1L HR+/HER2- mBC (GBG, Germany) - Pfizer
Discover KOL Sentiment on PADMA →Design - Randomized Phase IV German Breast Group trial: first-line palbociclib (Ibrance) + endocrine therapy vs chemotherapy, HR+/HER2- metastatic breast cancer with a chemotherapy indication (NCT03355157).
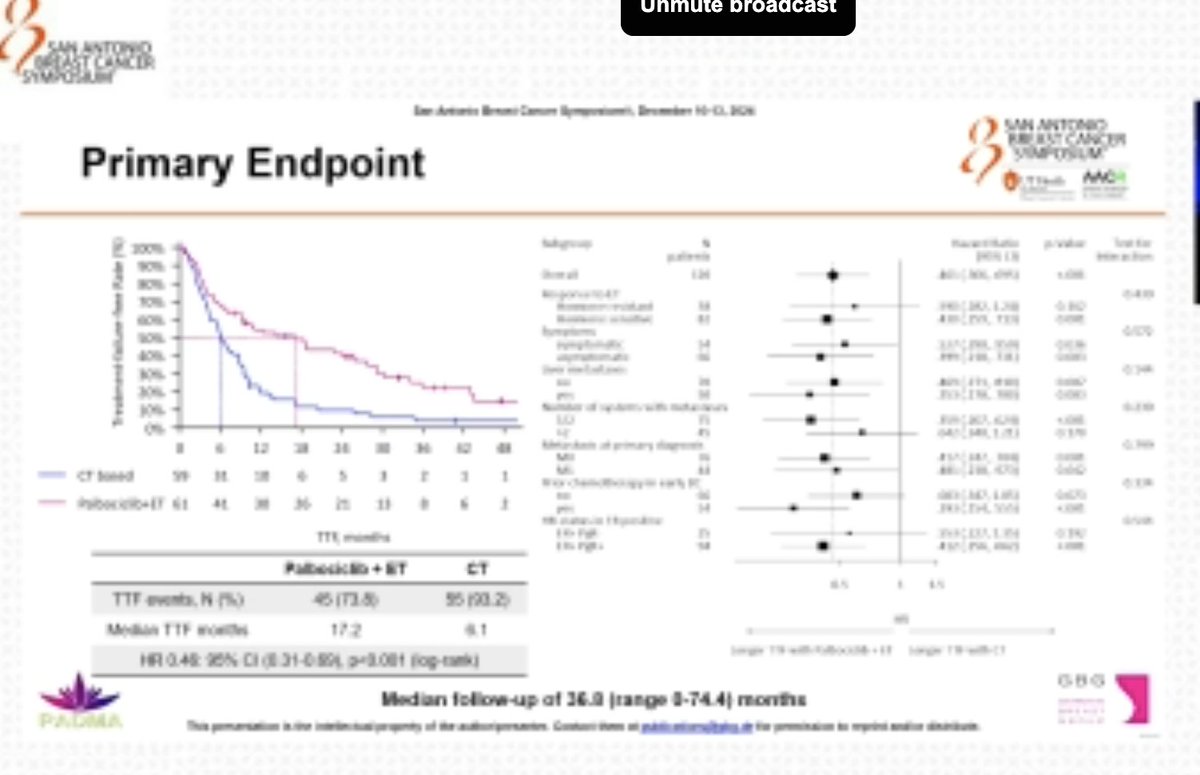
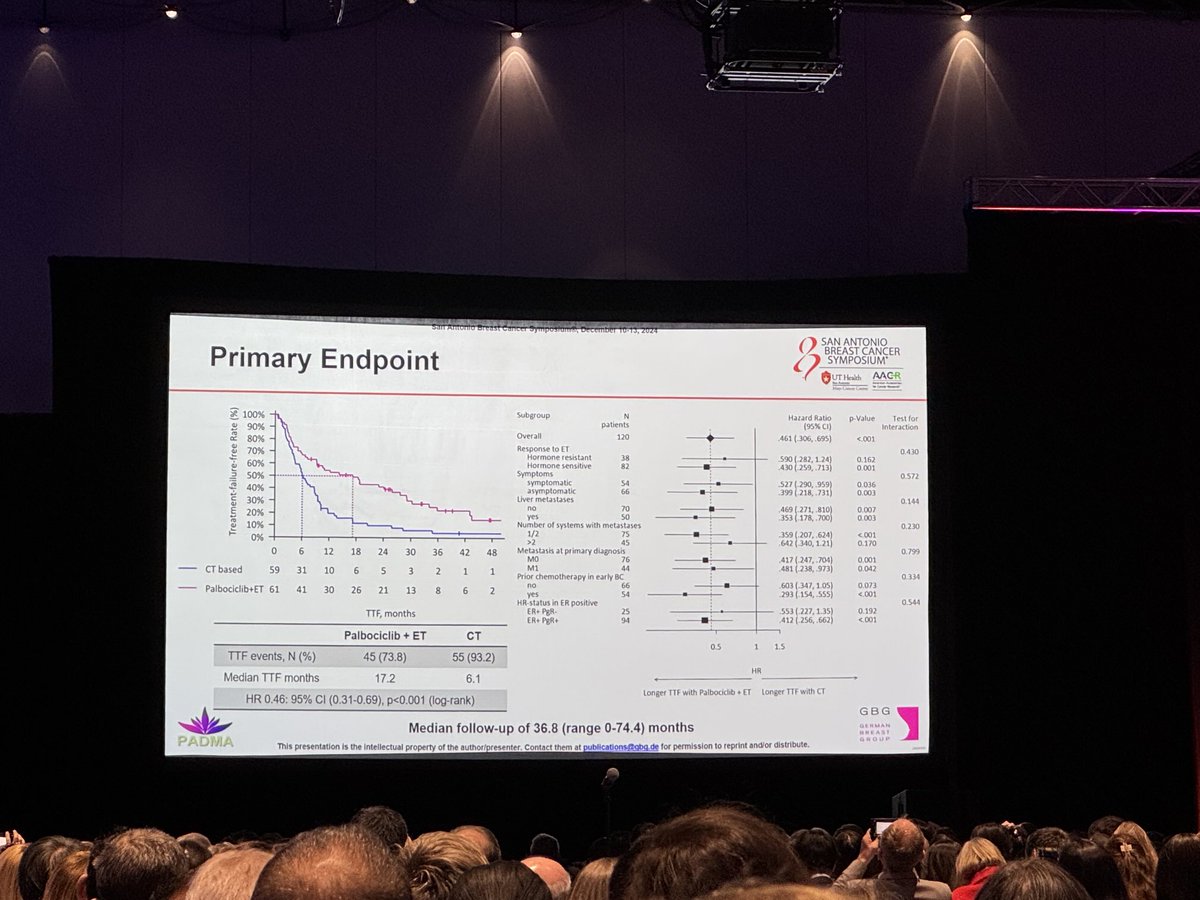
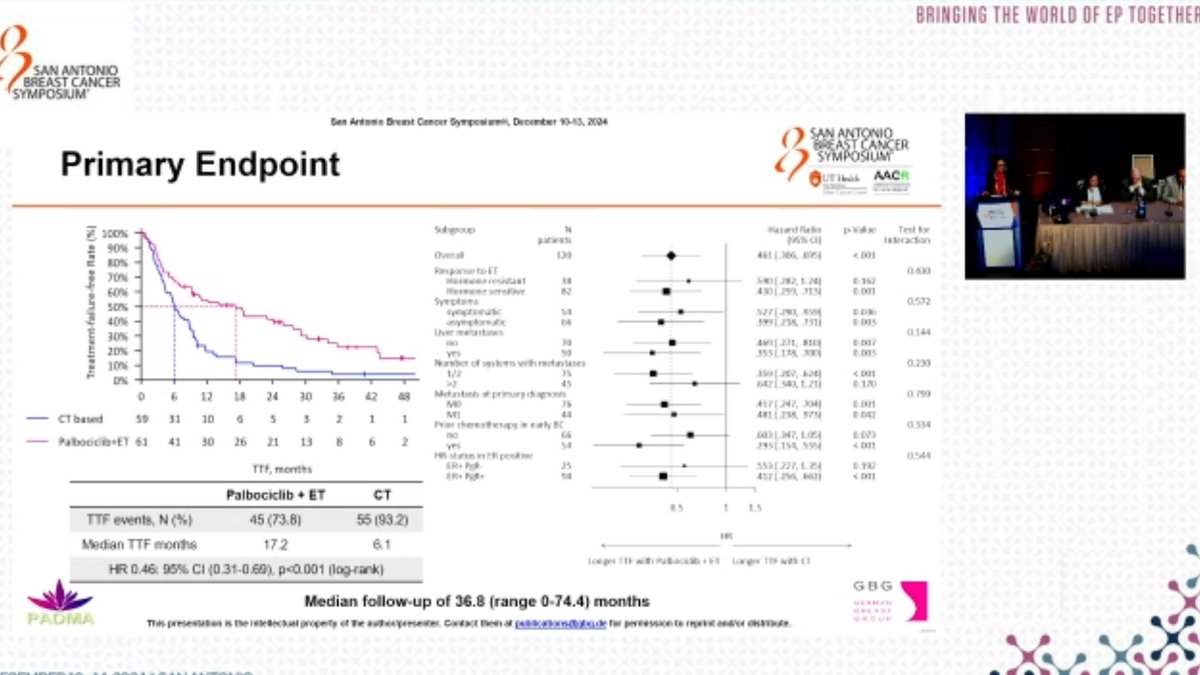
PFS - Median 18.7 vs 7.8 months, HR 0.45 (95% CI 0.29-0.70; p<0.001) favoring palbociclib + endocrine therapy; time to treatment failure 17.2 vs 6.1 months (HR 0.46).
OS - Numerical trend favoring palbociclib + endocrine therapy but not statistically significant: median 46.1 vs 36.8 months (HR 0.81; 95% CI 0.46-1.43; p=0.4630).
Safety - More hematologic toxicity with palbociclib (any-grade hematologic TRAEs 96.8% vs 58.6%; grade 3-4 54.8% vs 6.9%); non-hematologic AEs comparable.
Regulatory - Palbociclib (Ibrance) is FDA-approved with endocrine therapy in HR+/HER2- advanced/metastatic breast cancer; PADMA is an investigator-initiated comparative trial, not a new registration.
Sponsor / drug - German Breast Group (GBG); palbociclib (Ibrance) + endocrine therapy.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.











Top 10 by impressions - click to view on X
PADMA study: ET + palbo vs chemo (cape/taxane/navelbine) in high risk HR+ MBC--> confirms ET+ cdk4/6i is 1L SOC n=150 42% w/liver mets 6% BRCAm TTF: 17.2 vs 6.1mo HR 0.46 PFS: 18.7 vs 7.8...
#SABCS24 Part 2: Highlights w/ @jamecancerdoc ✅ #EUROPA ✅ #TAILORx ✅ #PADMA ✅ #EMBER3 Full 📢: ...
Sibylle Loibl presents Padma. Palbo plus ET improved TTF and PFS with OS trend compared to chemo. Patients should not get chemo first except in extraordinary situations. @OncoAlert...
#PADMA study presented by Dr. Loibl - looking at induction chemo followed by ET maint vs. upfront ET + CDk4/6 Another study- chemo inferior to ET + CDK4/6. 🆘 No need to do this...
At #SABCS24 LBA session - @LoiblSibylle on the PADMA trial comparing 1st line ET + Palbo vs Standard Mono-CT in High Risk HER2-/HR+ metastatic BC and indication for...
