Anitocabtagene autoleucel (anito-cel) BCMA CAR-T for relapsed/refractory multiple myeloma -- Arcellx / Kite (Gilead)
Discover KOL Sentiment on iMMagine-1 →Design — Phase 2 registrational, single-arm; anito-cel (BCMA CAR-T) in R/R multiple myeloma (NCT05396885). (ASH 2024 / ASH 2025)
Response / MRD — ORR 96% (112/117); CR/sCR 74%; MRD-negativity 95% at 10⁻⁵ (median follow-up 15.9 mo). (page data / ASH)
PFS — 82.1% at 12 mo, 67.4% at 18 mo, 61.7% at 24 mo; Phase 1 median PFS ~30 mo. (page data / ASH)
Safety — CRS 86% (overwhelmingly Grade 0-1); ICANS 8% any grade; no delayed neurotoxicities reported. (page data)
Regulatory — Investigational — NOT FDA approved; BLA filed. (Arcellx / Kite press)
Sponsor / Drug — Arcellx / Kite (Gilead); anitocabtagene autoleucel (anito-cel), a BCMA-directed CAR-T therapy. (Arcellx)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 20, 2026.







Top 10 by impressions -- click to view on X
#2 Anitocabtagene Autoleucel for Relapsed Refractory Myeloma: IMMagine-1 Trial results. #ASH24 @freemanlciaraMD @bhemato @GKaurMD @DrKrinaPatel #ASH24 New CAR-T for myeloma. Registration study. Impressive results.
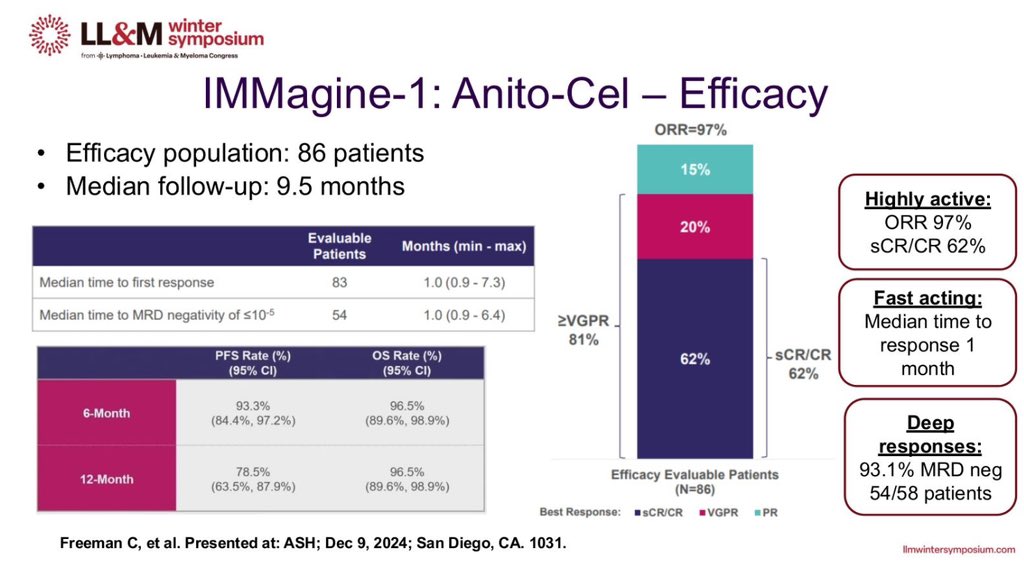
