CHRYSALIS-2 (NCT04077463) is a Phase 1/1b study of amivantamab (Rybrevant) plus lazertinib (Lazcluze); Cohort C enrolled treatment-naive advanced NSCLC with atypical/uncommon (non-exon-20-insertion) EGFR mutations. In 49 first-line patients the combination produced an objective response rate of 57%, median progression-free survival of 19.5 months and median overall survival of 41.0 months (ASCO 2026, Abstract 8501). This atypical-EGFR use is investigational. Sponsor: Johnson & Johnson.
ASCO 2026 · Abstract 8501 · OS UpdateAtypical EGFR-mutated NSCLC1st-LinePhase 1/1bAmivantamab + Lazertinib · Johnson & Johnson
Response (primary) — Investigator-assessed ORR 57%; median duration of response 20.7 months (95% CI 9.9-NE). (ASCO 2026)
PFS — Median progression-free survival 19.5 months (95% CI 11.2-NE). (ASCO 2026)
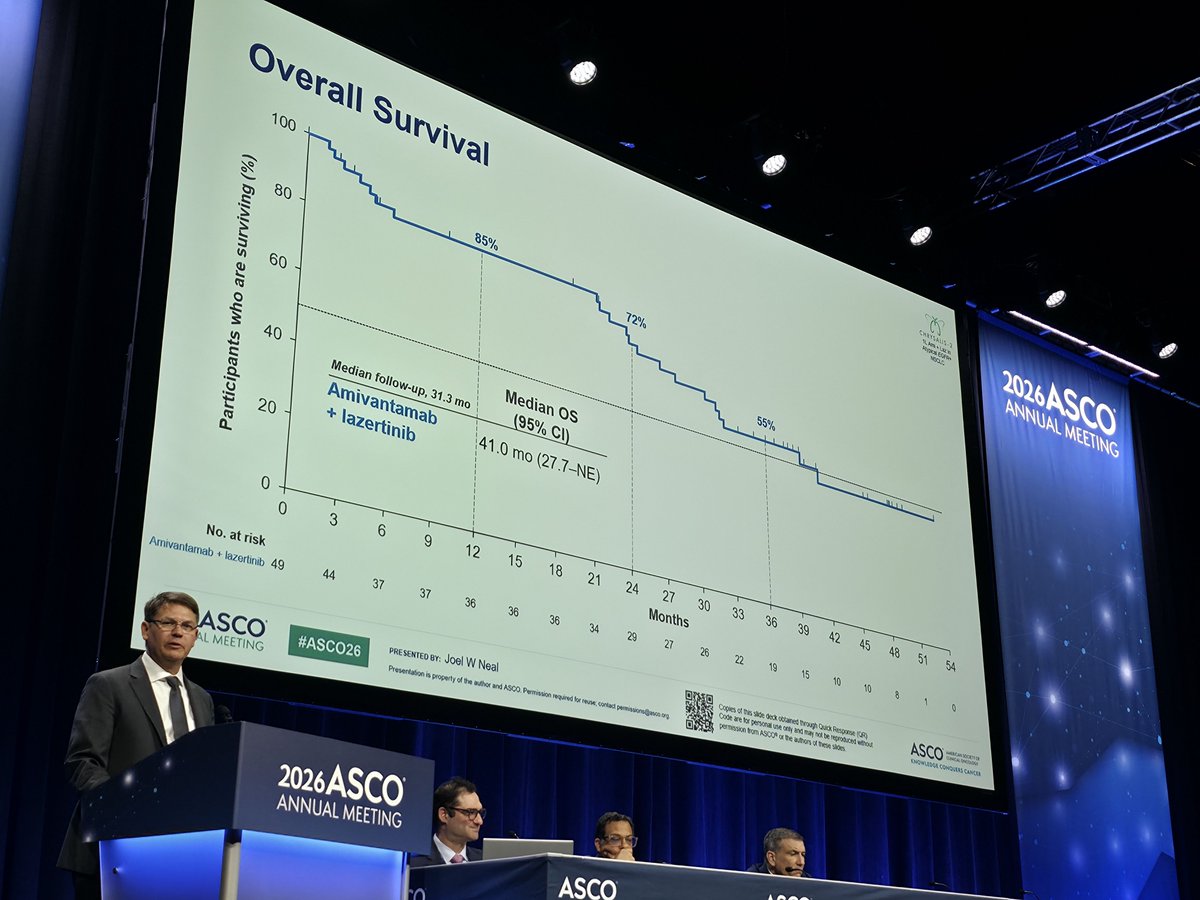
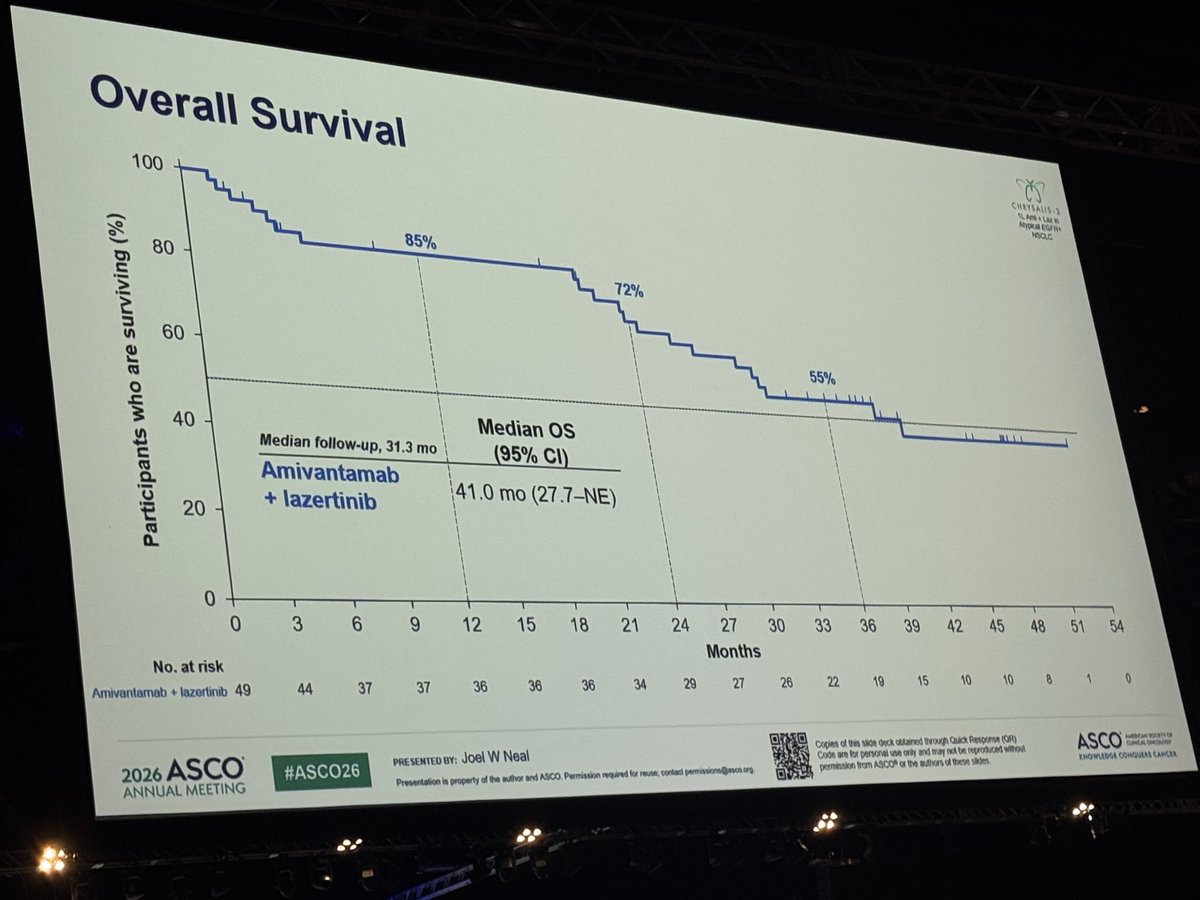
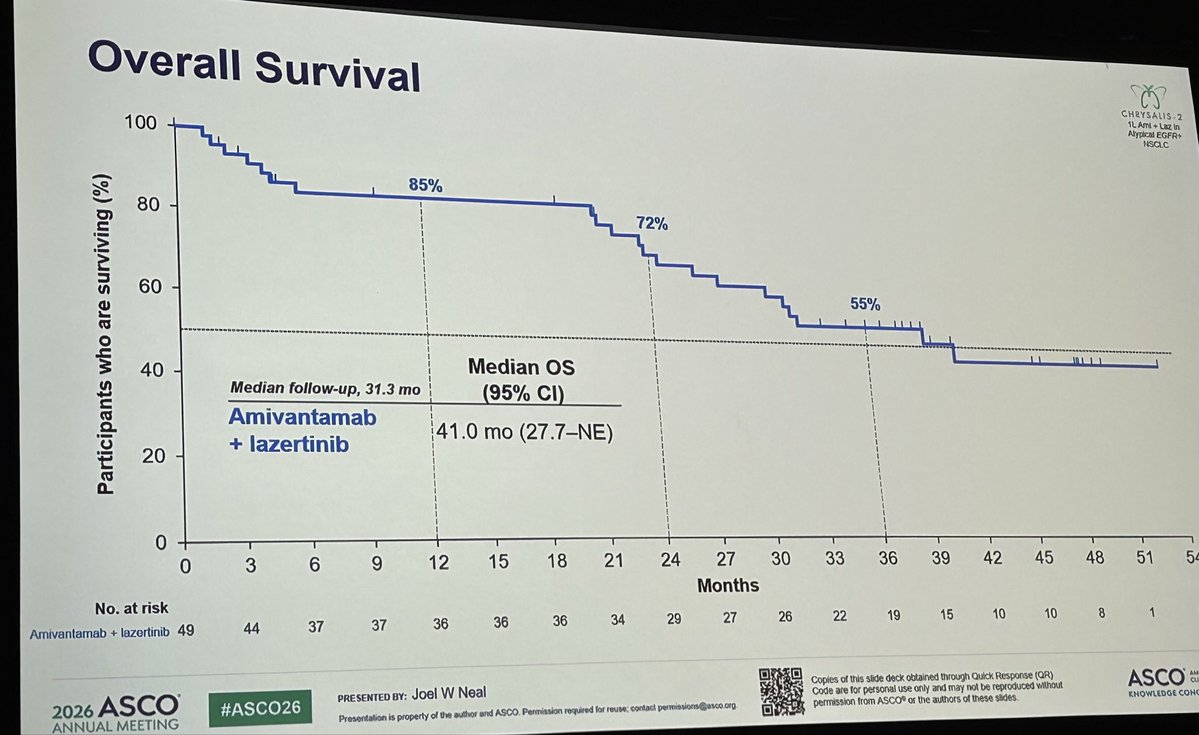
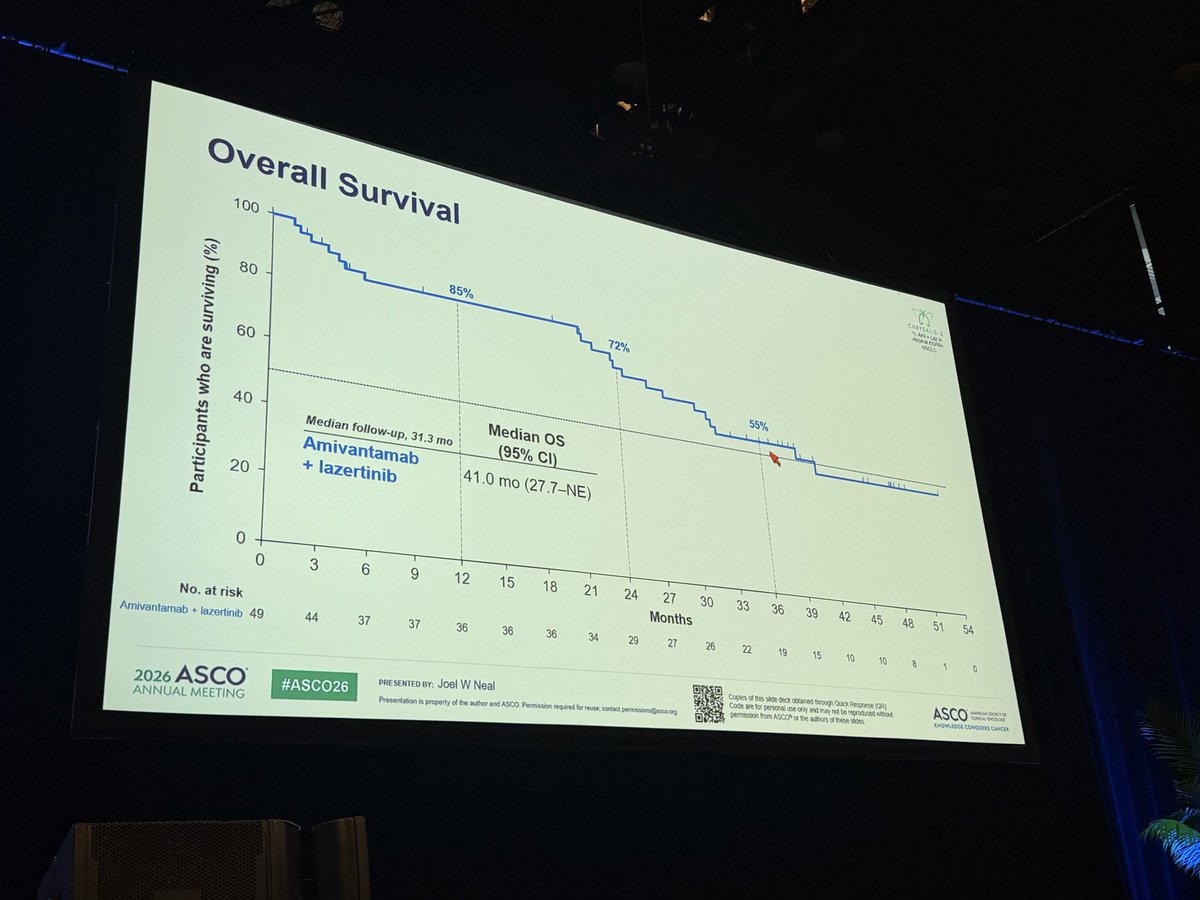
Overall survival — Median OS 41.0 months (95% CI 27.7-NE) at 31.3-month median follow-up (cutoff October 31, 2025); 3-year OS 55%, 4-year OS 46%. (ASCO 2026)
Safety — Consistent with prior amivantamab + lazertinib reports; no new safety signals on longer follow-up. (ASCO 2026)
Regulatory / Sponsor — INVESTIGATIONAL for atypical EGFR — not FDA approved in this population; Rybrevant + Lazcluze IS approved 1L for EGFR exon19del/L858R (MARIPOSA, Aug 2024). Johnson & Johnson. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.
Atypical
EETING
In CHRYSALIS-2
receive 1L amiva
Median age
Most freque
Compound 1
At a median follo
CBRe was 8
Median DoF
0
-20
Change in SoD of target
lesions (%)
-40
-60
-80
-100
Figure reused with permission from Toma
Participants may be counted in >1 categ
4 participants. CBR is defined as the per
1. Tomasini P, ot al. J Clin Oncol. 2026;4
2026 ASCO
#ASC
ANNUAL MEETING
2026
ASC
ANNUAL MEETI
---
CJ
Conclusions
CHRYSALIS 2
Atypical EGFR+
NSCLC
This single-arm study of amivantamab + lazertinib (n=49) in 1L atypical EGFR-mutated advanced NSCLC
demonstrates a clinically meaningful median os of ~3.5 years
Responses were durable regardless of demographics, baseline tumor mutations, and disease characteristics
With longer follow-up, the safety profile of IV amivantamab + lazertinib was consistent with prior reports¹,²,
with no new safety signals
Amivantamab + lazertinib as a 1L treatment has now shown durable survival
in both common and atypical EGFR-mutated advanced NSCLC
