Adjuvant HCC after complete radiologic response post-resection or ablation — Merck Sharp & Dohme LLC
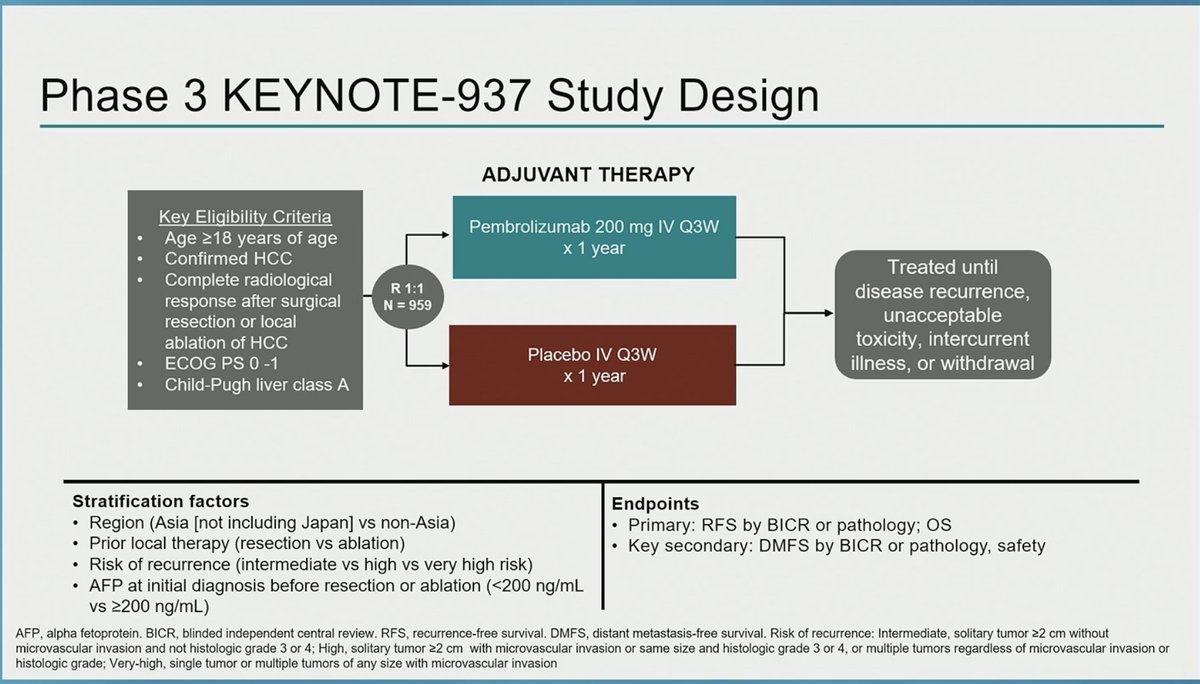
Discover KOL Sentiment on KEYNOTE-937 →Design - Phase 3 adjuvant pembrolizumab vs placebo after complete resection or ablation in HCC (NCT03867084).