#ASH24: @arcellx CEO Rami Elghandour discusses a data update of the iMMagine-1 Study for the company's BCMA CAR-T. The data showed a 62% CR/sCR at a median follow-up of 9.5 months. #ASH24 $ACLX
#EHA2025: @arcellx CEO Rami Elghandour discusses the results presented today of the iMMagine-1 Study for the company's BCMA CAR-T. #EHA2025 $ACLX
Arcellx $ACLX $GILD Announces New Positive Data for Its iMMagine-1 Study in Patients With RRMM to be Presented During an Oral Presentation at #ASH24 #BCMA #CART (--> $JNJ $LEGN) Phase 2 iMMagine-1 DCO 31-10-2024 - mFU 9.5mo - n=86 evaluable for efficacy
Anito-cel: Updated data from IMMagine-1 trial (n=58; ~10 months median f/u) ORR/>=CR: 95%/62% (comparable to cilta-cel). No delayed neurotoxicity, CN palsies, GBS, or Parkinsonian-like symptoms till date
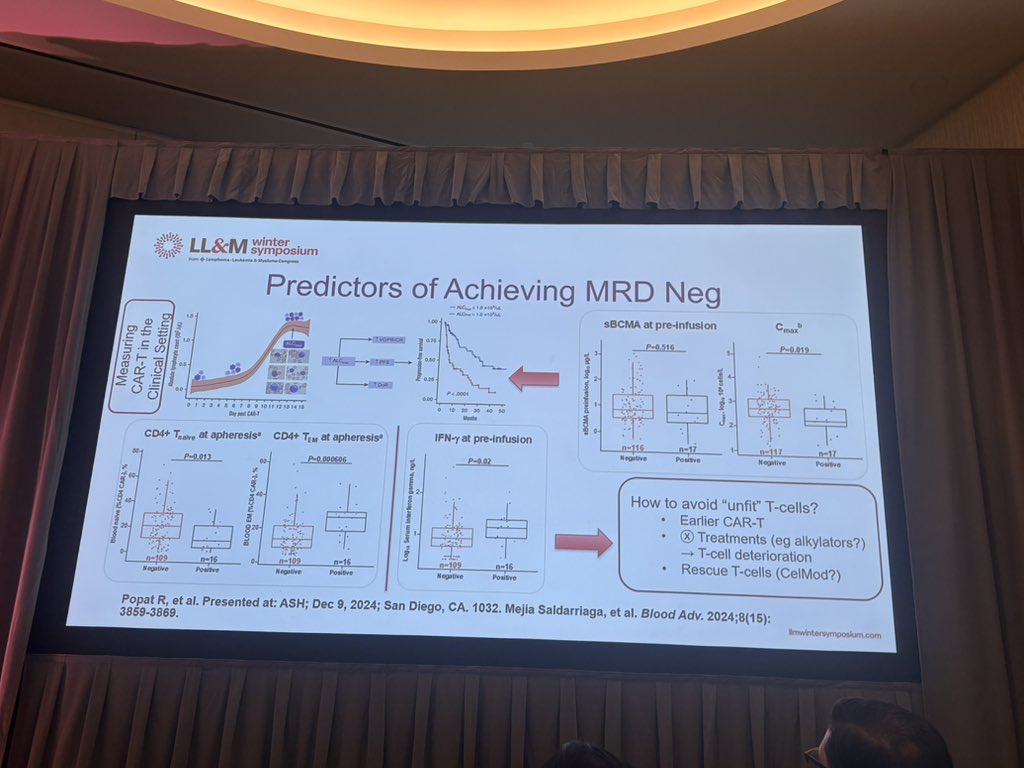
Cart for RRMM, by @mmejia91 Need to search for prognostic factors as lymphocytosis >1.0 x 103/uL Must discuss for all patients in 2nd line (> OS in cartitude 4) New Cart coming as Anitocel and GPRC5D targets being explored #LLMWinter2025

We're excited to share that our partner @Arcellx presented new data from the pivotal Phase 2 iMMagine-1 study in relapsed/refractory multiple myeloma at #EHA2025 today.