1. Tomanini P. at J Clin Oncol 2020 44(1).54- 2. Yang JCH, of a N Engl / Med. 2025,393(17) 1581-1693
2026 ASCO
PRE SENTED BY: Joel W Neal
Copies of his slide deck obtained through Quick Response (QR)
Code are for personal use only and may not be reproduced without
ASCO
AMERICAN ROCETY OF
CUPICAL OHCOLOGY
#ASCO26
ANNUAL MEETING
Presentation a property of the author and ASCO Permission required for - contact permissions@assoo.or org
permission from ASCO* or the authors of these sades
KNOWLEDGE CONQUERS CANCER
ASCO
ASCO
ASCO
ASCO
ASCO
AS
ASCO
ASC
ASCO
ASCO
ASCO
ASCO
CO
SC
ASCO
AS
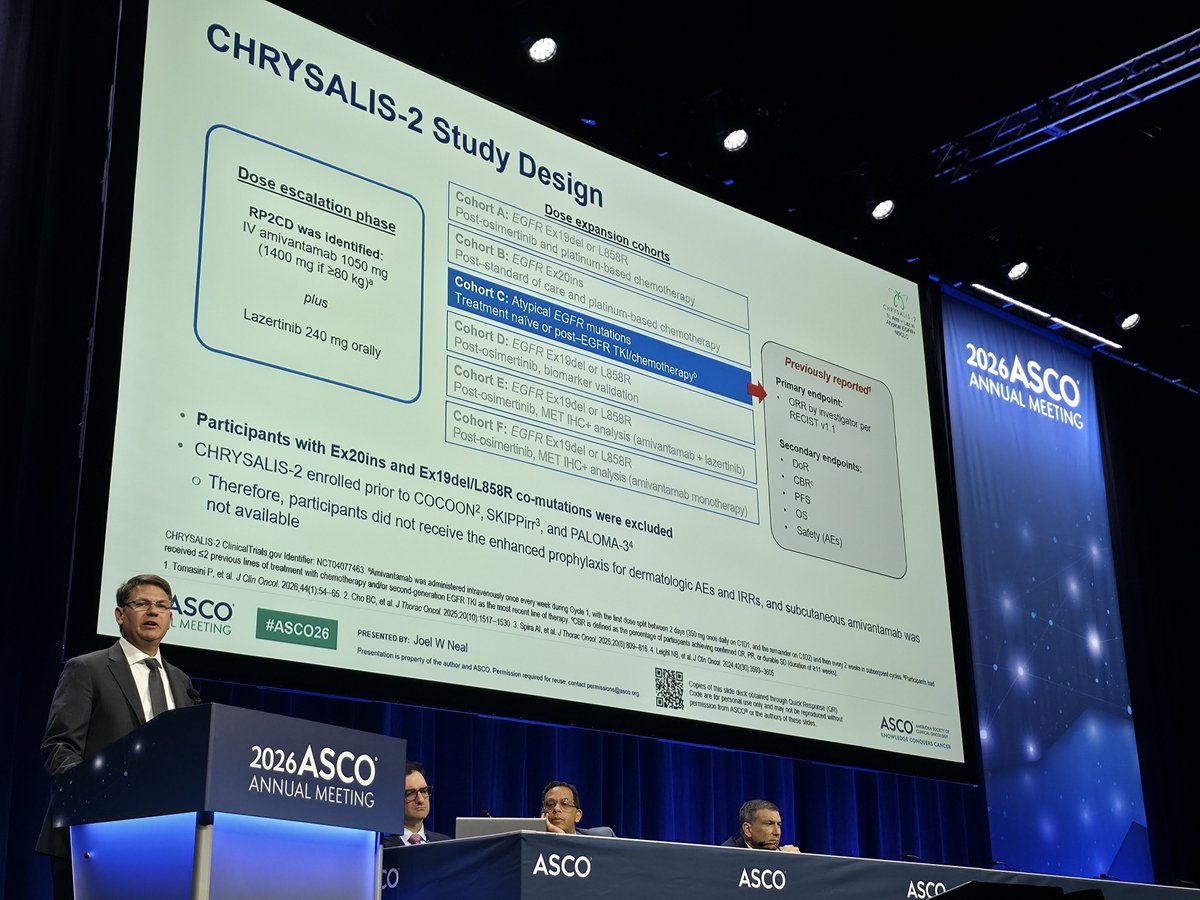
CHRYSALIS-2 Study Design
CHRYSACIS-2
esser
MOOLC
Dose expansion cohorts
Cohort A: EGFR Ex19del or L858R
Post-osimertinib and platinum-based chemotherapy
Cohort B: EGFR Ex20ins
Dose escalation phase
Post-standard - of care and platinum-based chemotherapy
Previously reported1
RP2CD was identified:
Cohort C: Atypical EGFR mutations
Primary endpoint:
IV amivantamab 1050 mg
Treatment naive or post-EGFR TKI/chemotherapy®
ORR by investigator per
(1400 mg if >80 kg)a
RECIST v1.1
Cohort D: EGFR Ex19del or L858R
plus
Post-osimertinib, biomarker validation
Secondary endpoints:
DoR
Cohort E: EGFR Ex19del or L858R
Lazertinib 240 mg orally
CBR
Post-osimertinib, MET IHC+ analysis (amivantamab + lazertinib)
PFS
Cohort F: EGFR Ex19del or L858R
OS
Post-osimertinib, MET IHC+ analysis (amivantamab monotherapy)
Safety (AEs)
Participants with Ex20ins and Ex19del/L858R co-mutations were excluded
CHRYSALIS-2 enrolled prior to COCOON2, SKIPPirr³, and PALOMA-34
Therefore, participants did not receive the enhanced prophylaxis for dermatologic AEs and IRRs, and subcutaneous amivantamab was
not available
Identifier: NCT04077463 Amivantamab was administered intravenously once every week during Cycle 1, with the as first the dose spit between of 2 days (350 achieving mg ance confirmed daily on C101, CR, PR, and of the durable remainder SD /duration on C C102) of 211 and weeks) then every 2 in subsequent cycles Participants had
CHRYSALIS-2 ClinicalTrials lines of gov treatment with chemotherapy and/or second-generation EGFR TKI as the most recent line of therapy. CBR is defined percentage participants Clin Oncol 2024,42(3) 3593-3605
received 1. Tomasini <2 P. previous et al. J Clin Oncol 2026;44(1):54-65. 2. Cho BC, of al. J Thorac Oncol 2025,20(10) 1517-1530 3 Spira Al, et al. J Thorac Oncol 2025,20(8) 809-816 4 Leight NB, d.