Padma study shows that first line treatment of ER+ MBC is >> better than first line single agent chemo. @SABCSSanAntonio #sabcs24

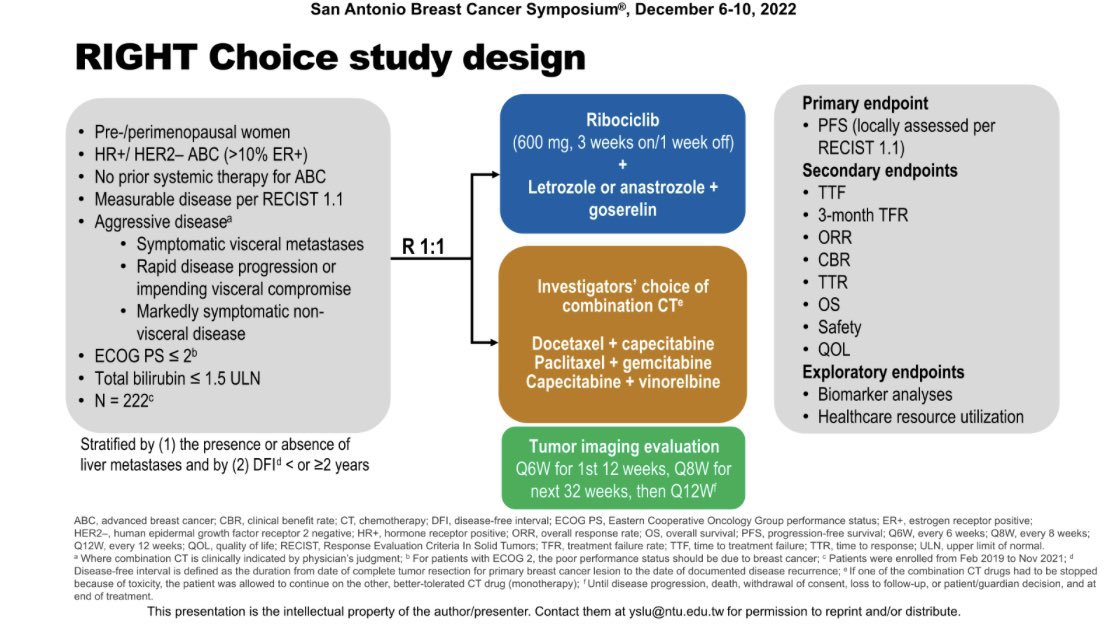
PADMA trial . Results similar to right choice trial . Not many pts with viceral crisis though. @Larvol @5_utr @OncoAlert @SABCSSanAntonio...
2. #PADMA: Ph III, HR+ metastatic breast cancer, chemo vs ET + Palbociclib. - #SABCS22 in #RightChoice study, we knew CDK4/6i upfront is better. -...

PADMA: High risk HR+/Her2- metastatic breast cancer -> physicians choice chemo + endocrine vs endocrine + palbociclib mOS was “numerically prolonged” p=0.46 Much higher high grade heme...