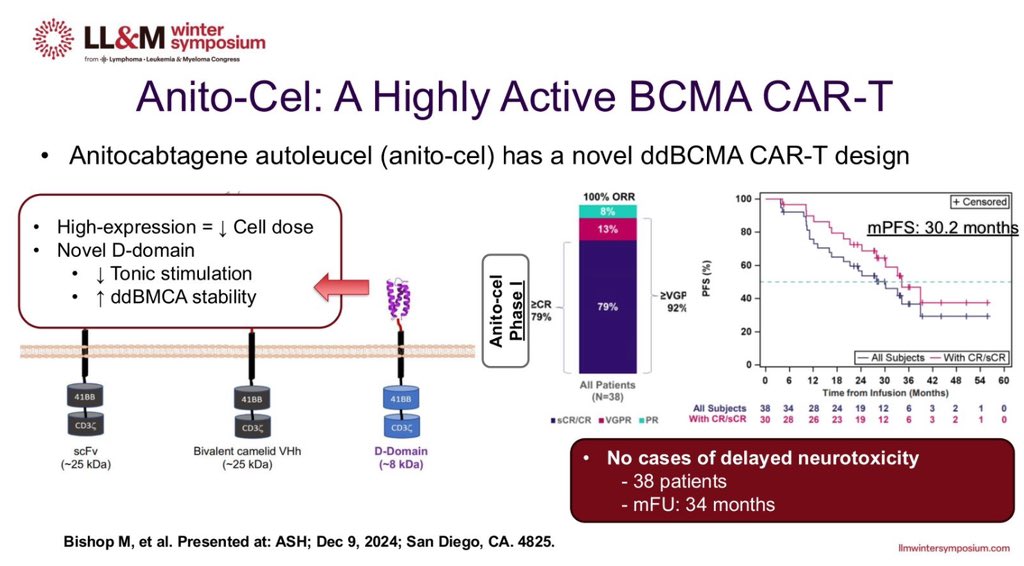
Didn't have time to post everything from #ASH24, but some additional highlights on the CAR T side of things. 1) Anito-cel: Poster 4825: Median PFS of 30 months from the phase 1, with high-risk disease performing at least as good as all-comers

9/ #EHA2025 #MMsm CAR-T: Not #ASCO25 per se but of course must add: S201 iMMagine-1 (@GKaurMD): Per press release, now n=117 anito-cel recipients (3+ prior LOT). MRD neg 70/117, 12-mo PFS 79%. I hope this gets approved ASAP!
2. iMMagine-1 Phase 2 trial of Anito-cel (@DrKrinaPatel): >=3 prior LoT, 86% triple-class refractory, 40% penta-refractory, ~40% with high-risk cytogenetics. >=CR rate~70% (79/117 patients) MRD-neg rate (10^-5) among evaluable patients (n=75): 93%
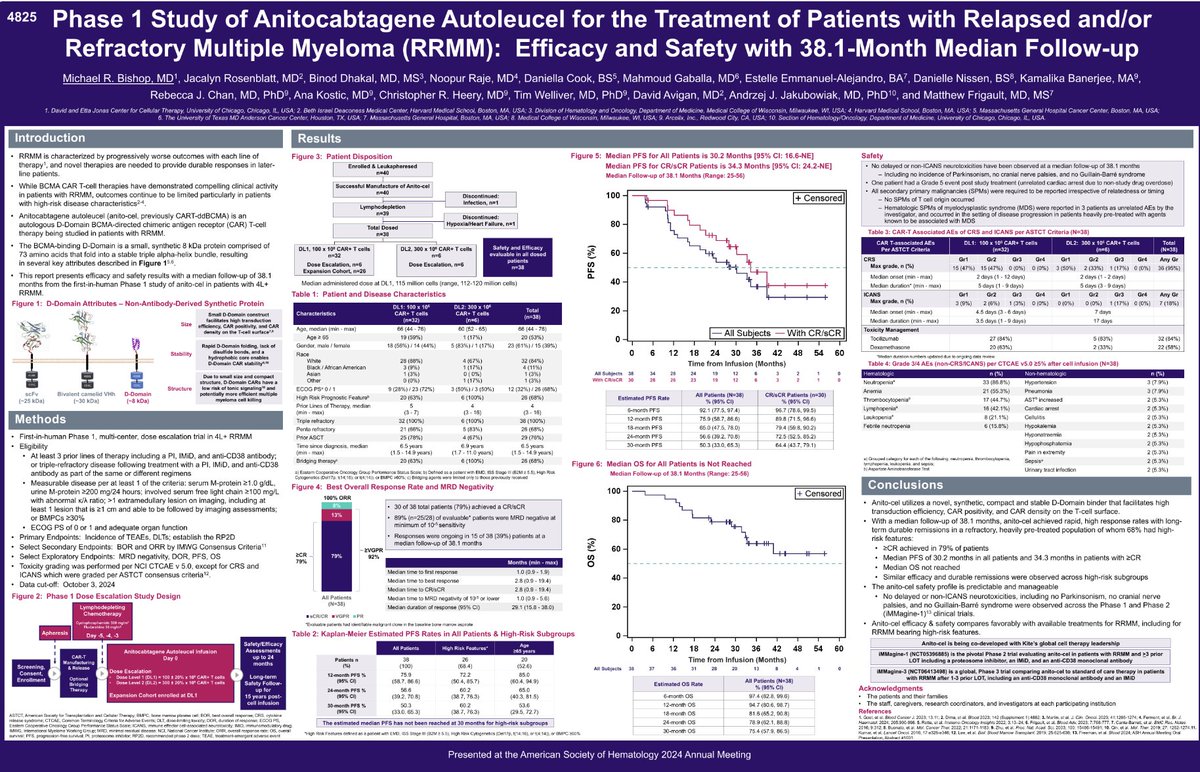
iMMagine-1 (NCT05469893) is a Phase 2 registrational study evaluating anitocabtagene autoleucel (anito-cel), an autologous BCMA-directed CAR-T cell therapy developed by Arcellx and Kite (a Gilead company), in patients with relapsed and/or refractory multiple myeloma who have received three or more prior lines of therapy. Anito-cel uses a novel, compact synthetic D-Domain binder (~8 kDa) instead of a traditional scFv, which may reduce tonic signaling and contribute to its differentiated safety profile. In the pivotal