Copies of This as obtained through Quick Response OR)
ASCO
was
CHICA -
ASCO
PRESENTED BY: Joel W Neal
Code are for personal use only and may not be reproduced without
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco org
permission from ASCO® or the authors of these sides
ENQWLEDGE CONQUERS CANCER
#ASCO26
MEETING
2026ASCO
ANNUAL MEETING
ASCO
ASCO
ASCO
---
diographic Response With 1L Amivantamab + Lazertinib in
CHRYSALIS
Atypical EGFR-Mutated NSCLC1
NSCLC
2026
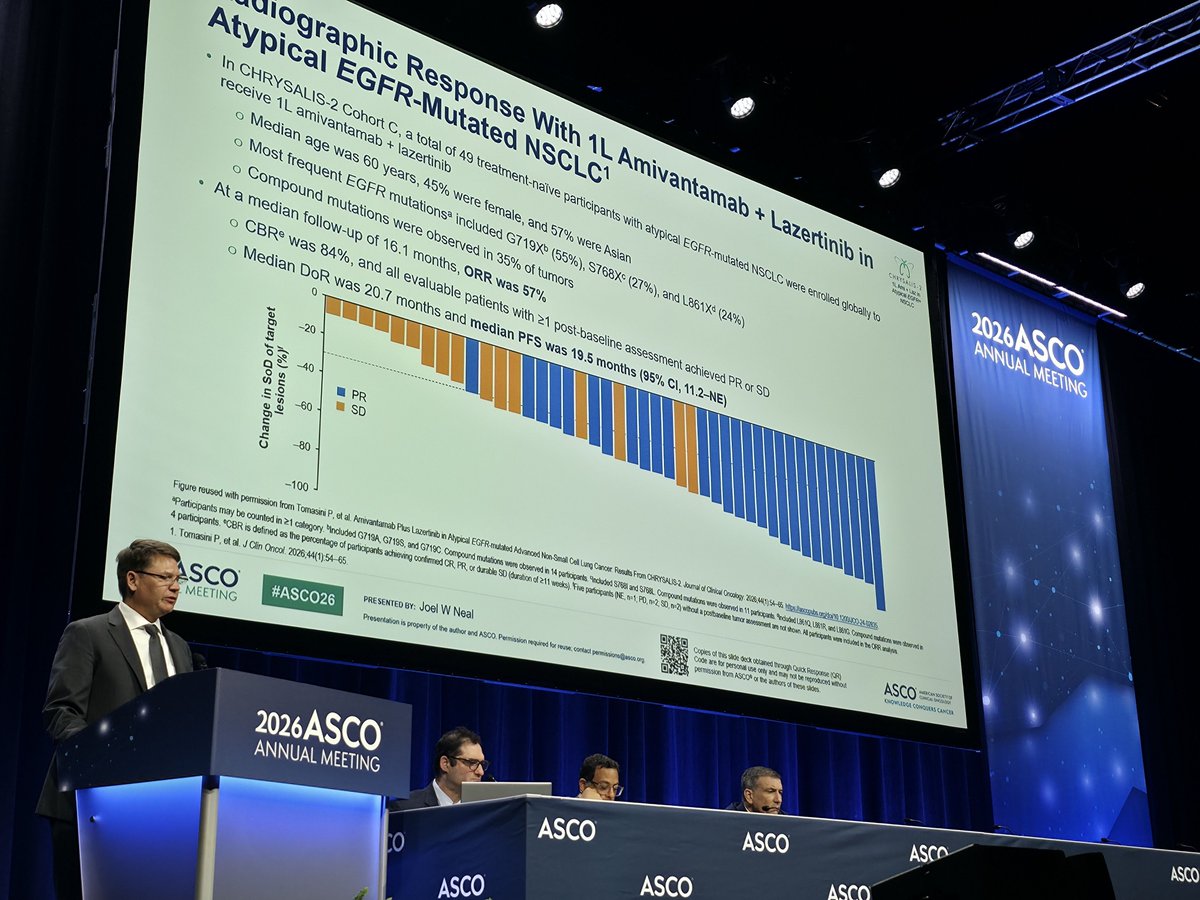
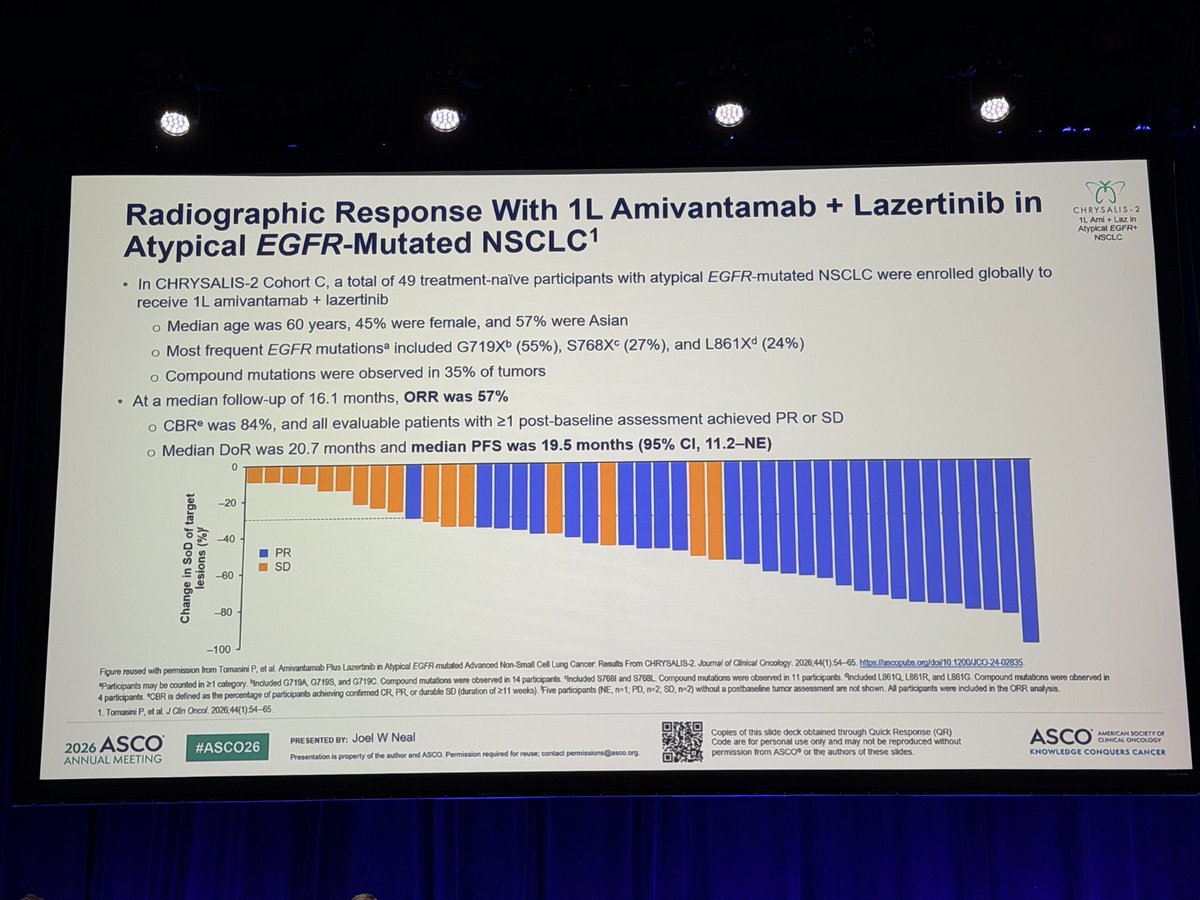
In CHRYSALIS-2 Cohort C, a total of 49 treatment-naïve participants with atypical EGFR-mutated NSCLC were enrolled globally to
ANNUA
receive 1L amivantamab + lazertinib
Median age was 60 years, 45% were female, and 57% were Asian
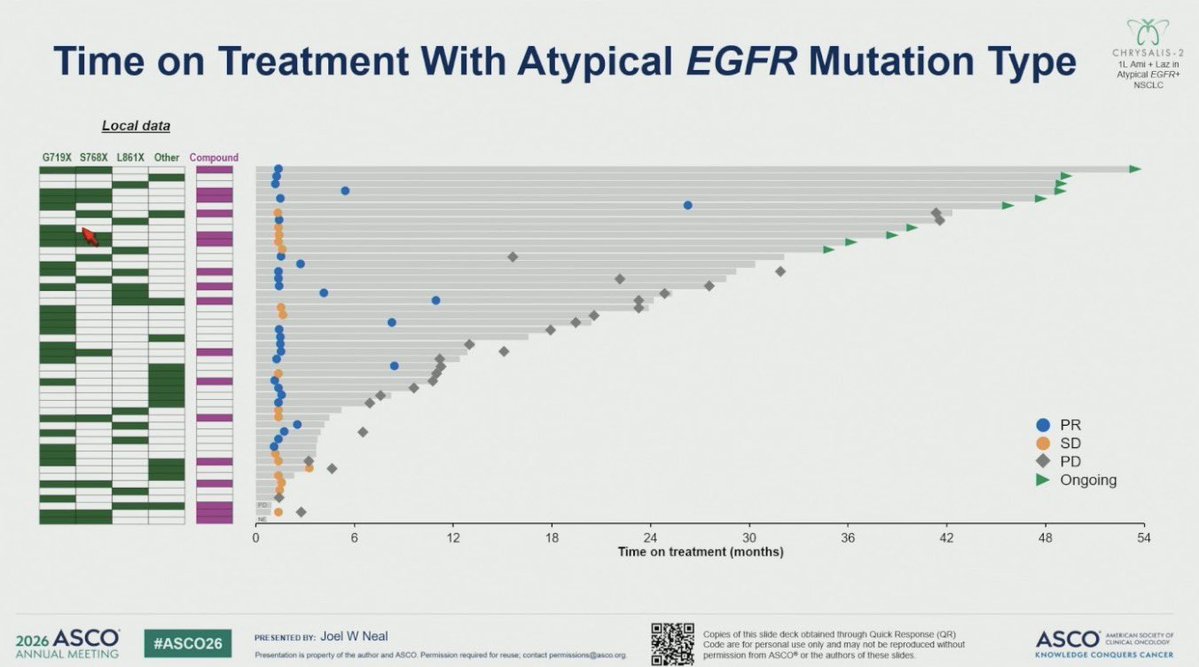
Most frequent EGFR mutations included G719Xb (55%), S768Xc (27%), and L861Xᵈ (24%)
Compound mutations were observed in 35% of tumors
At a median follow-up of 16.1 months, ORR was 57%
CBRe was 84%, and all evaluable patients with ≥1 post-baseline assessment achieved PR or SD
Median DoR was 20.7 months and median PFS was 19.5 months (95% CI, 11.2-NE)
0
-20
Change in SoD of target
lesions (%)
-40
PR
SD
-60
-80
Figure Participants reused may CBR with be permission IS counted defined in from as -100 21 the category Tomasini percentage Included P. et al of participants Amivantamab G719A G719S, achieving Plus and Lazertinib confirmed G719C in Compound CR Atypical PR, or EGFR mutations durable mutated SD were (duration Advanced observed 211 Non-Small in 14 weeks). participants Cell Five Lung participants included Cancer Results $7681 NE, at and From PD. S768L CHRYSALIS-2 n-2, Compound SD, n=2) without mutations Journal postbaseline of - Clinical observed Oncology fumor deck 11 atternment 2026,44(1) 54-6 participants obtained an through 9nduded L9E1Q not stown Quick Response participants L861R and LB6NG (QR) without - included e Compound be ASCO analysis -
I
Copies of TUS stide only and not be reproduced
CHOWLEDGE CONQUERS CANCER
4 1. participants. Tomasini P. J Clin Oncol 2026,44(1):54-65.
permission Code are for from personal ASCO* or the authors these sades.
