Post-ASCT maintenance NDMM - Janssen
Discover KOL Sentiment on AURIGA →
















Top 10 by impressions - click to view on X
🚨🚨a 🧵 of AURIGA Study 1/The study aimed to determine if adding daratumumab to standard lenalidomide maintenance would improve outcomes in MRD-positive patients with at least VGPR post-ASCT Phase 3,...
🚨 AURIGA results in #IMS24 app! After ASCT in #MMsm, 30-mo PFS 83% Dara-R vs 66% R alone. Can’t directly extrapolate to quad induction or MRD- after ASCT, and not...
Let's talk AURIGA: Dara-R vs R maintenance for myeloma patients post-ASCT with MRD-positivity without prior CD38-exposure (#IMS24) 🥇endpt: MRD<10^-5...
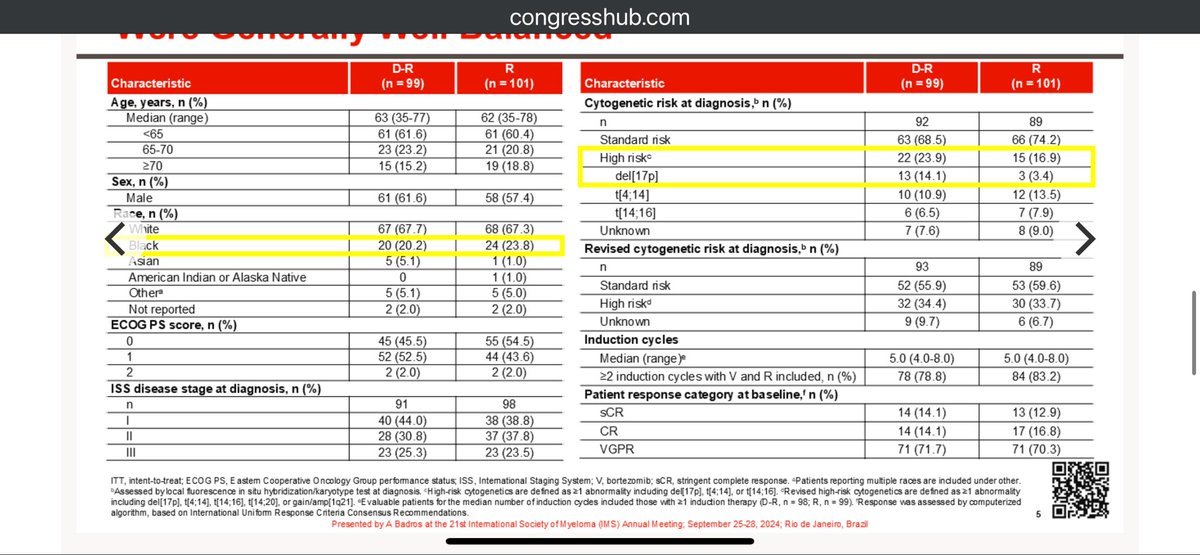
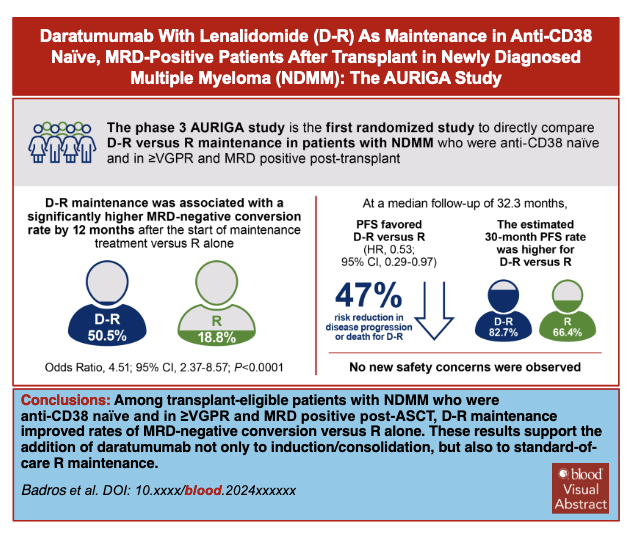
AURIGA - DaraR vs R alone in MRD+ post SCT and CD38 naive. Primary endpoint conversion to MRD neg. Slightly more HR markers in DR arm. P53 14 vs 3%. Primary endpoint 50.5 vs 18.8...