cohort of 117 triple-class exposed patients, anito-cel demonstrated an overall response rate (ORR) of 96% with a complete response/stringent complete response (CR/sCR) rate of 74%. MRD negativity rates were 95% at 10^-5 sensitivity and 78% at 10^-6. The safety profile was notable for low-grade CRS (83% Grade 0-1), very low ICANS (8%), and zero delayed neurotoxicities including no Parkinsonism or cranial nerve palsies. Anito-cel is investigational; a BLA has been filed with an anticipated PDUFA date of December 23, 2026. In February 2026, Gilead acquired Arcellx for up to $7.8 billion.
iMMagine-1 is a Phase 2 registrational, single-arm trial of anitocabtagene autoleucel (anito-cel), a BCMA-directed CAR-T therapy, in adults with relapsed/refractory multiple myeloma (NCT05396885).
No. Anitocabtagene autoleucel (anito-cel) is investigational and not FDA approved. A Biologics License Application has been filed for the treatment of relapsed/refractory multiple myeloma.
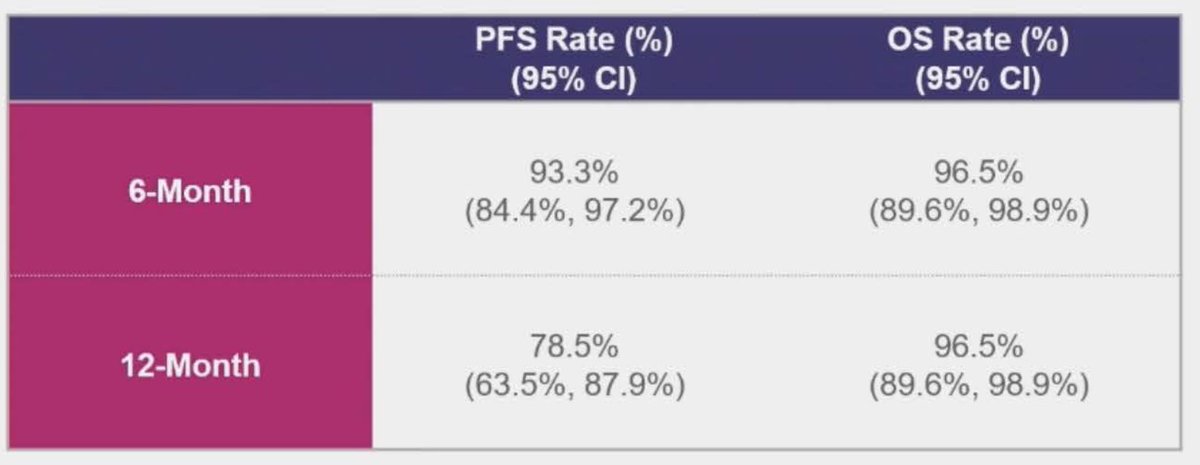
Among 117 evaluable patients at a median follow-up of 15.9 months, anito-cel achieved an overall response rate of 96% with a CR/sCR rate of 74%. MRD-negativity was reached in 95% of evaluable patients at 10⁻⁵. Progression-free survival was 82.1% at 12 months, 67.4% at 18 months, and 61.7% at 24 months.