SCO
#ASCO26
PRE Presentation property of he author and ASCO Permission required for reuse. contact
SENTED BY: Joel W Neal
MEETING
2026ASCO
ASCO
ANNUAL MEETING
ASCO
ASCO
ASCO
O
ASCÓ
ASCO
---
Overall Survival
CHRYSALIS-2
Anypical EGFA+
NOCLC
100
85%
80
72%
Participants who are surviving (%)
60
55%
Median os
40
Median follow-up, 31.3 mo
(95% CI)
Amivantamab
41.0 mo (27.7-NE)
+ lazertinib
20
0
18
21
24
27
30
33
36
39
42
45
48
51
54
0
3
6
9
12
15
Months
No. at risk
34
29
27
26
22
19
15
10
10
8
1
0
ivantamab lazertinib 49
44
37
37
36
36
36
Copies of this side deck obtained through Quick Response (QR)
ASCO
SINCAL exclusive
PRESENTED BY: Joel W Neal
Code are for personal use only and may not be reproduced whoul
KNOWLEDGE CONQUERS CANCER
ASCO
permission from ASCO* or the authors of these sides
#ASCO26
Presentation is property of the author and ASCO Permission required for contact permissions@asco org
AL MEETING
2026ASCO
ANNILIAL MEETING
---
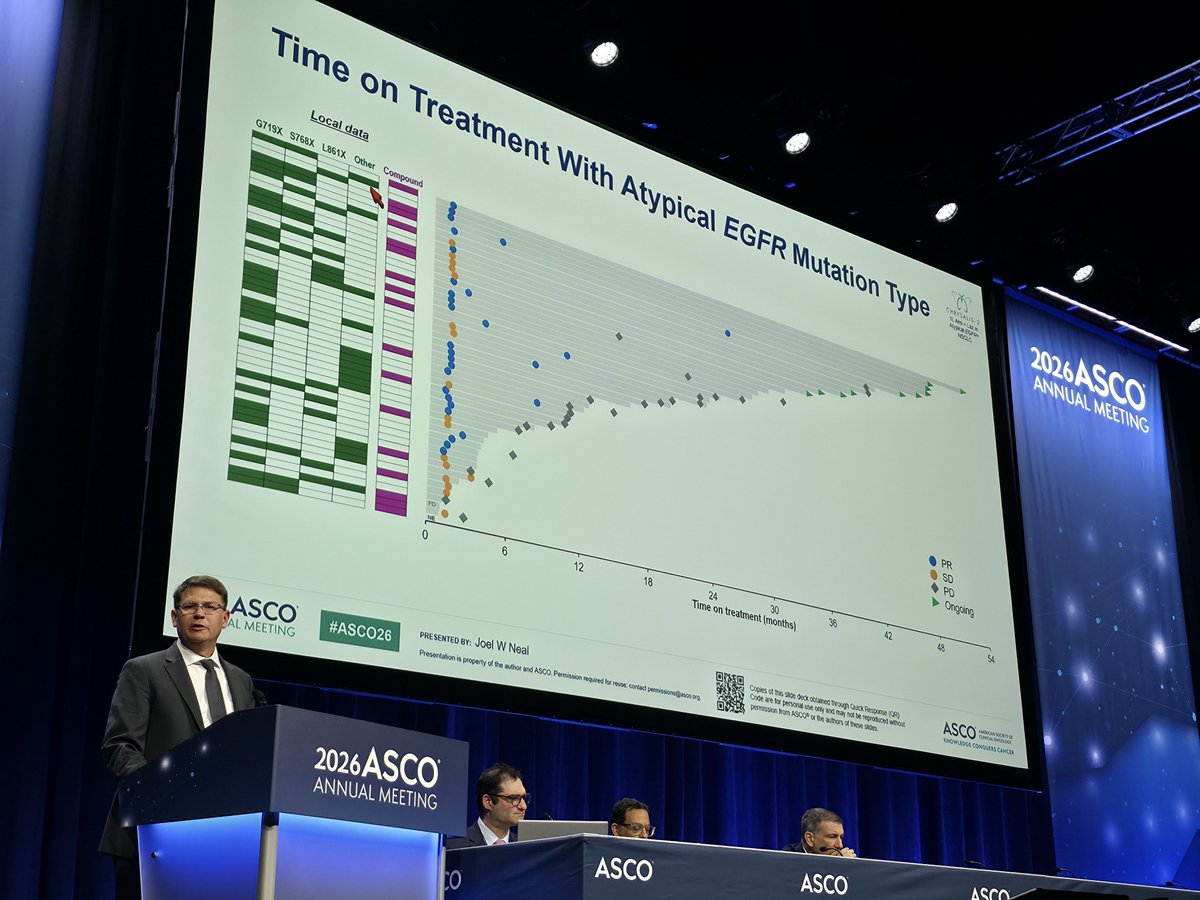
Time on Treatment With Atypical EGFR Mutation Type
CHRYSALIS-2
NSCLC
2020
Local data
ANN
G719X S768X L861X Other Compound
PR
SD
PD
Ongoing
PD
24
30
36
42
48
54
6
12
18
0
Time on treatment (months)
Copies of his slot deck obtained through Quick Response (QR)
ASCO
OREA
Code are for personal use only and may not be reproduced without
KNOWLEDGE CONQUERS CANCER
PRESENTED BY: Joel W Neal
permission bom ASCOR or the authors of these sades
ASCO
#ASCO26
Presentation is property of the author and ASCO. Permission required for reuse contact permissions@asco.org
AL MEETING
2026ASCO
ANNUAL MEETING
ASCO
ASCO
ASCO
ASCO
CHRYSALIS. 2
2026
Amt Laz in
Atypical EGFR*
ANNUAL MEETING
NSCLC
Overall survival of first-line amivantamab plus lazertinib
in atypical EGFR-mutated advanced NSCLC
Updated results from the CHRYSALIS-2 study
Joel W Neal1, Byoung Chul Cho², Yongsheng Wang³, Lin Wu⁴, Enriqueta Felip⁵, Jiuwei Cui⁶, Alexander I Spira⁷,
Melina E Marmarelis⁸, Eiki Ichihara⁹, Se-Hoon Lee¹⁰, James Chih-Hsin Yang¹¹, Sebastian Michels¹², Joshua C Curtin¹³,
Xuesong Lyu14, Zacharias Anastasiou¹⁵, Isabelle Leconte¹⁶, Leonardo Trani¹³, Sujay Shah¹³, Pascale Tomasini¹⁷
Stanford Cancer Institute, Stanford University, Stanford, CA USA Division of Medical Oncology, Yonsei Cancer Center, Yonsei University College of Medicine, Seoul, Republic of Korea, Division of Thoracic Tumor Multimodality Treatment,
Cancer Center and Clinical Trial Center, West China Hospital, Sichuan University, Chengdu, China; Department of Thoracic Medical Oncology, Hunan Cancer Hospital/The Affiliated Cancer Hospital of Xiangya School of Medicine, Central South
University, Changsha, China, Medical Oncology Service, Vall d'Hebron Institute of Oncology (VHIO), Vall d'Hebron Barcelona Hospital Campus, Universitat Autónoma de Barcelona, Barcelona, Spain; The First Hospital of Jilin University,
Changchun, China Virginia Cancer Specialists, Fairfax, VA, USA; Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA, Center for Clinical Oncology, Okayama University Hospital, Okayama, Japan, Samsung
Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea, "National Taiwan University Cancer Center, Taipei, Towan, Department I for Internal Medicine, Faculty of Medicine and University Hospital Cologne,
Lung Cancer Group Cologne, Center for Integrated Oncology Aachen Koin Bonn Düsseldorf, University of Cologne, Cologne, Germany, "Johnson & Johnson, Spring House, PA, USA; "Johnson & Johnson, Shanghai, China,
"Johnson & Johnson, Alhers, Greece, "Johnson & Johnson, Allschwil, Switzerland "Aix Marseille University - CNRS, INSERM, CRCM, CEPCM- AP-HM Hôpital de la Timone, Marseille, France
2026 ASCO
#ASCO26
PRE SENTED BY: Joel W Neal
Copies of this Mde deck obtained through Quick Response (QR)
ANNUAL MEETING
ASCO
AMERICA MN SOCIETY of
Code are for personal use only and may not be reproduced without
CLINICAL ONCOLOGY
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@esico.or
permission from ASCO or the authors of these sides.
KNOWLEDGE CONQUERS CANCER
in atypical EGFR-mutated advanced NSCLC
Updated results from the CHRYSALIS-2 study
---
CHRYSALIS 2
CHRYSALIS-2 Study Design
1L Amt Laz in
Atypical EGFR+
NSCLC
Dose expansion cohorts
Cohort A: EGFR Ex19del or L858R
Post-osimertinib and platinum-based chemotherapy
Cohort B: EGFR Ex20ins
Previously reported1
Dose escalation phase
Post-standard of care and platinum-based chemotherapy
Primary endpoint:
RP2CD was identified:
Cohort C: Atypical EGFR mutations
ORR by investigator per
IV amivantamab 1050 mg
Treatment naïve or post-EGFR TKI/chemotherapyᵇ
RECIST v1.1
(1400 mg if >80 kg)ᵃ
Cohort D: EGFR Ex19del or L858R
plus
Post-osimertinib, biomarker validation
Secondary endpoints:
DoR
Lazertinib 240 mg orally
Cohort E: EGFR Ex19del or L858R
CBRc
Post-osimertinib, MET IHC+ analysis (amivantamab + lazertinib)
PFS
Cohort F: EGFR Ex19del or L858R
OS
Post-osimertinib, MET IHC+ analysis (amivantamab monotherapy)
Safety (AEs)
Participants with Ex20ins and Ex19del/L858R co-mutations were excluded
CHRYSALIS-2 enrolled prior to COCOON², SKIPPirr³, and PALOMA-34
Therefore, participants did not receive the enhanced prophylaxis for dermatologic AEs and IRRs, and subcutaneous amivantamab was
not available
CHRYSALIS-2 ClinicalTrials gov identifier: NCT04077463 "Amivantamab was administered intravenously once every week during Cycle 1, with the first dose split between 2 days (350 mg once daily on C1D1, and the remainder on C102) and then every 2 weeks in subsequent cycles. Participants had
received 52 previous lines of treatment with chemotherapy and/or second generation EGFR TKI as the most recent line of therapy. CBR is defined as the percentage of participants achieving confirmed CR, PR, or durable SD (duration of 211 weeks).