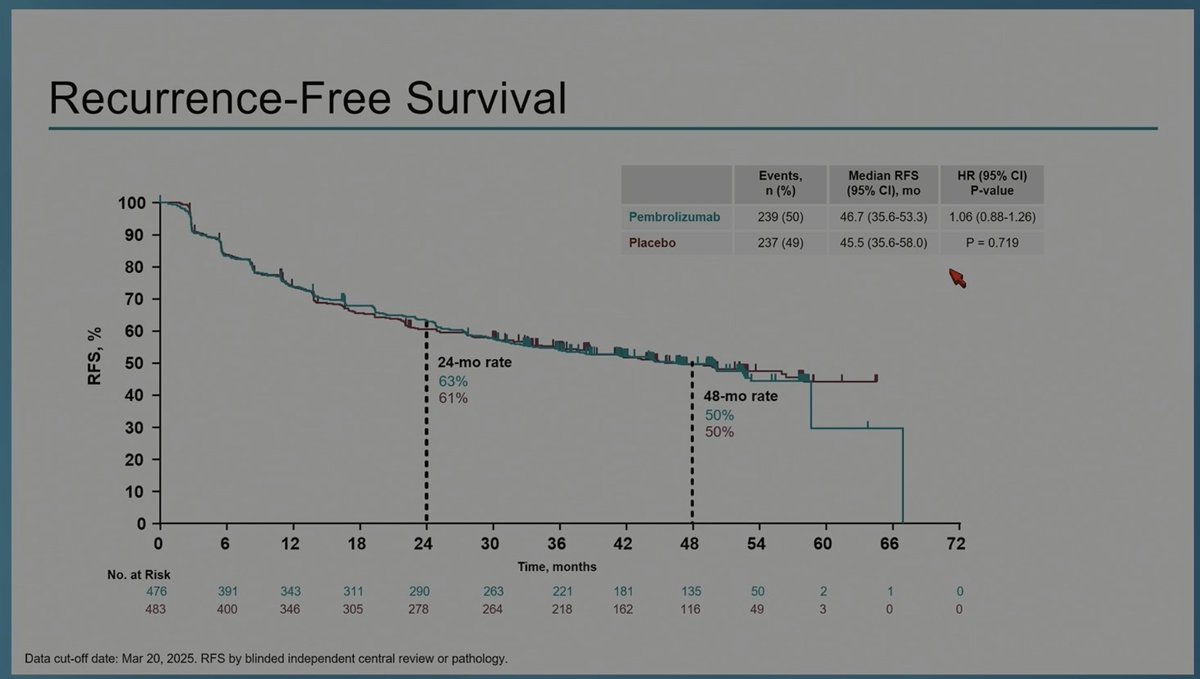
RFS (primary) - NEGATIVE - median 46.7 vs 45.5 mo, HR 1.06 (95% CI 0.88-1.26), P=0.719; 48-month RFS 50% in both arms. Primary endpoint not met.
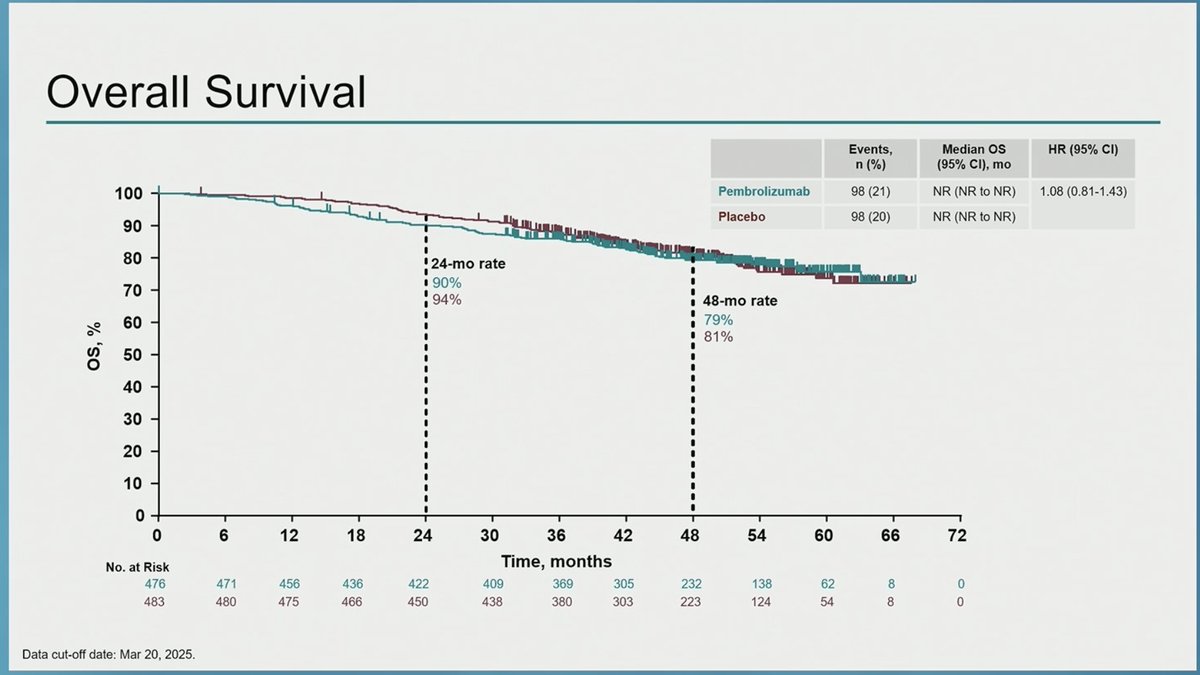
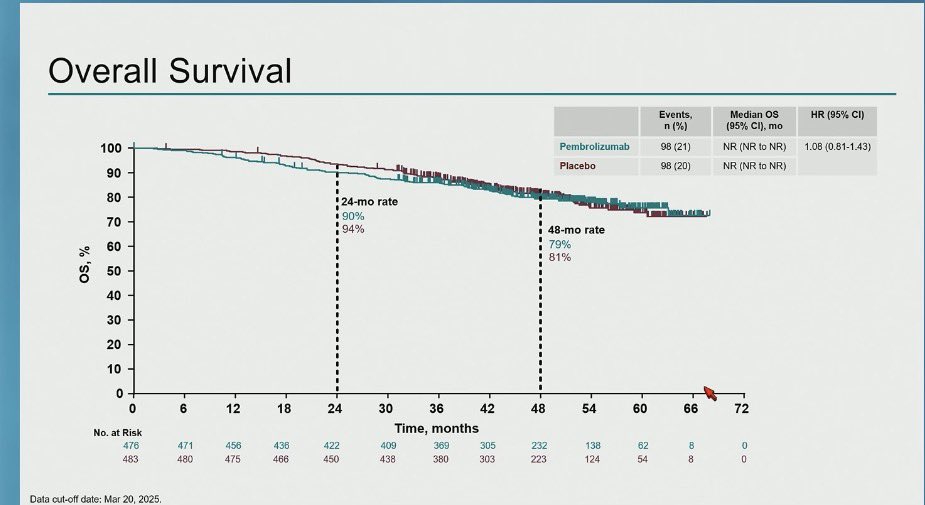
OS - No benefit - median not reached in either arm; descriptive HR 1.08 (95% CI 0.81-1.43); 48-month OS 79% vs 81%.
Safety - Grade >=3 treatment-related AEs 14% vs 5%; treatment-related discontinuation 10% vs 1%; no treatment-related deaths.
Regulatory - Investigational - NOT FDA approved for adjuvant HCC; standard of care unchanged.
Sponsor / drug - Merck (MSD); pembrolizumab (Keytruda).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.













Top tweets by impressions — click to view on X
#GI26 KEYNOTE-937 (phase III)
🔀 Adj HCC (PEM vs PBO) after complete radiologic response (resection/ablation)
📉 RFS: 46.7 vs 45.5 mo; (HR 1.06; P=0.72)
📉 OS: 48-mo OS 79% vs 81%
🛡️ Higher grade ≥3 AEs…
#GI26
KEYNOTE-937 is a letdown, but the story feels familiar 😕🩸
Phase 3 KEYNOTE-937 tested pembrolizumab after surgical resection or local ablation for HCC. This was the long-awaited attempt to…
