📈 1-yr EFS: 84% (CT+CRT) vs 78% (CRT) vs 68%…
Dr. Hallemeier excellent discussion on CRITICS-II vs TOPGEAR, noting differences in absence of IO & periop vs TNT approaches between studies including study heterogeneity. Important for further…
Dr. Verheij CRITICS-II rand PhII pick-the-winner neoadj tx strategies in resectable #GC/GEJC ➡️ total neoadjuvant chemo + chemoRT w/best outcomes & preferred candidate for further study, notably…
CRITICS-II: Phase II trial of neo-adjuvant CTx vs neo-adjuvant CTx and subsequent CTR vs neo-adjuvant chemoradiotherapy followed by surgery in resectable GC
#ASCOGI26
👉 Arm1: lowest efficacy
👉…

#ASCOGI26 | CRITICS-II (Abstract 283)
Can we finally solve the post-op drop-out problem in gastric cancer?
Total neoadjuvant therapy (chemo → chemoradiotherapy → surgery) shows higher 1-year EFS…
Phase 2 'pick-the-winner' trial — CT + CRT arm selected for phase 3 evaluation in resectable gastric cancer. Shifts attention back to preoperative chemoradiotherapy after CRITICS-I (phase 3) showed no benefit for postoperative CRT. Does not change current practice but informs phase 3 design.
Three-arm pick-the-winner design comparing preoperative regimens. CT alone: 1-yr EFS 68% (below 75% threshold). CT + CRT: 1-yr EFS 84%. CRT alone: 1-yr EFS 78%. Winner = CT + CRT based on EFS, OS, surgical outcomes, and pCR. Median follow-up 40.4 months.
1-year OS rates: CT alone 74%, CT+CRT 89%, CRT alone 84%. Pick-the-winner design — not powered for formal OS comparison between arms.
Preoperative regimen safety profile detailed in primary publication. Pick-the-winner design focuses on 1-year EFS landmark rather than extensive toxicity comparison.
⚠️ Phase 2 pick-the-winner — informs phase 3 design, not current practice. Phase 2 'pick-the-winner' trial — CT + CRT arm selected for phase 3 evaluation in resectable gastric cancer. Shifts attention back to preoperative chemoradiotherapy after CRITICS-I (phase 3) showed no benefit for postoperative CRT. Does not change current practice but informs phase 3 design.
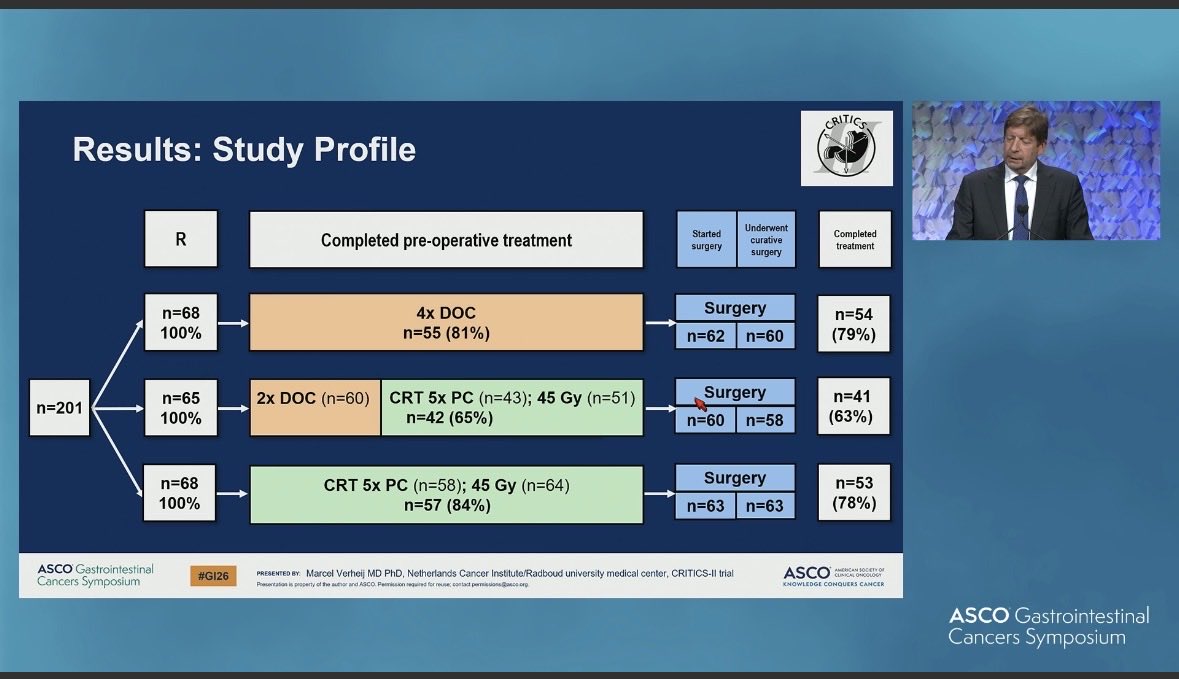
CRITICS-II is a randomized Phase 2 'pick-the-winner' strategy trial (NCT02931890) run across 16 Dutch centers, comparing three preoperative regimens in resectable gastric cancer: chemotherapy alone, chemotherapy plus chemoradiotherapy, and chemoradiotherapy alone. The primary endpoint was 1-year event-free survival, used to select one regimen to advance to Phase 3.
One-year event-free survival was 68% with chemotherapy alone (below the pre-specified 75% threshold), 84% with chemotherapy plus chemoradiotherapy, and 78% with chemoradiotherapy alone. One-year overall survival rates were 74%, 89%, and 84%, respectively. Based on event-free survival, overall survival, surgical outcomes, and pathologic complete response, the chemotherapy-plus-chemoradiotherapy arm was selected as the winner (median follow-up 40.4 months).
No. CRITICS-II is a Phase 2 pick-the-winner design intended to select the most promising preoperative regimen for a subsequent Phase 3 trial - it informs trial design rather than defining current standard of care. It does not test or approve any new drug and did not involve an FDA action.
The earlier CRITICS-I Phase 3 trial showed no benefit from adding postoperative chemoradiotherapy to perioperative chemotherapy. CRITICS-II shifts the question to the preoperative setting, and its selection of the chemotherapy-plus-chemoradiotherapy arm renews interest in delivering chemoradiotherapy before surgery in resectable gastric cancer.
CRITICS-II enrolled patients with resectable gastric cancer eligible for preoperative therapy and curative-intent surgery. Because it is a strategy trial, patients were randomized among three preoperative regimen approaches rather than to a single novel agent, and the focus was on identifying the optimal preoperative strategy to carry forward.