1.
Tomasini P. et al. Clin Oncol 2026;44(1).54-65. 2 Cho BC, et al. J Thorac Oncol. 2025,20(10):1517-1530. 3. Spira Al, et al. J Thorac Oncol 2025;20(6) 809-816. 4. Leight NB, etal.J Clin Oncol 2024,42(30),3593-3605
2026 ASCO
PRESENTED BY: Joel W Neal
Copies of this slide deck obtained through Quick Response (QR)
Code are for personal use only and may not be reproduced without
ASCO
AMERICAN SOCIETY OF
#ASCO26
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse; contact permissions@asco.org.
permission from ASCO or the authors of these slides
KNOWLEDGE CONQUERS CANCER
CO
HRYSALIS-2 Study Design
2026ASCO
ANNUAL MEETING
CHRYSALIS-2 Study Design
If
Statement
Detert
---
Overall Survival
CHRYSALIS-2
Адурісай EGFR+
NSCLC
100
85%
80
72%
Participants who are surviving (%)
60
55%
40
Median os
Median follow-up, 31.3 mo
(95% CI)
Amivantamab
41.0 mo (27.7-NE)
+ lazertinib
20
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
Months
No. at risk
Amivantamab lazertinib 49
44
37
37
36
36
36
34
29
27
26
22
19
15
10
10
8
1
0
PRESENTED BY: Joel W Neal
Copies of this sade deck obtained through Quick Response (QR)
ASCO
AMERICAN SOURTY CR
2026 ASCO
#ASCO26
Code are for personal use only and may not be reproduced without
CLAIM OHCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco. org
permission from ASCO or the authors of these sides
KHOWLEDGE CONQUERS CANCER
---
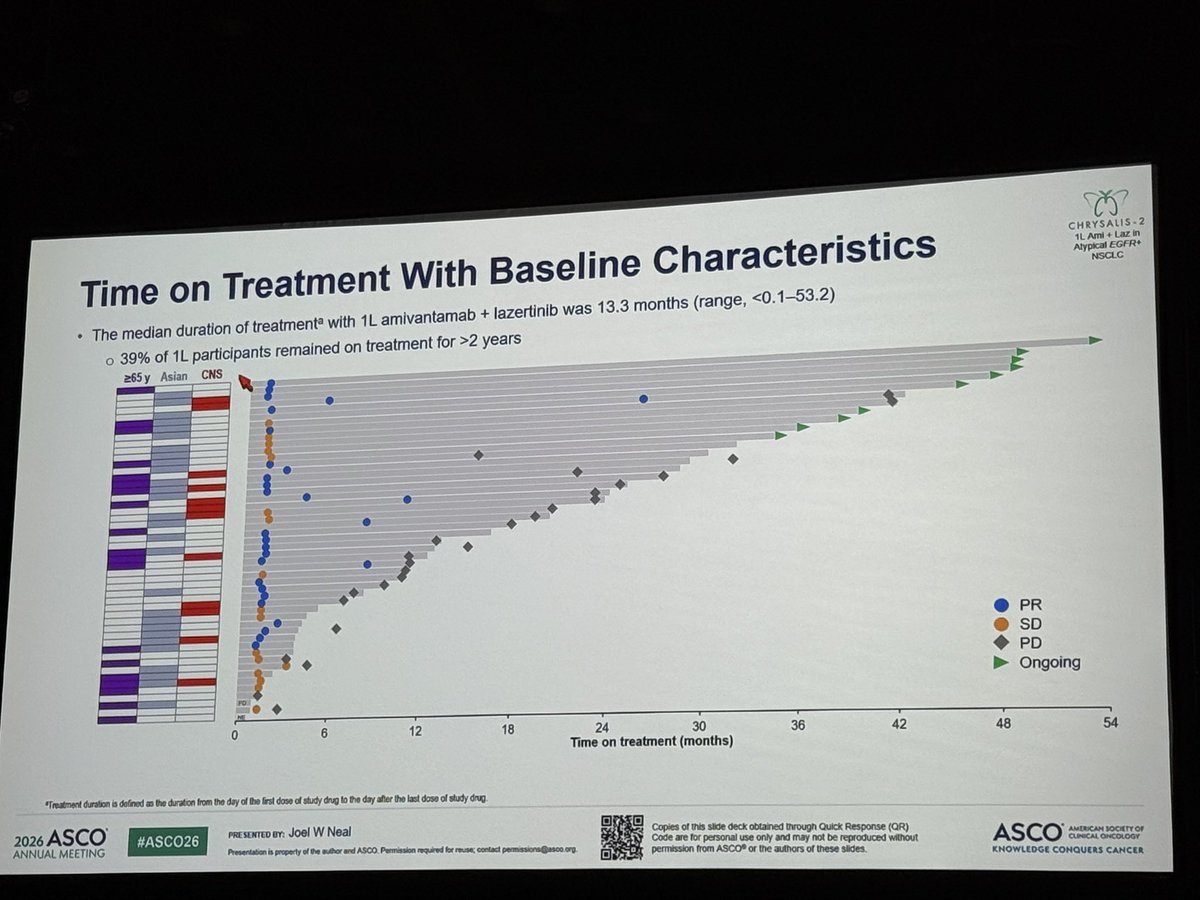
Time on Treatment With Baseline Characteristics
CHRYSALIS-2
1LAml LIZ in
Adypical EGFR+
NSCLC
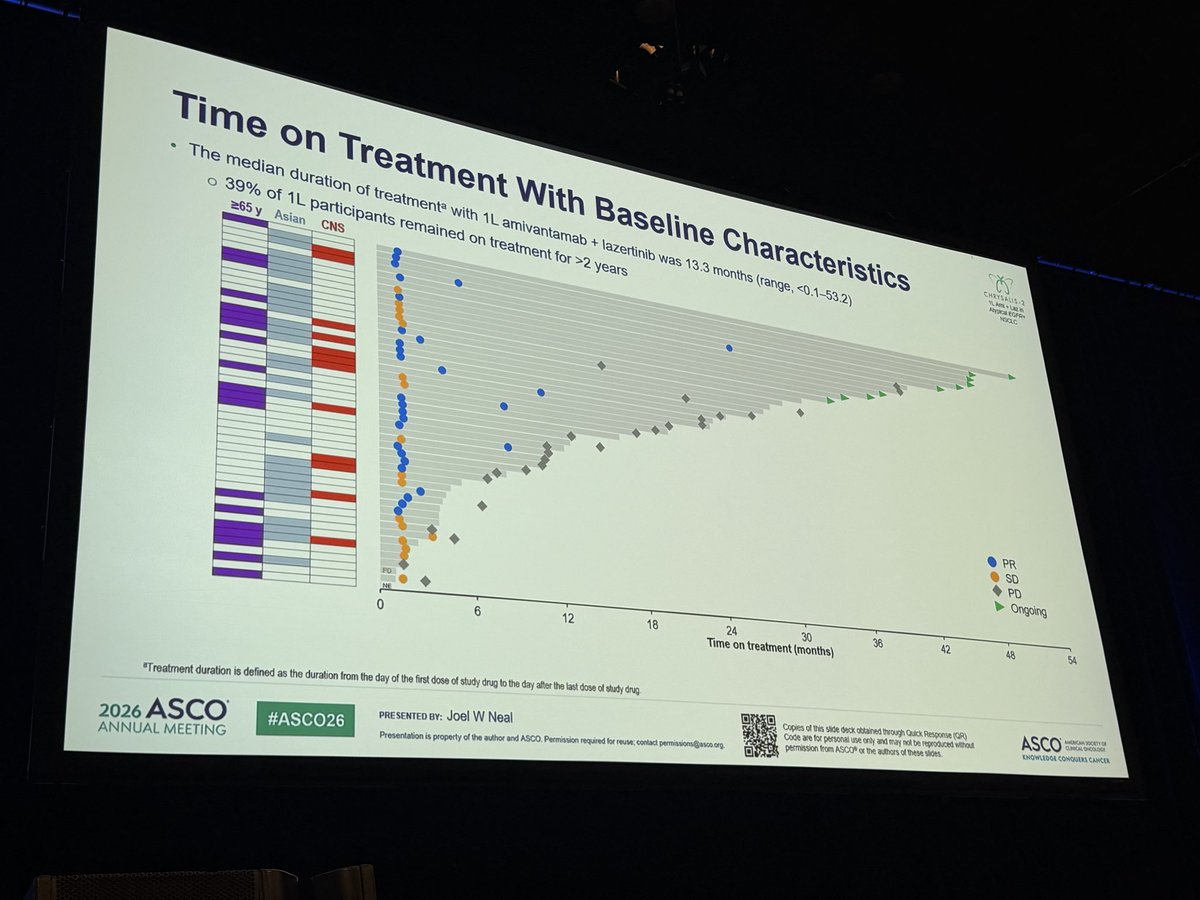
The median duration of treatmentᵃ with 1L amivantamab + lazertinib was 13.3 months (range, <0.1-53.2)
39% of 1L participants remained on treatment for >2 years
>65 y Asian CNS
PR
SD
PD
Ongoing
FOR
12
18
24
30
36
42
48
54
0
6
Time on treatment (months)
"Treatment duration is defined as the duration from the day of the first dose of study drug to the day after the last dose of study drug
Copies of this slide deck obtained through Quick Response (QR)
ASCO
AMERICAN SOCIETY OF
CUMICAL DHCOLDER
PRESENTED BY: Joel W Neal
Code are for personal use only and may not be reproduced without
2026 ASCO
KNOWLEDGE CONQUERS CANCER
#ASCO26
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco.org
permission from ASCO or the authors of these slides
ANNUAL MEETING
Frontline phase III trials for EGFR exon 20 insertions
PAPILLON (n=308)
EXCLAIM-2 (n=354)
WU-KONG 28 (n=324)
Arms
Amivantamab+chemo V
Mobocertinib V chemotherapy
Sunvozertinib V chemotherapy
chemotherapy
Drug
Bispecific lgG antibody
Pyrimidine-based small molecule
Pyrimidine-based small molecule
Dosing
iv/subcut q3 weekly
Oral, daily
Oral, daily (300 mg)
Patient
Brain mets: 23% V 23%
Brain mets: 33% V 31%
Brain mets: 12.9 V 12.4%
characteristics
Never smoker: 58 V 59%
Never smoker: 54% V 61%
Never smoker: 62 V 66.5%
Efficacy
ORR: 73% V 47%
ORR: 32% V 30%
ORR: 58.8% V 31.1%
PFS: 11.4 V 6.7 m
PFS: 9.6 V 9.6 m
PFS: 10.3 V 7.5 m
DoR: 9.7 V 4.4 m
DoR: 12.0 V 8.4 m
DoR: 11.2 V 7.1 m
Toxicities
Neutropenia: 59%/33%
Diarrhoea: 96%/ 20%
Diarrhoea: 84%/13.5%
(All grades/ G3)
Paronychia: 56%/7%
Paronychia: 47%/ 1%
Rash: 51.5%/0.6%
Rash: 54%/ 11%
Stomatitis: 40%/ 4%
Anaemia: 46%/ 6.1%
Stomatitis: 25%/ 1%
Acneiform rash: 35%/1%
CPK increase 55.2%/20.2%
Paronychia: 48.5%/3.7%
Dose interruption: 64%
Dose interruption: 70%
Dose reduction: 36%
Dose reduction: 45%
Drug interruption: 45.4%
Discontinuation: 11%
Discontinuation: 18%
Dose reduction: 40.5%
Discontinuation: 7.4%
Girard NEJM 2023; Janne JCO 2025; Heymach ASCO 2026
026 ASCO
PRE SENTED BY: Daniel SW Tan, National Cancer Centre Singapore
ASCO
AMERICAN SOCIETY OF
#ASCO26
CLINICAL CHEDLOGY
NNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco
KNOWLEDGE CONQUERS CANCER
---
Therapeutic advances in EGFR ex20 ins mutations
-
-
EXCLAIM
EXCLAIM-2
Accelerated approval
PFS adents
-
-
"
Mobocertinib vs
-
mobocertinib
Chemo
-
Structural basis
PFS: 9.6 V 9.6 m
.