Negative trials matter too!
Especially given the paradigm shift towards IO in HCC since 2020, it is important (if disappointing) to learn that adjuvant pembrolizumab does not affect survival outcomes…
keynote 937 negative study for adjuvant #HCC in line with prior results from IMbrave 050. Unfortunately, still lack of positive #HCC trials. Novel strategies needed since given uniqueness of HCC…
Keynote-937 phs-3: pembrolizumab for HCC after surgical resection or local ablation
#ASCOGI26
👉mRFS: 46 vs 45 mo
👉4-yr RFS rate: 50 vs 50%
🧐Very disappointing, but inline with IMBRAVE-050, now we…
KEYNOTE-937- adj pembro v placebo #HCC
➡️ 2nd -ve trial; n=959, mFU 50.7mths
➡️ maj viral aetiology; 77% AFP<200, 83% BCLCA
➡️mRFS 46.7 v 45.5mo, mOS NR either arm
➡️≥G3 AEs 32 v 22%
higher mRFS…

Dr. Chan @CUHKofficial rand PhIII KN-937 trial of adj #pembrolizumab X1 year in #HCC after surgery or local ablation ➡️ no sig improvement in #RFS (primary endpoint) vs placebo (HR 1.06), no diff in…

6. KEYNOTE-937: PhIII, Adj Pembrolizumab vs. placebo post-resection/ablation in HCC.
- No RFS benefit: 46.7mos vs 45.5mos (HR 1.06).