PADMA trial presented at #SABCS24 today Results supporting international guidelines advocating use of ET+CdK4/6i as standard first-line treatment for HR+mBC #bcsm...
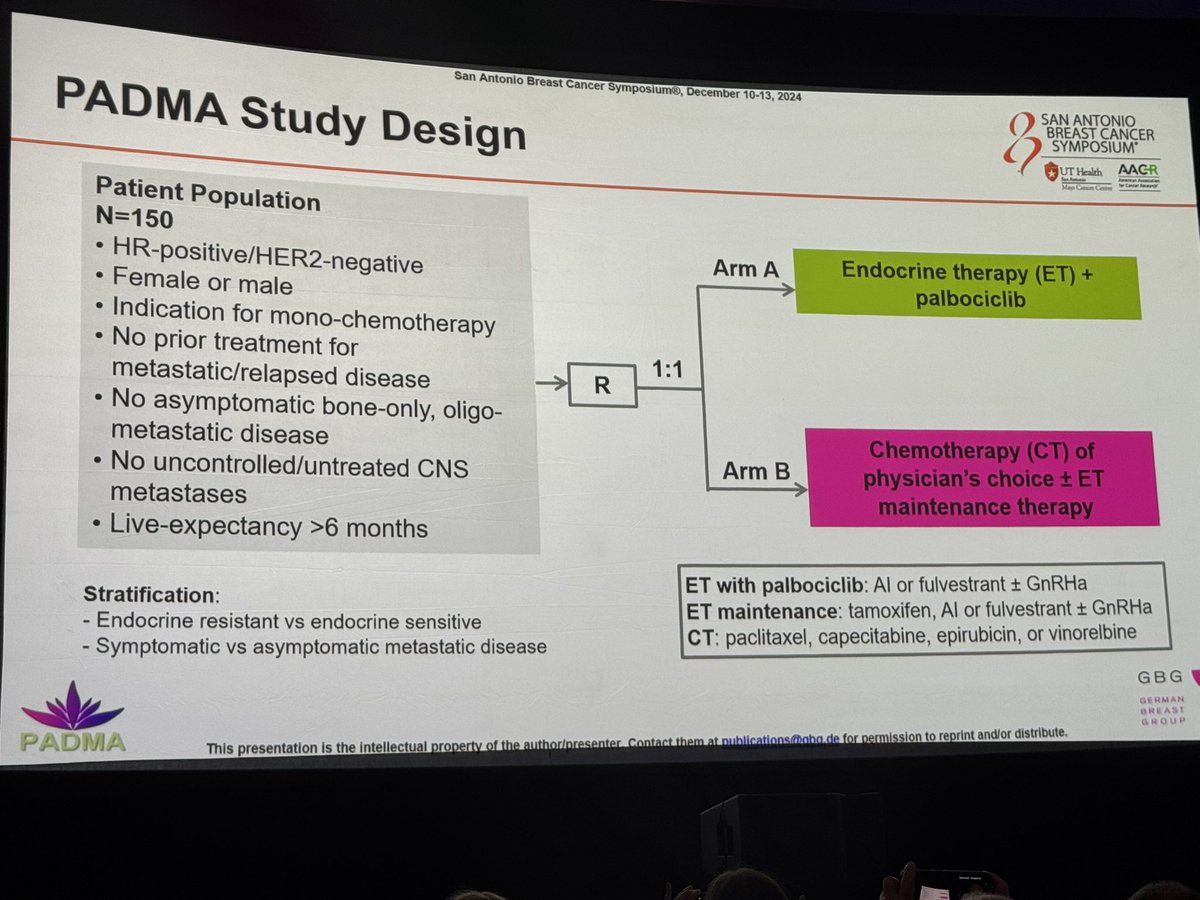
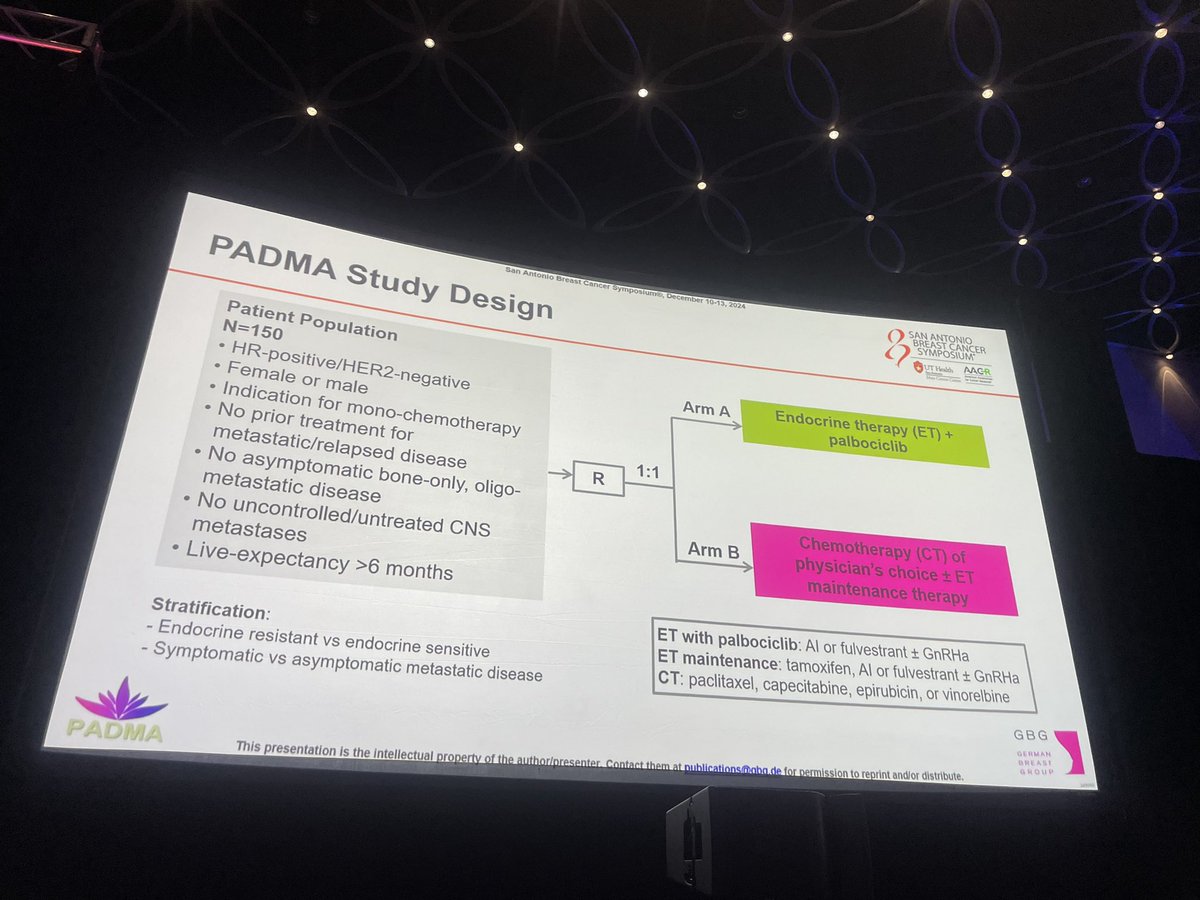
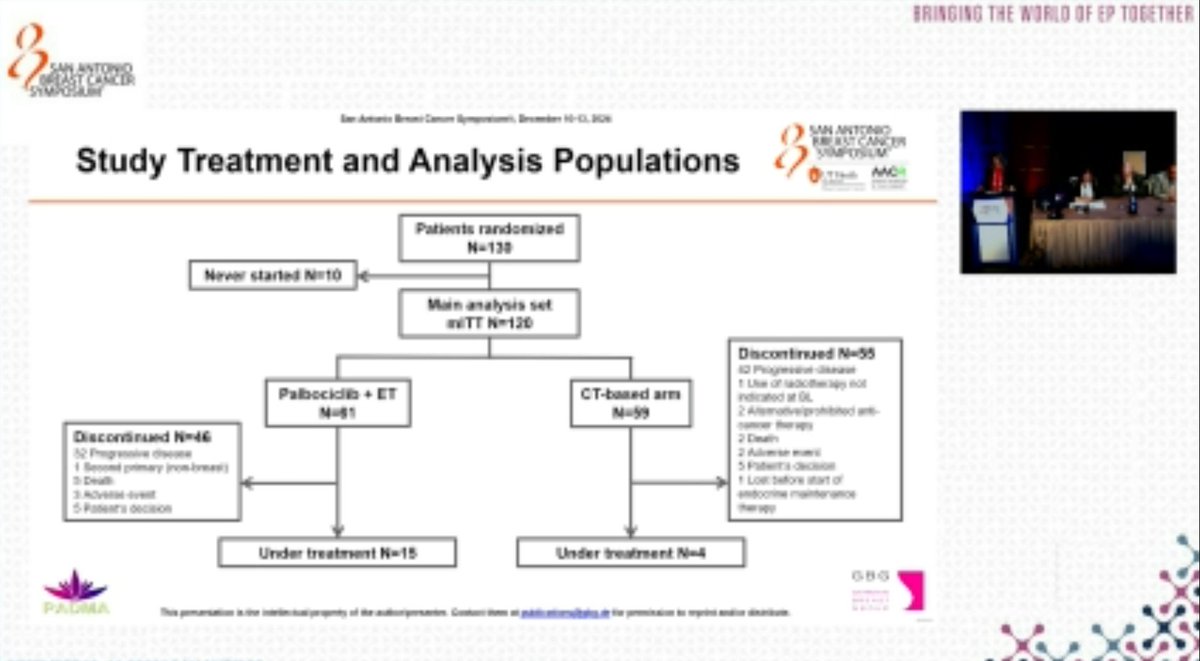
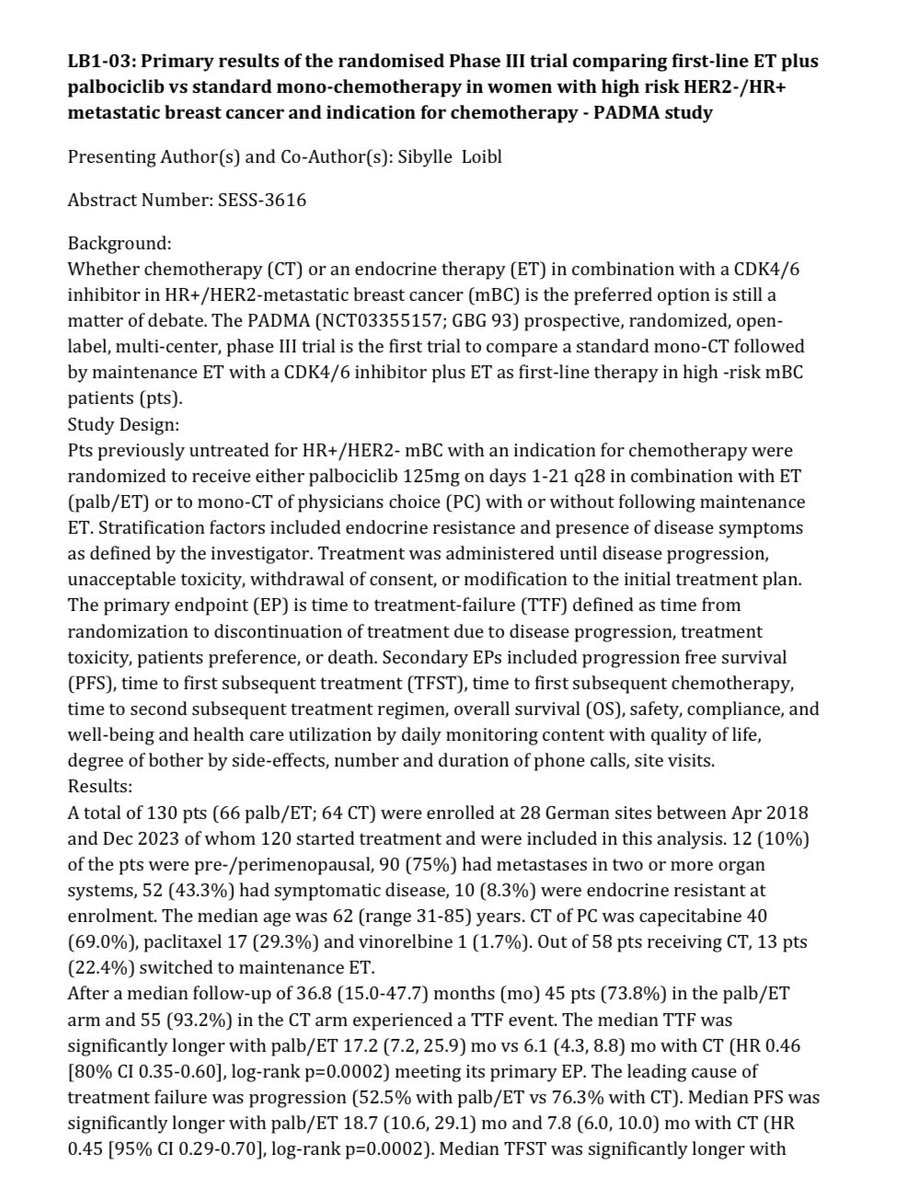
PADMA is a Phase IV, prospective, randomized, open-label, multicenter trial that is the first study to directly compare palbociclib (Ibrance) plus endocrine therapy against standard single-agent chemotherapy as first-line treatment for high-risk HR+/HER2- metastatic breast cancer. Conducted