,
4
.
"
"
.
11
24
If
-
a
resistance to 1G
Time months)
EGFR TKI in Ex20
CHRYSALIS
insertions
Accelerated approval
Roubichoux et al.
WU-KONG 1B
Yasuda STM 2013
- amivantamab
Structural-functional
Accelerated approval
(monotherapy)
basis classification
- Sunvozertinib 200 mg
2013
2015
2017
2019
2021
2023
2024
2025
2026
Yang et al. Role of
Osimertinib 160 mg OM
PAPILLON
FAVOUR
WU-KONG 28
afatinib in uncommon
POSITION20
SoC chemo-
Firmonertinib
Phase III
mutations (LUX-2,
ORR 28%, mPFS 6.8 m
amivantamab
ORR 78,6%
Sunvozertinib 300 mg
LUX-3, LUX-6)
- - 3 cohorts: Exon 20
ECOG ACRIN EA5162
mDoR 15.2 m
vs chemo
A handred, blinded Independent Central
ins/atypicals/ T790M
ORR 24%, mPFS 9.6 m
to
Patients
Limited efficacy for
10
14-7.21
afatinib in exon 20 ins
#
-
is
35-4
12
is
is
n
24
Henths
- -
($)
us
-
N
-
0
0
1
:
-
1
as
an
24
42
14
4
I
a
6
2026 ASCO
PRE SENTED BY: Daniel SW Tan, National Cancer Centre Singapore
ASCO
AMERICAN SOCIETY OF
#ASCO26
CLINICAL CHCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse contact permissions@asco
KNOWLEDGE CONQUERS CANCER
---
Upfront RT did not reduce intracranial PFS
Intracranial PFS
PFS
Overall survival
UPPRONT RT + Delayed RT
State - UPFRONT AT - Delayed RT
- UPPRONT RT - Delayed ST
16
1.0
1.0
Protosty OF
OD
0.8
Cumulative Survival Probability
0.8
04
Cumulative Survival Probability
0.8
06
06
04
0.4
0.2
0.2
0.2
0
0
12
11
24
30
30
00
00
Time months
0
6
12
18
24
30
30
Time months
0
6
12
18
24
30
30
Number et risk
Time months
135
87
85
37
26
15
7
Number risk
Number at nuk
DONNERS
103
47
53
32
22
12
$
"
30
Strata
UPFRONCE
105
87
65
37
26
15
7
.
C
21
X
&
103
87
55
32
22
12
8
UPPRONT #1
105
10
71
45
34
23
14
Time months
9
1
4
4
24
30
XI
Delivery
103
R
74
59
41
25
17
Time months
0
$
Q
0
H
#
.
Time months
Median icPFS 18.2 V 14.8 m
Median PFS 12.7 V 12.0 m
Median os 23.3 V 28.7 m
HR 0.82 (0.59 — 1.16) p 0.26
HR 1.05 (0.76 — 1.44) 0.75
HR 1.45 p 0.07
Treatment
0.70
Delayed RT
-
UPFRONT RT
0.65
0.00
Upfront RT (n=105)
Delayed RT (n=103)
Intracranial progression
111
0.50
Cumutative Incidence
0.45
Number of Events
20
47
"death as competing event
0.40
0.33
1-year
0.30
8.7% 2.9%,14.5%)
25.7% (16.8%,34.7%)
0.23
[exploratory analysis]
0.23
2-years
21.7% (12.6%,30.8%)
50% (39.2%,60.9%)
013
0.12
0.03
Sub-HR(95% CI)
0.35(0.21,0.59)
p-value = <0.001
0.00
0
6
12
11
24
30
%
Time (months)
26 ASCO
PRESENTED BT: Daniel SW Tan, National Cancer Centre Singapore
#ASCO26
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
NUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco org
With death as a competing event CONQUERS CANCER
---
Expanding role of high-quality clinical registries for HTA
assessments especially in rare diseases
Median as
(95% C)
100
Amirantamab isrertinio
Median os
Physician selected CFR- TIO
19.6 m (5.6-52.7)
(95% Ca
Amivantamab lazertinit
41.0 mo (27.7-NE)
(%) Participants 1 :
100
75
Physician-sected EGFRTIO
75
Anivartanch
25
Physician-selet (CFR no
Patients who are alive (%)
-
50
Anivantamab lazertinis
-
50
Median follow-up:
25
Amivantamab 31.3mg
Physician selected (CFIL TX)
Physician-selected CFR TXL 124mg
0
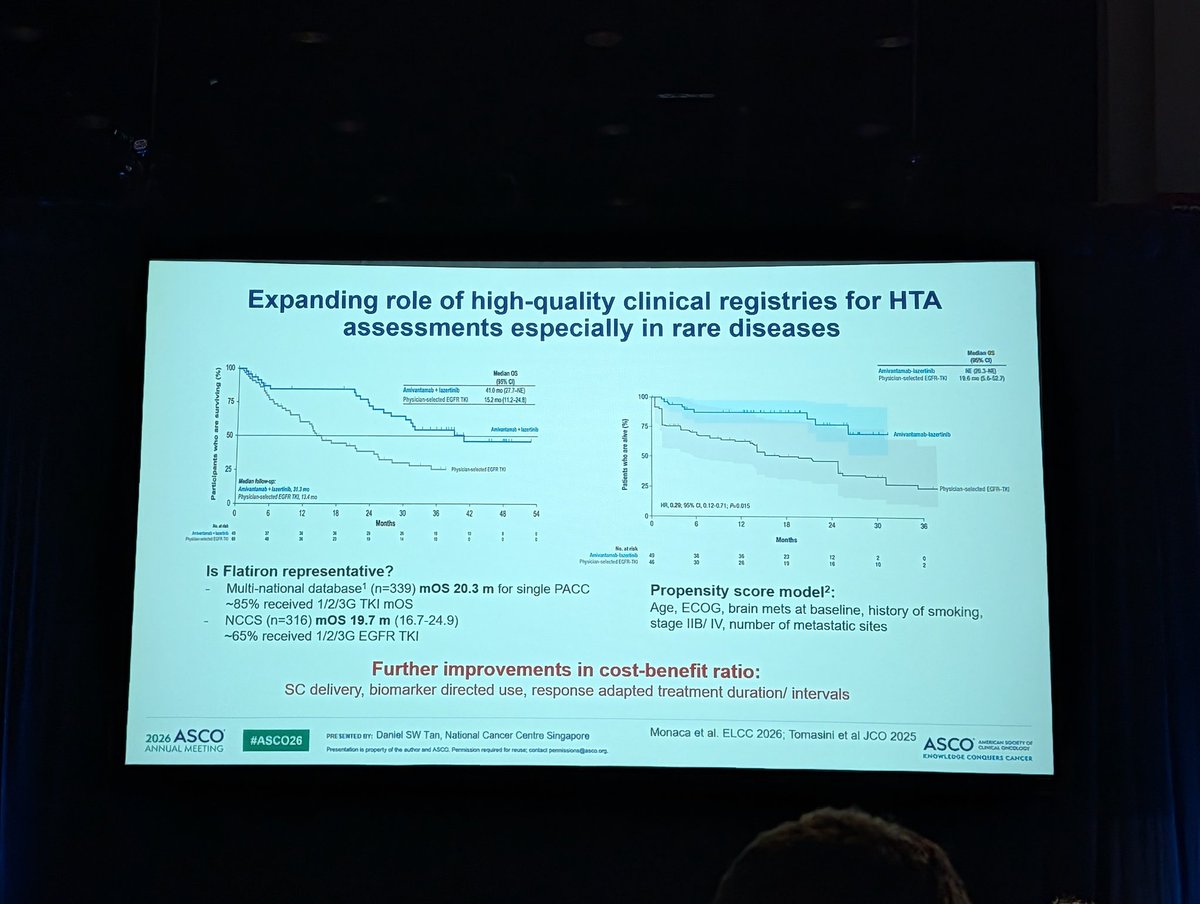
HR,0.29, 95% a 0.12-071; Pv0.015
0
6
12
18
24
30
36
42
48
54
0
Months
0
6
12
18
24
30
36
-
I I
:
:
:
:
:
:
:
:
:
Months
No. at eisk
Amixantamob questions
43
34
36
23
12
2
c
Physician-selected 50
45
8
21
19
16
10
2
Is Flatiron representative?