Published in @BloodJournal #mmsm and presented in #IMS24 : AURIGA study 🧵 N=194 pts Median follow up <3 years This is for patients with anti-CD38...

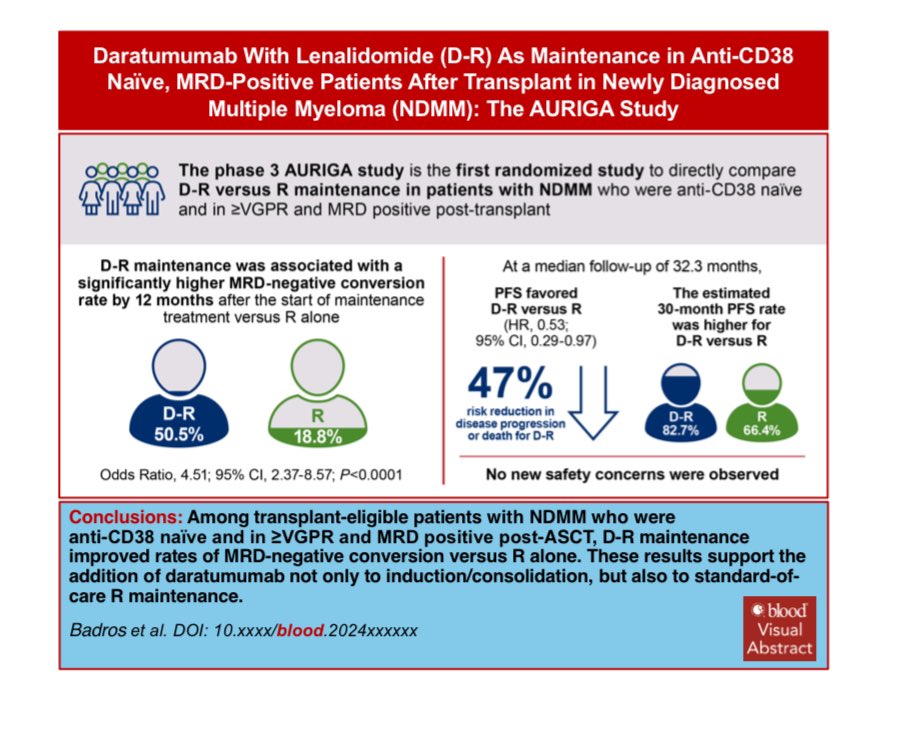
#Myeloma Paper of the Day: Phase 3 AURIGA study of Dara/Rev vs. Rev maintenance in newly diagnosed MM post-ASCT w/ ≥VGPR/MRD+ & anti-CD38 naïve shows Dara/Rev superior w/ 47%...

DARZALEX (daratumumab) SC-based regimens improve MRD negativity and PFS in NDMM (CEPHEUS, AURIGA), and OS in AL amyloidosis (ANDROMEDA) #ASH24 $JNJ $GMAB CEPHEUS: 85% of pts who...