across 28 sites in Germany, the trial enrolled 130 patients with an indication for mono-chemotherapy. The results, presented at SABCS 2024, demonstrated that palbociclib plus endocrine therapy is significantly superior to chemotherapy, supporting existing international guidelines.
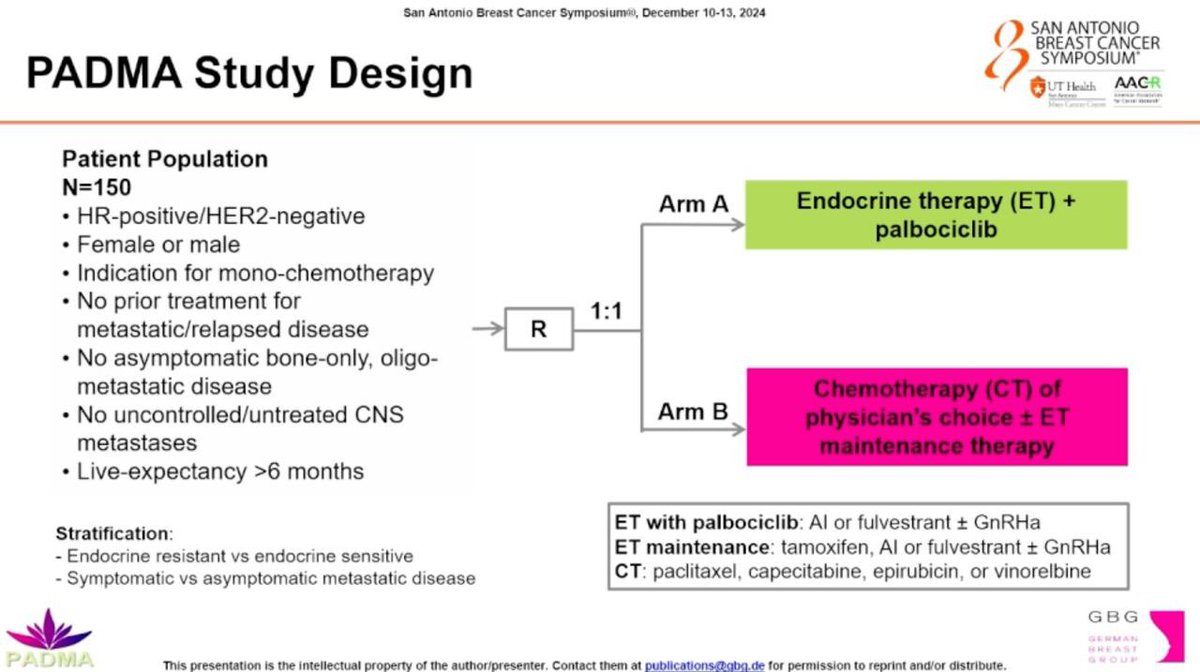
Phase IV, prospective, randomized 1:1, open-label, multicenter trial (NCT03355157; GBG 93). Patients were stratified by endocrine resistance vs. sensitivity and symptomatic vs. asymptomatic metastatic disease. Treatment continued until disease progression, unacceptable toxicity, withdrawal, or treatment plan change.