-
Multi-national database¹ (n=339) mos 20.3 m for single PACC
Propensity score model²:
~85% received 1/2/3G TKI mOS
Age, ECOG, brain mets at baseline, history of smoking,
-
NCCS (n=316) mOS 19.7 m (16.7-24.9)
stage IIB/ IV, number of metastatic sites
~65% received 1/2/3G EGFR TKI
Further improvements in cost-benefit ratio:
SC delivery, biomarker directed use, response adapted treatment duration/ intervals
2026 ASCO
PRE SENTED BY Daniel SW Tan, National Cancer Centre Singapore
Monaca et al. ELCC 2026; Tomasini et al JCO 2025
#ASCO26
ASCO
AMERICAN SQOETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse contact pennissions@asco.org
KNOWLEDGE CONQUERS CANCER
2026ASCO
ANNUAL MEETING
AS
---
Radiographic Response With 1L Amivantamab + Lazertinib in
CHRYSALIS
1L Ami Laz in
Atypical EGFR-Mutated NSCLC1
Atypical EGFR+
NSCLC
In CHRYSALIS-2 Cohort C, a total of 49 treatment-naïve participants with atypical EGFR-mutated NSCLC were enrolled globally to
receive 1L amivantamab + lazertinib
Median age was 60 years, 45% were female, and 57% were Asian
Most frequent EGFR mutations included G719Xb (55%), S768Xc (27%), and L861Xd (24%)
Compound mutations were observed in 35% of tumors
At a median follow-up of 16.1 months, ORR was 57%
CBRe was 84%, and all evaluable patients with ≥1 post-baseline assessment achieved PR or SD
Median DoR was 20.7 months and median PFS was 19.5 months (95% CI, 11.2-NE)
0
-20
Change in SoD of target
lesions (%)
-40
PR
SD
-60
-80
-100
Figure reused with permission from Tomasini P. et al Amivantamab Plus Lazertinib in Atypical EGFR mutated Advanced Non Small Cell Lung Cancer Results From CHRYSALIS-2 Journal of Clinical Oncology 2026,44(1):54-65 https://ascopabs.org/doi/10 1200/JCO-24-02835
Participants may be counted in 21 category "Included G719A G7198 and G719C Compound mutations were observed in 14 participants 'Included S7681 and S768L Compound mutations were observed in 11 participants included L861Q L861R and LB61G Compound mutations were observed
in
4 participants "CBR is defined as the percentage of participants achieving confirmed CR PR, or durable SD (duration of 211 weeks) Five participants (NE, n=1, PD, n=2 SD. n=2) without a postbaseline tumor assessment are not shown All participants were included in the ORR analysis
1. Tomasini P. of al J Clin Oncol 2026;44(1) 54-65
2026 ASCO
PRE SENTED BY: Joel W Neal
Copies of this stide deck obtained through Quick Response (QR)
#ASCO26
ASCO
AMERICAN SOCIETY OF
Code are for personal use only and may not be reproduced without
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@as.co.org
permission from ASCO* or the authors of these slides
KNOWLEDGE CONQUERS CANCER
---
Overall Survival
CH
1L
Aty
100
85%
80
72%
Participants who are surviving (%)
60
55%
Median os
40
Median follow-up, 31.3 mo
(95% CI)
Amivantamab
41.0 mo (27.7-NE)
+ lazertinib
20
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
5
Months
No. at risk
Amivantamab lazertinib 49
44
37
37
36
36
36
34
29
27
26
22
19
15
10
10
8
1
0
2026 ASCO
PRESENTED BY: Joel W Neal
Copies of this slide deck obtained through Quick Response (QR)
Code are for personal use only and may not be reproduced without
ASCO
AMERICA
#ASCO26
CUNICA
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
permission from ASCO* or the authors of these stides
KNOWLEDGE CONQUE
---
Time on Treatment With Atypical EGFR Mutation Type
CHRYSALIS 2
1L Amt Laz in
Atypical EGFR+
NSCLC
Local data
G719X S768X L861X Other Compound
PR
SD
PD
Ongoing
0
6
12
18
24
30
36
42
48
54
Time on treatment (months)
2026 ASCO
PRE SENTED BY: Joel W Neal
Copies of this slide deck obtained through Quick Response (QR)
ASCO
AMERICAN SOCIETY OF
#ASCO26
Code are for personal use only and may not be reproduced without
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
permission from ASCO* or the authors of these slides
KNOWLEDGE CONQUERS CANCER
CHRYSALIS 2
Overall Survival
1L Ami Laz in
Alypical EGFR+
NSCLC
100
85%
80
72%
Participants who are surviving (%)
60
55%
Median os
40
Median follow-up, 31.3 mo
(95% CI)
Amivantamab
41.0 mo (27.7-NE)
+ lazertinib
20
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
Months
No. at risk
vantamab . lazertinib 49
44
37
37
36
36
36
34
29
27
26
22
19
15
10
10
8
1
0
2026 ASCO
PRESENTED BY: Joel W Neal
Copies of this slide deck obtained through Quick Response (QR)
Code are for personal use only and may not be reproduced without
ASCO
AMERICAN SOCIETY OF
#ASCO26
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco org.
permission from ASCO® or the authors of these slides.
KNOWLEDGE CONQUERS CANCER
---
Time on Treatment With Baseline Characteristics
CHRYSALIS. 2
1L Ami Laz in
Atypical EGFR+
NSCLC
The median duration of treatmentᵃ with 1L amivantamab + lazertinib was 13.3 months (range, <0.1-53.2)
39% of 1L participants remained on treatment for >2 years
≥65y Asian CNS
PR
SD
PD
Ongoing
0
6
12
18
24
30
36
42
48
54
Time on treatment (months)
"Treatment duration is defined as the duration from the day of the first dose of study drug to the day after the last dose of study drug.
2026 ASCO
PRESENTED BY: Joel W Neal
Copies of this slide deck obtained through Quick Response (QR)
#ASCO26
ASCO
AMERICAN SOCIETY OF
Code are for personal use only and may not be reproduced without
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asoo org.
permission from ASCO or the authors of these slides,
KNOWLEDGE CONQUERS CANCER
---
CHRYSA
Conclusions
1L Ami +
Atypical 1
NSC
This single-arm study of amivantamab + lazertinib (n=49) in 1L atypical EGFR-mutated advanced NSCLC
demonstrates a clinically meaningful median os of ~3.5 years
Responses were durable regardless of demographics, baseline tumor mutations, and disease characteristics
With longer follow-up, the safety profile of IV amivantamab + lazertinib was consistent with prior reports¹,²,
with no new safety signals
Amivantamab + lazertinib as a 1L treatment has now shown durable survival
in both common and atypical EGFR-mutated advanced NSCLC
Tomasini P, of al. J Clin Oncol 2026;44(1):54-65. 2. Yang JCH, et of Engl / Med. 2025,393(17) 1681-1693
ASCO
PRESENTED BY: Joel W Neal
#ASCO26
Copies of this slide deck obtained through Quick Response (QR)
Code are for personal use only and may not be reproduced without
ASCO
AMERICAN SO
CLINICAL ONC
---
Also at ASCO 2026
CHRY
1L Am
Atypic
NS
May 30th 9:00am-12:00pm
May 31st 8:00am-11:00am
Gastrointestinal Cancer - Colorectal and Anal
Head and Neck Cancer
Poster Session: Hall A
Oral Abstract Session: S100a
Abstract 3548
RIGAMI-1
Abstract 6008
Poster board 315
RIGAMI-4
Oral presentation
Antitumor activity of amivantamab by consensus
Amivantamab in HPV-unrelated R/M HNSCC after disease
molecular subtypes in RAS/RAF WT mCRC
progression on checkpoint inhibitor and chemotherapy
(M Cruz-Correa)
(B Burtness)
May 30th 1:30pm-4:30pm
May 31st 9:00am-12:00pm
Head and Neck Cancer
Lung Cancer - Non-Small Cell Metastatic
Poster Session: Hall A
Poster Session: Hall A
Abstract 6038; Poster board 495
Abstract 8613; Poster board 403
Real-world treatment patterns and overall survival
in R/M HNSCC following treatment with ICI
SC amivantamab + lazertinib with
and platinum-based chemotherapy (AJ Rosenberg)
supportive care in 1L EGFRm
COPERNICUS
advanced NSCLC (SB Goldberg)
Trial in progress:
RIGAMI-5
Abstract TPS6127
Abstract 8614; Poster board 404
Poster board 583a
SC amivantamab + pembrolizumab + carboplatin VS
SC amivantamab + chemotherapy with
5-FU + pembrolizumab + cisplatin/carboplatin in 1L R/M
COPERNICUS
enhanced dermatologic AE prophylaxis in
HNSCC (RI Haddad)
2L EGFRm advanced NSCLC (T Leal)
SCO
#ASCO26
PRESENTED BY: Joel W Neal
Copies of this slide deck obtained through Quick Response (QR)
EETING
Presentation is property of the author and ASCO. Permission required for reuse; contact permissions@asco.org
Code are for personal use only and may not be reproduced without
ASCO
AMERICAN
CLINICAL Of
permission from ASCO® or the authors of these slides.
KNOWLEDGE CONQUERS
Overall Survival
CHRYSALIS 2
1L Aml Laz in
Alypical EGFR+
100
NSCLC
85%
80
72%
Participants who are surviving (%)
60
55%
40
Median os
Median follow-up, 31.3 mo
(95% CI)
Amivantamab
41.0 mo (27.7-NE)
+ lazertinib
20
0
15
18
21
24
27
30
33
36
39
42
45
48
51
54
0
3
6
9
12
Months
No. at risk
37
36
36
36
34
29
27
26
22
19
15
10
10
8
1
Amivantamab + lazertinib 49
44
37
Copies of this slide deck obtained through Quick Response (QR)
ASCO 33
2026 ASCO
PRESENTED BY: Joel W Neal
Code are for personal use only and may not be reproduced without
KNOWLEDGE CONC
#ASCO26
permission from ASCO or the authors of these slides.
Presentation is property of the author and ASCO. Permission required for reuse: contact permissions@asco.or
ANNUAL MEETING
---
Radiographic typical EGFR-Mutated Response NSCLC1 With 1L Amivantamab + Lazertinib in
CHRYSA -
1L Ami
Alypical
receive In CHRYSALIS-2 1L amivantamab Cohort + C, lazertinib a total of 49 treatment-naïve participants with atypical EGFR-mutated NSCLC were enrolled globally to
NSC
Median age was 60 years, 45% were female, and 57% were Asian
Most frequent EGFR mutationsᵃ included G719Xb (55%), S768Xc (27%), and L861Xd (24%)
Compound mutations were observed in 35% of tumors
At a median follow-up of 16.1 months, ORR was 57%
CBRe was 84%, and all evaluable patients with >1 post-baseline assessment achieved PR or SD
Median DoR was 20.7 months and median PFS was 19.5 months (95% CI, 11.2-NE)
0
-20
Change in SoD of target
lesions (%)
-40
PR
SD
-60
-80
-100
reused with permission from Tomasini P, et al. Amivantamab Plus Lazertinib in Atypical EGFR-mutated Advanced Non-Small Cell Lung Cancer Results From CHRYSALIS-2 Journal of Clinical Oncology. 2026,44(1):54-65. Vascopube org/doi/10 1200/JCO-24-02835
Figure Included G719A, G719S, and G719C. Compound mutations were observed in 14 participants. Included S7681 and S768L Compound mutations were observed in 11 participants. Included L861Q All participants L861R, and LB61G included Compound in the ORR mutations analysi "
4 Participants participants. may CBR be is counted defined in as 21 the category. percentage of participants achieving confirmed CR, PR, or durable SD (duration of 211 weeks). Five participants (NE, n=1; PD, n=2; SD, n=2) without a postbaseline tumor assessment are not shown. were
1. Tomasini P, et al. J Clin Oncol. 2026;44(1):54-65.
Copies of this slide deck obtained through Quick Response (QR)
A
Code are for personal use only and may not be reproduced without
of
these
slides.