- Did not improve outcomes. Negative study!
7/7…

KEYNOTE-937 highlights that adjuvant pembrolizumab after complete radiologic response in HCC does not improve RFS or OS, with higher ≥G3 AEs. Important negative trial shaping practice. #GI26 #HCC…

🚨KEYNOTE-937🚨
Resected or ablated early stage HCC
🔎Adjuvant Pembro vs Placebo
🛑No improvement in RFS and no suggestion of improvement in OS
🧐Findings similar to IMBrave050… more work needed to…
Second negative phase 3 adjuvant immunotherapy trial in HCC after IMbrave-050 showed loss of initial RFS benefit with longer follow-up. Community is shifting toward perioperative (neoadjuvant + adjuvant) immunotherapy strategies. Current SOC for resected/ablated HCC remains surveillance.
Median RFS was 46.7 months with pembrolizumab vs. 45.5 months with placebo (HR 1.06, 95% CI 0.88-1.26, P=0.719). 48-month RFS rate was 50% in both arms. Primary endpoint was not met; per hierarchical testing, OS was not formally tested.
Median OS was not reached in either arm (descriptive HR 1.08, 95% CI 0.81-1.43, nominal P=0.704). 48-month OS rate was 79% (pembrolizumab) vs. 81% (placebo). No OS benefit.
Grade ≥3 treatment-related adverse events occurred in 14% of pembrolizumab patients vs. 5% with placebo. Treatment-related discontinuation was 10% vs. 1%. No treatment-related deaths. Most common TRAEs: pruritus, rash, hypothyroidism.
⚠️ Negative trial — standard of care unchanged. Second negative phase 3 adjuvant immunotherapy trial in HCC after IMbrave-050 showed loss of initial RFS benefit with longer follow-up. Community is shifting toward perioperative (neoadjuvant + adjuvant) immunotherapy strategies. Current SOC for resected/ablated HCC remains surveillance.
KEYNOTE-937 is a Phase 3 randomized trial (NCT03867084) of adjuvant pembrolizumab (Keytruda) versus placebo in patients with hepatocellular carcinoma who achieved a complete radiologic response after surgical resection or local ablation. Recurrence-free survival was the primary endpoint.
No. KEYNOTE-937 was a negative trial. Median recurrence-free survival was 46.7 months with pembrolizumab versus 45.5 months with placebo (HR 1.06; 95% CI 0.88-1.26; P=0.719), and the 48-month RFS rate was 50% in both arms. Because the primary endpoint was not met, overall survival was not formally tested; the descriptive OS hazard ratio was 1.08 with no benefit.
No. Pembrolizumab (Keytruda) is not FDA approved as adjuvant therapy for hepatocellular carcinoma. KEYNOTE-937 did not demonstrate a recurrence-free or overall survival benefit in this setting, so the standard of care in adjuvant HCC is unchanged. Pembrolizumab remains approved in many other cancer types.
Grade 3 or higher treatment-related adverse events occurred in 14% of pembrolizumab patients versus 5% with placebo, and treatment-related discontinuation was 10% versus 1%. No treatment-related deaths were reported; the most common events were pruritus, rash, and hypothyroidism, consistent with the known checkpoint-inhibitor profile.
KEYNOTE-937 is the second negative Phase 3 adjuvant immunotherapy trial in HCC, following IMbrave-050, which lost its initial recurrence-free survival benefit with longer follow-up. These results have shifted interest toward perioperative (neoadjuvant plus adjuvant) immunotherapy strategies, which are being tested in ongoing trials.