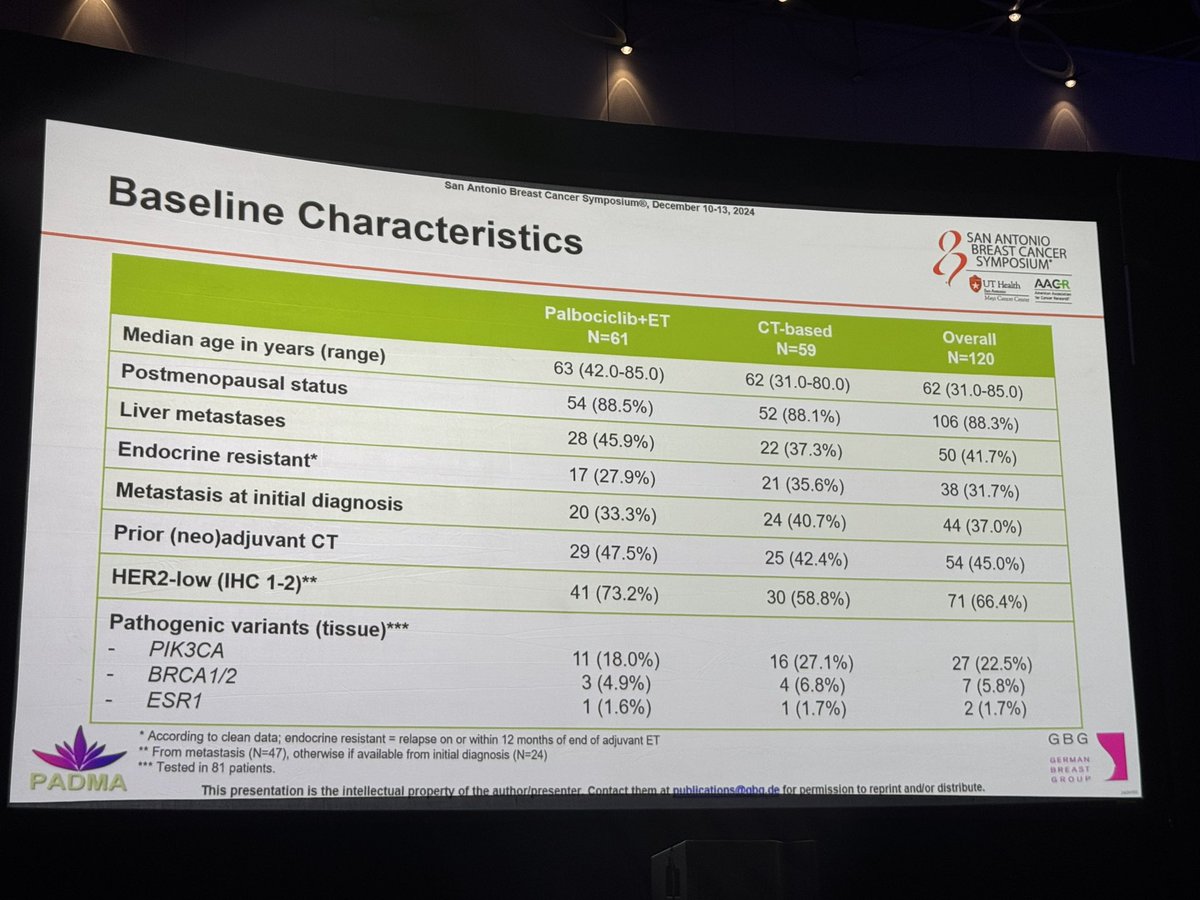
Previously untreated female and male patients with high-risk HR+/HER2- metastatic breast cancer with a clinical indication for mono-chemotherapy. Required life expectancy greater than 6 months. Excluded asymptomatic bone-only disease, oligo-metastatic disease, and uncontrolled CNS metastases. Median age 62 years; approximately 42% had liver metastases and 32% were ET-resistant.
Palbociclib 125 mg on days 1-21 of every 28-day cycle plus endocrine therapy (aromatase inhibitor or fulvestrant) versus mono-chemotherapy of physician's choice (capecitabine, paclitaxel, or vinorelbine) with or without subsequent maintenance ET.
Primary endpoint: Time to treatment failure (TTF), defined as time from randomization to discontinuation due to disease progression, toxicity, patient preference, or death. Secondary endpoints: PFS, OS, time to first subsequent treatment, safety, tolerability, treatment compliance, patient-reported QoL, and DMTI.