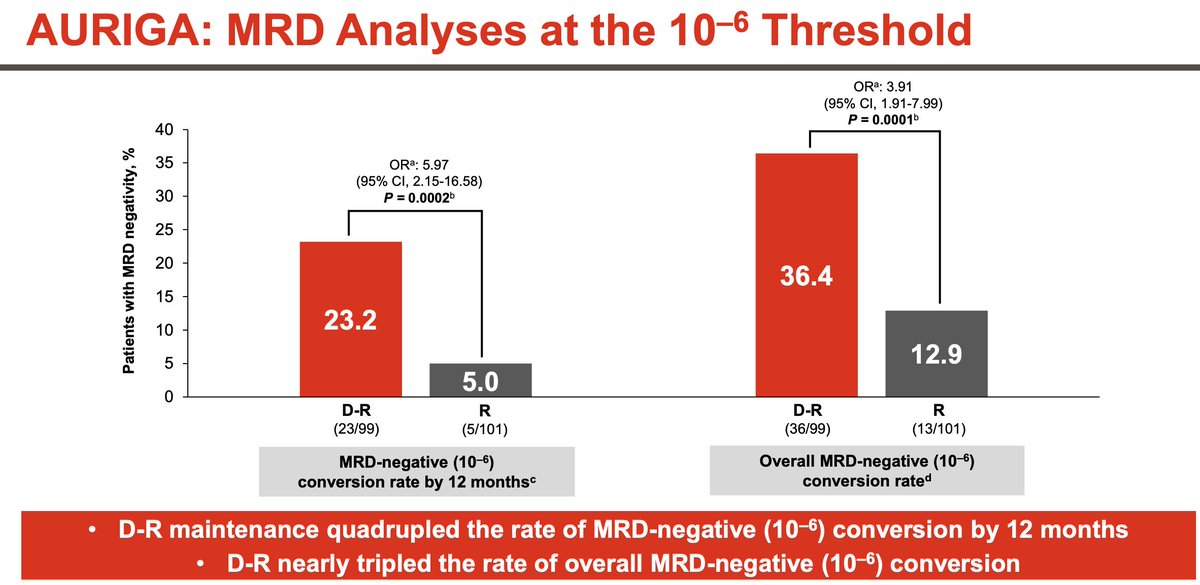
D-R maintenance improved MRD-negative conversion rate in patients with NDMM who were MRD-positive after transplant vs R maintenance. #clinicaltrialsandobservations...
This is really important and justifies DR ongoing treatment but ? For 2, 3, 4 years or more. I’m seeing very few early relapses with this approach
#IMS24 my approach to post-ASCT maintenance in myeloma (“just len”!) before versus after AURIGA. (Image courtesy @juneklanoue @AjaiChari @SLentzsch) glad...
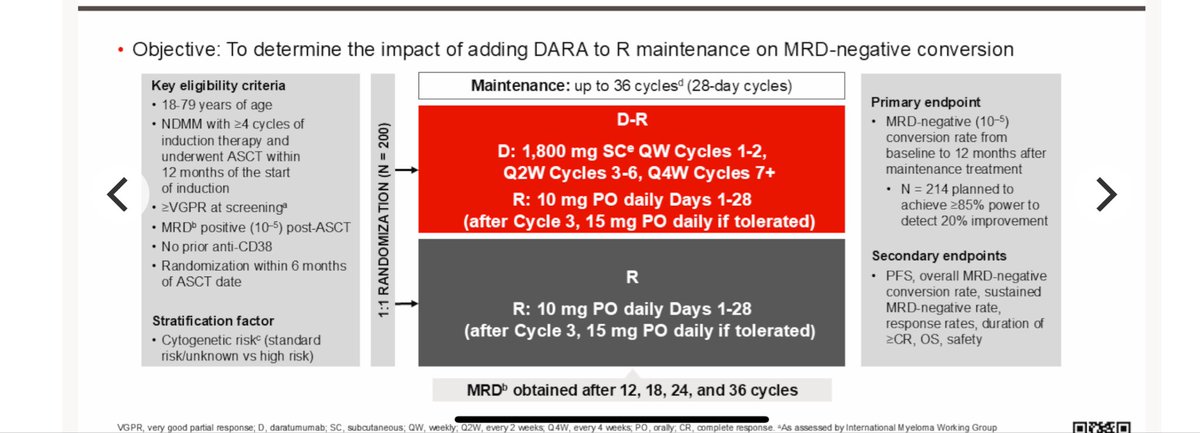
AURIGA is a Phase III, open-label, multicenter, randomized trial evaluating the addition of subcutaneous daratumumab (Darzalex Faspro) to lenalidomide maintenance (D-R) versus lenalidomide alone (R) in patients with newly diagnosed multiple myeloma who are MRD-positive after autologous stem cell transplant. The trial enrolled 200 anti-CD38-naive patients who had achieved VGPR or better post-ASCT. AURIGA is the first Phase III study designed to evaluate MRD-negative conversion as a primary endpoint in the post-transplant maintenance setting.