Anito-cel showed a favorable safety profile: cytokine release syndrome occurred in 86% of patients but was overwhelmingly Grade 0-1, and ICANS occurred in only 8% of patients (92% had no ICANS). No delayed neurotoxicities were reported in the study.
Anitocabtagene autoleucel is developed by Arcellx in collaboration with Kite, a Gilead company.
Phase 2, single-arm, registrational/pivotal study of anitocabtagene autoleucel (anito-cel), an autologous BCMA-directed CAR-T cell therapy using a novel synthetic D-Domain binder. Manufacturing turnaround of 17 days or less with 96%+ in-spec rate.
117 patients with relapsed and/or refractory multiple myeloma, triple-class exposed (3+ prior lines of therapy). Approximately 40% penta-refractory, ~40% with high-risk cytogenetics.
Anitocabtagene autoleucel (anito-cel), a BCMA-directed CAR-T cell therapy with a compact 8 kDa D-Domain binder that reduces tonic signaling. Single infusion following lymphodepletion.
Overall response rate (ORR). Key secondary endpoints include CR/sCR rate, MRD negativity, duration of response, PFS, and OS.
In 117 evaluable patients at a median follow-up of 15.9 months, anito-cel achieved an ORR of 96% (112/117) with a CR/sCR rate of 74% (86/117). MRD negativity was achieved in 95% of evaluable patients at 10^-5 sensitivity and 78% at 10^-6. Sustained MRD negativity (6+ months) was observed in 83% of MRD-evaluable patients. Median time to MRD negativity was approximately 1 month.
PFS rates at key timepoints: 82.1% at 12 months, 67.4% at 18 months, and 61.7% at 24 months. Phase 1 data demonstrated a median PFS of 30 months, with high-risk disease performing at least as well as all-comers. These durability signals are particularly notable in a triple-class exposed, heavily pretreated population.
OS rates were 94% at 12 months, 88% at 18 months, and 83% at 24 months. These survival outcomes compare favorably in the context of heavily pretreated R/R multiple myeloma, though cross-trial comparisons should be interpreted with caution given the single-arm design.
The safety profile of anito-cel was differentiated by remarkably low-grade toxicity. CRS occurred in 86% of patients but was overwhelmingly Grade 0-1 (83% of all patients). Only 8% experienced ICANS of any grade, with 92% having no ICANS events. Critically, there were zero delayed neurotoxicities -- no movement and neurocognitive treatment-emergent adverse events (MNTs), no Parkinsonism, no cranial nerve palsies, and no Guillain-Barre syndrome. One Grade 5 CRS event was reported.
Anito-cel demonstrates competitive efficacy versus approved BCMA CAR-T therapies ciltacabtagene autoleucel (Carvykti) and idecabtagene vicleucel (Abecma), with a potentially differentiated safety profile characterized by the absence of delayed neurotoxicities. The 96% ORR, 95% MRD negativity rate, and 24-month PFS of 61.7% position anito-cel as a potential best-in-class BCMA CAR-T candidate. However, as this is a single-arm study, cross-trial comparisons are unreliable and randomized data against established CAR-T options would be needed to confirm superiority. Anito-cel remains investigational (BLA filed, PDUFA Dec 2026).