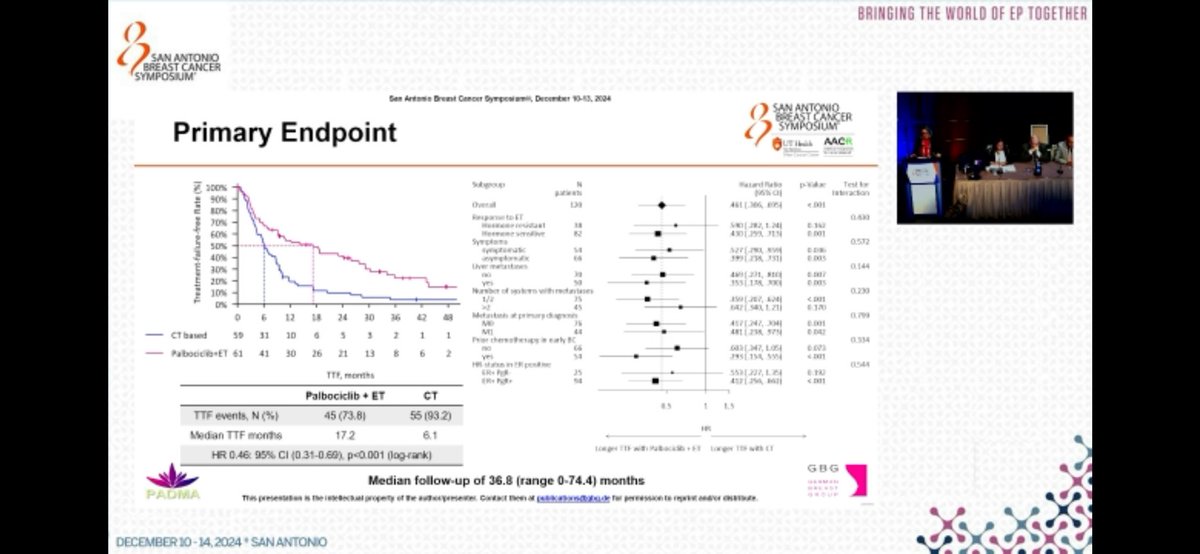
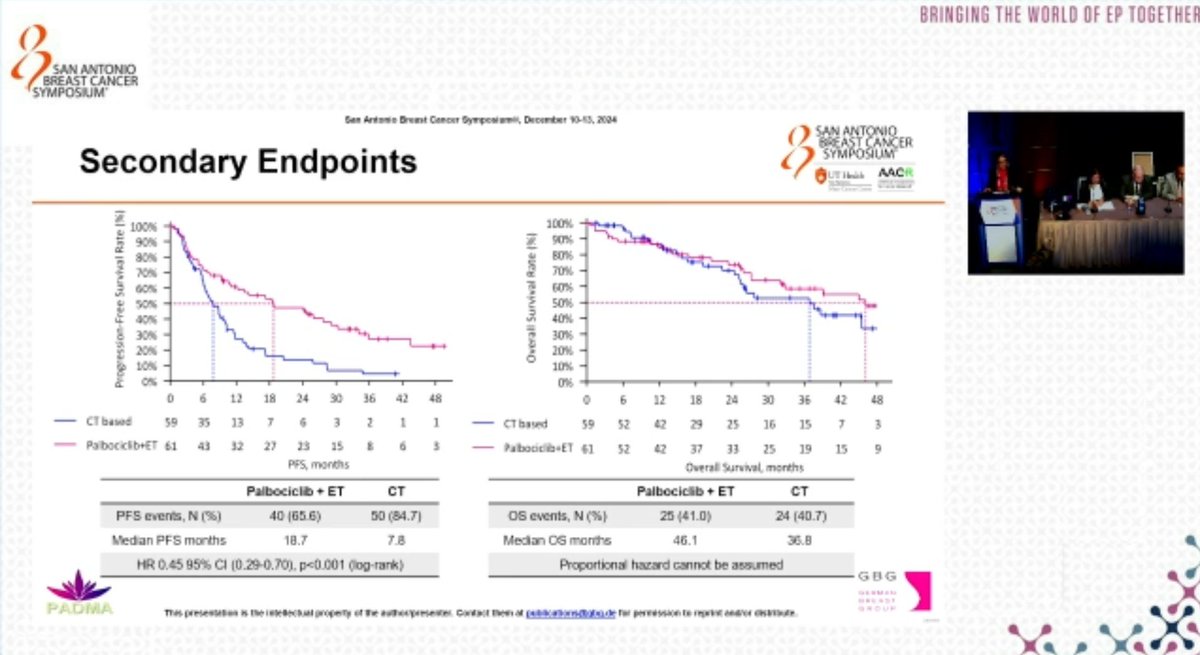
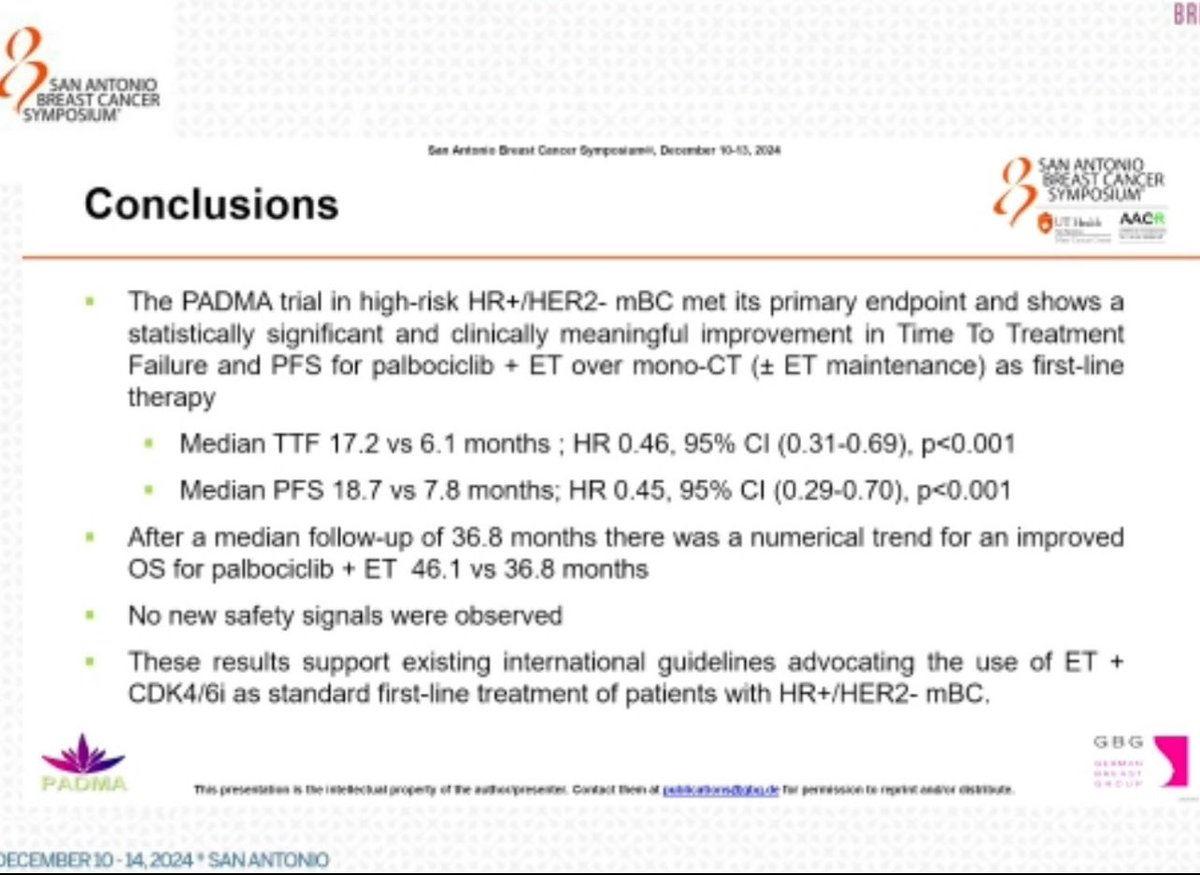
Palbociclib plus ET demonstrated a highly significant improvement in PFS versus chemotherapy. Median PFS was 18.7 months vs. 7.8 months (HR 0.45; 95% CI: 0.29-0.70; p<0.001). The primary endpoint TTF was also significantly improved: median TTF 17.2 months vs. 6.1 months (HR 0.46; 95% CI: 0.31-0.69; p<0.001). Disease progression was the leading cause of treatment failure: 52.5% in the palbociclib arm vs. 76.3% in the chemotherapy arm.