Phase III, open-label, active-controlled, 1:1 randomized, multicenter trial (NCT03901963). Patients received D-R or R alone in 28-day cycles for up to 36 cycles. Daratumumab SC 1,800 mg was administered weekly (cycles 1-2), every 2 weeks (cycles 3-6), and every 4 weeks (cycle 7+). Lenalidomide started at 10 mg daily (days 1-28), increasing to 15 mg after cycle 3 if tolerated. Stratified by cytogenetic risk (standard/unknown vs high).
Adults aged 18-79 with newly diagnosed multiple myeloma, MRD-positive (10-5 by NGS) after ASCT, in VGPR or better, anti-CD38 naive, who received at least 4 induction cycles and were enrolled within 12 months of induction start and 6 months of ASCT. ECOG PS 0-2. High-risk cytogenetics defined as del(17p), t(4;14), and/or t(14;16).
Arm A: Subcutaneous daratumumab 1,800 mg + lenalidomide (D-R) for up to 36 cycles. Arm B: Lenalidomide alone (R) for up to 36 cycles. Treatment continued until disease progression, unacceptable toxicity, or consent withdrawal.
Primary endpoint: MRD-negativity conversion rate (10-5 by NGS) by 12 months from maintenance initiation. Secondary endpoints: overall MRD-negativity conversion rate, sustained MRD-negativity (6 and 12 months), CR or better rate, PFS, and OS.
At updated analysis (median follow-up 40.3 months), D-R demonstrated a significant PFS benefit with median PFS not reached vs 47.2 months for R (HR 0.55; 95% CI 0.33-0.91; p=0.0183). The MRD-negativity conversion rate (10-5) was 60.6% for D-R vs 28.7% for R (OR 3.92; 95% CI 2.16-7.14; p<0.0001). At 12 months, MRD conversion was 50.5% vs 18.8% (OR 4.51; p<0.0001). Sustained MRD-negativity (10-5) for 12 months or more was 29.3% vs 7.9% (OR 4.88; p=0.0001). No patient achieving sustained MRD-negativity on D-R experienced progression.
Overall survival data remain immature. At a median follow-up of 40.3 months, OS HR was 0.42 (95% CI 0.14-1.20; p=0.0954), with estimated 36-month OS of 94.7% for D-R vs 90.5% for R. A total of 16 patients died: 5 in the D-R group and 11 in the R group. OS trends favor D-R but have not reached statistical significance.
Grade 3/4 cytopenias occurred in 54.2% of D-R vs 46.9% of R patients. Grade 3/4 infections were 19.8% vs 14.3%. Serious TEAEs were reported in 31.3% vs 25.5%. Treatment discontinuation due to AEs was 12.5% vs 9.2%. TEAE-related deaths occurred in 2.1% (D-R) vs 1.0% (R), all due to infections (COVID-19 pneumonia, Legionella pneumonia). No new safety signals identified with the addition of daratumumab.
AURIGA demonstrates that adding subcutaneous daratumumab to lenalidomide maintenance significantly deepens MRD responses and improves PFS in MRD-positive post-transplant patients. The MRD conversion benefit was consistent across cytogenetic risk subgroups, including high-risk patients. However, D-R maintenance post-ASCT is not yet FDA approved; the current standard daratumumab frontline approval (PERSEUS) uses D-VRd induction through maintenance. Key debates include optimal patient selection (MRD-positive only vs all patients), sequencing with PERSEUS-style D-VRd, and whether MRD-guided treatment discontinuation is feasible.