There was a numerical trend toward improved OS favoring palbociclib plus ET, though not statistically significant. Median OS was 46.1 months vs. 36.8 months in the chemotherapy arm (HR 0.81; 95% CI: 0.46-1.43; p=0.4630). Proportional hazards could not be assumed for the OS data.
Hematologic toxicity was significantly higher in the palbociclib arm: any-grade hematologic TRAEs 96.8% vs. 58.6% (p<0.001), Grade 3-4 hematologic TRAEs 54.8% vs. 6.9%. Non-hematologic adverse events were comparable between groups (82.3% vs. 93.1%). Overall Grade 3-4 TRAEs were 59.7% vs. 27.6%. Only 3 patients discontinued palbociclib due to adverse events. One treatment-related death (septic shock) occurred in the palbociclib arm.
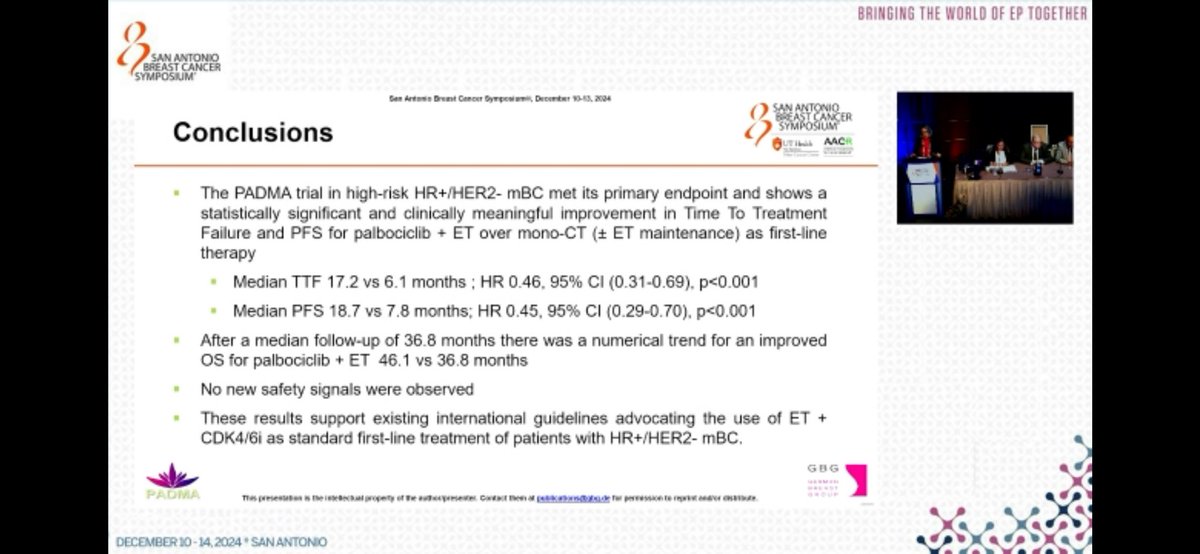
PADMA provides the first prospective, randomized evidence that CDK4/6 inhibitor-based endocrine therapy is superior to chemotherapy in high-risk HR+/HER2- mBC patients with an indication for chemotherapy. The results reinforce existing international guidelines recommending ET plus CDK4/6 inhibitors as standard first-line treatment. The patient-centric TTF endpoint captured broader clinical benefit including tolerability and treatment durability. While OS was numerically favored, longer follow-up is needed.
PADMA (NCT03355157) is a randomized, open-label, multicenter Phase IV trial from the German Breast Group (GBG) comparing first-line palbociclib (Ibrance) plus endocrine therapy against chemotherapy in patients with HR-positive, HER2-negative metastatic breast cancer who had an indication for chemotherapy. It provides prospective, randomized head-to-head data for these two first-line strategies.
Palbociclib plus endocrine therapy significantly improved median progression-free survival to 18.7 versus 7.8 months with chemotherapy (hazard ratio 0.45; 95% CI 0.29-0.70; p<0.001), with time to treatment failure of 17.2 versus 6.1 months. Overall survival showed a numerical trend favoring palbociclib plus endocrine therapy (46.1 versus 36.8 months) that was not statistically significant.
Yes. Palbociclib (Ibrance, Pfizer) is FDA-approved in combination with endocrine therapy for HR-positive, HER2-negative advanced or metastatic breast cancer. PADMA itself is an investigator-initiated randomized comparison of palbociclib plus endocrine therapy versus chemotherapy and is not a separate FDA registration trial.
Hematologic toxicity was more common with palbociclib plus endocrine therapy (any-grade hematologic treatment-related adverse events 96.8% versus 58.6%; grade 3-4 54.8% versus 6.9%), while non-hematologic adverse events were comparable between the arms. The palbociclib hematologic events, chiefly neutropenia, are generally manageable with monitoring and dose adjustment.
PADMA provides prospective, randomized evidence that CDK4/6 inhibitor-based endocrine therapy is superior in progression-free survival to chemotherapy as first-line treatment in high-risk HR-positive, HER2-negative metastatic breast cancer patients who otherwise had a chemotherapy indication, reinforcing guideline preference for endocrine therapy plus a CDK4/6 inhibitor.