KNO
G
CHRYSALIS-2 Study Design
CHRYSALIS 2
1L Ami Laz in
Atypical EGFR+
NSCLC
Dose expansion cohorts
Cohort A: EGFR Ex19del or L858R
Post-osimertinib and platinum-based chemotherapy
Cohort B: EGFR Ex20ins
Dose escalation phase
Previously reported1
Post-standard of care and platinum-based chemotherapy
Primary endpoint:
RP2CD was identified:
Cohort C: Atypical EGFR mutations
IV amivantamab 1050 mg
Treatment naive or post-EGFR TKI/chemotherapyᵇ
ORR by investigator per
(1400 mg if >80 kg)ª
RECIST v1.1
Cohort D: EGFR Ex19del or L858R
plus
Post-osimertinib, biomarker validation
Secondary endpoints:
DoR
Lazertinib 240 mg orally
Cohort E: EGFR Ex19del or L858R
Post-osimertinib, MET IHC+ analysis (amivantamab + lazertinib)
CBRc
PFS
Cohort F: EGFR Ex19del or L858R
OS
Post-osimertinib, MET IHC+ analysis (amivantamab monotherapy)
Safety (AEs)
Participants with Ex20ins and Ex19del/L858R co-mutations were excluded
CHRYSALIS-2 enrolled prior to COCOON2, SKIPPirr³, and PALOMA-34
Therefore, participants did not receive the enhanced prophylaxis for dermatologic AEs and IRRs, and subcutaneous amivantamab was
not available
CHRYSALIS-2 ClinicalTrials gov Identifier: NCT04077463 *Amivantamab was administered intravenously once every week during Cycle 1, with the first dose split between 2 days (350 mg once daily on C1D1, and the remainder on C102) and then every 2 weeks in subsequent cycles. Participants had
received 52 previous lines of treatment with chemotherapy and/or second generation EGFR TKI as the most recent line of therapy. °CBR is defined as the percentage of participants achieving confirmed CR, PR, or durable SD (duration of 211 weeks).
1. Tomasini P. et al. J Clin Oncol. 2026,44(1):54-65 2. Cho BC, et al. J Thorac Oncol 2025,20(10):1517-1530. 3. Spira Al, et al J Thorac Oncol 2025,20(6) 809-816. 4. Leight NB, et al. J Clin Oncol 2024;42(30) 3593-3605
2026 ASCO
PRESENTED BY: Joel W Neal
Copies of this slide deck obtained through Quick Response (QR)
#ASCO26
ASCO
AMERICAN SOCIETY OF
Code are for personal use only and may not be reproduced without
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco.org
permission from ASCO or the authors of these slides.
KNOWLEDGE CONQUERS CANCER
---
Radiographic Response With 1L Amivantamab + Lazertinib in
CJ
CHRYSALIS 2
1L Aml Laz in
Atypical EGFR-Mutated NSCLC¹
Atypical EGFR+
NSCLC
In CHRYSALIS-2 Cohort C, a total of 49 treatment-naïve participants with atypical EGFR-mutated NSCLC were enrolled globally to
receive 1L amivantamab + lazertinib
Median age was 60 years, 45% were female, and 57% were Asian
Most frequent EGFR mutationsᵃ included G719Xb (55%), S768Xc (27%), and L861Xd (24%)
Compound mutations were observed in 35% of tumors
At a median follow-up of 16.1 months, ORR was 57%
CBRe was 84%, and all evaluable patients with ≥1 post-baseline assessment achieved PR or SD
Median DoR was 20.7 months and median PFS was 19.5 months (95% CI, 11.2-NE)
0
-20
Change in SoD of target
lesions (%)
-40
PR
SD
-60
-80
-100
Figure reused with permission from Tomasini P. of al Amivantamab Plus Lazertinib in Alypical EGFR mutated Advanced Non-Small Cell Lung Cancer Results From CHRYSALIS-2 Journal of Clinical Oncology 2026;44(1) 54-65 https://ascopubs.org/doi/10 1200/JCO-24-02835
Participants may be counted in 21 category. Included G719A G719S, and G719C Compound mutations were observed in 14 participants. included S7681 and S768L Compound mutations were observed in 11 participants. included L861Q L861R, and L861G Compound mutations were observed
in
4
participants *CBR is defined as the percentage of participants achieving confirmed CR PR or durable SD (duration of 211 weeks). Five participants (NE, n=1; PD, n=2, SD, n=2) without a postbaseline tumor assessment are not shown All participants were included in the ORR analysis.
1. Tomasini P. of al J Clin Oncol 2026,44(1).54-65
2026 ASCO
PRESENTED BY: Joel W Neal
Copies of this slide deck obtained through Quick Response (QR)
#ASCO26
Code are for personal use only and may not be reproduced without
ASCO
AMERICAN SOCIETY
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asoo.org
permission from ASCO or the authors of these slides.
KNOWLEDGE CONQUERS CANCER
---
Overall Survival
CHRYSALIS- 2
1L Amt az in
Alypical EGFR+
NSCLC
100
85%
80
72%
Participants who are surviving (%)
60
55%
Median os
40
Median follow-up, 31.3 mo
(95% CI)
Amivantamab
41.0 mo (27.7-NE)
+
lazertinib
20
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
Months
No. at risk
Amivantamab lazertinib 49
44
37
37
36
36
36
34
29
27
26
22
19
15
10
10
8
1
0
2026 ASCO
PRESENTED BY: Joel W Neal
Copies of 745 stide deck obtained through Quick Response (QR)
ASCO
AMERICAN SOCIETY OF
#ASCO26
Code are for personal use only and may not be reproduced without
CURRENCAL -
ANNUAL MEETING
Presentation " property of the author and ASCO Permission required for revse, contact permissions@eson.org
permission from ASCO* or the authors of these sades
KNOWLEDGE CONQUERS CANCER
---
"
Conclusions
CHRYSALIS-2
N Am L62 in
Alypical
NSCLC
This single-arm study of amivantamab + lazertinib (n=49) in 1L atypical EGFR-mutated advanced NSCLC
demonstrates a clinically meaningful median OS of ~3.5 years
Responses were durable regardless of demographics, baseline tumor mutations, and disease characteristics
With longer follow-up, the safety profile of IV amivantamab + lazertinib was consistent with prior reports¹,²,
with no new safety signals
Amivantamab + lazertinib as a 1L treatment has now shown durable survival
in both common and atypical EGFR-mutated advanced NSCLC
1 of a Cin Oncol 2028,44(1) 54 65. 2. Yang OL of N Engl Med 2025,393(17) 1641-1593
2026 ASCO
PRE SENTED am Joel W Neal
Copies of (74) side Deck obtained through Quick Response (CIR)
#ASCO26
Code are for personal use only and may not be reproduced without
ASCO
INVOICAN SOCIETY DE
- -
ANNUAL MEETING
Presentation property of the author and ASCG Permission - - - contact permissions@wos.org
permission from ASCO* or the authors or these skins
KNOWLEDGE COMQUERS CANCER
Conclusions
CHRYSALIS. 2
1L Ami Laz in
Atypical EGFR+
NSCLC
This single-arm study of amivantamab + lazertinib (n=49) in 1L atypical EGFR-mutated advanced NSCLC
demonstrates a clinically meaningful median os of ~3.5 years
Responses were durable regardless of demographics, baseline tumor mutations, and disease characteristics
With longer follow-up, the safety profile of IV amivantamab - + lazertinib was consistent with prior reports¹,²,
with no new safety signals
Amivantamab + lazertinib as a 1L treatment has now shown durable survival
in both common and atypical EGFR-mutated advanced NSCLC
1. Tomasini P. etal.J Clin Oncol 2026;44(1) 54-65. 2. Yang JCH, et at N Engl Med. 2025,393(17) 1681-1693
2026 ASCO
PRE SENTED BY: Joel W Neal
#ASCO26
Copies of this slide deck obtained through Quick Response (QR)
ANNUAL MEETING
Code are for personal use only and may not be reproduced without
ASCO
AMERICAN SOCIETY OF
Presentation is property of the author and ASCO. Permission required for reuse; contact permissions@asco.org
CLINICAL ONCOLOGY
permission from ASCO or the authors of these stides
KNOWLEDGE CONQUERS CANCER
CHRYSALIS-2 Study Design
Dose expansion cohorts
CHRYSALIS-2
Cohort A: EGFR Ex19del or L858R
1L Aml Laz in
Atypical EGFR+
Post-osimertinib and platinum-based chemotherapy
NSCLC
Dose escalation phase
Cohort B: EGFR Ex20ins
RP2CD was identified:
Post-standard of care and platinum-based chemotherapy
IV amivantamab 1050 mg
Cohort C: Atypical EGFR mutations
Previously reported1
(1400 mg if ≥80 kg)a
Treatment naïve or post-EGFR TKI/chemotherapyᵇ
Primary endpoint:
Cohort D: EGFR Ex19del or L858R
ORR by investigator per
plus
RECIST v1.1
Post-osimertinib, biomarker validation
Lazertinib 240 mg orally
Cohort E: EGFR Ex19del or L858R
Secondary endpoints:
DoR
Post-osimertinib. MET IHC+ analysis (amivantamab + lazertinib)
CBRc
Cohort F: EGFR Ex19del or L858R
PFS
Post-osimertinib, MET IHC+ analysis (amivantamab monotherapy)
OS
Safety (AEs)
Participants with Ex20ins and Ex19del/L858R co-mutations were excluded
CHRYSALIS-2 enrolled prior to COCOON², SKIPPirr³, and PALOMA-34
Therefore, participants did not receive the enhanced prophylaxis for dermatologic AEs and IRRs, and subcutaneous amivantamab was
not available
CHRYSALIS-2 ClinicalTrials gov Identifier: NCT04077463 "Amivantamab was administered intravenously once every week during Cycle 1, with the first dose split between 2 days (350 mg once daily on C101, and the remainder on C102) and then every 2 weeks in subsequent cycles. Participants had
received <2 previous lines of treatment with chemotherapy and/or second-generation EGFR TKI as the most recent line of therapy. CBR is defined as the percentage of participants achieving confirmed CR, PR or durable SD (duration of 211 weeks).
1. Tomasini P. et al. J Clin Oncol. 2026;44(1):54-65. 2 Cho BC, et al. J Thorac Oncol. 2025,20(10):1517-1530. 3 Spira AI, et al. J Thorac Oncol 2025,20(6).809-816.4. Leight NB, et al. Clin Oncol 2024;42(30).3593-3605.
PRE SENTED BY: Joel W Neal
Copies of this slide deck obtained through Quick Response (QR)
026
ASCO
Code are for personal use only and may not be reproduced without
ASCO
AMERICAN SOCIETY
CLINICAL ONCOLOGY
#ASCO26
permission from ASCO® or the authors of these stides
KNOWLEDGE CONQUERS CANCER
NNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse: contact permissions@asco.org
---
Overall Survival
CHRYSALIS 2
mains
100
NOCLC
85%
80
72%
Participants who are surviving (%)
60
55%
40
Median os
Median follow-up, 31.3 mo
(95% CI)
Amivantamab
+
20
lazertinib
41.0 mo (27.7-NE)
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
No. at risk
51
Months
54
Amivantamab lazertinib 49
44
37
37
36
36
36
34
29
27
26
22
19
15
10
10
8
1
0
2026 ASCO
#ASCO26
PRESENTED BY: Joel W Neal
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse contact permissions@ason.org
Copies of this sade deck obtained through Quick Response (QR)
Code are for personal use only and may not be reproduced without
permission from ASCO of the authors of these slides
ASCO
MERCAN
CANCAL
KNOWLEDGE CONQUERS CANCER
---
Subsequent Therapy
CHRYSALIS-2
Mysical EGFR+
ROCLC
Most participants whose disease had progressed and discontinued 1L treatment were able to receive subsequent
therapy (71% [20/28])
The most common subsequent regimens included platinum-based chemotherapy-containing regimens (55%)
Amivantam (n=1)
15%
EGFR antibody-drug conjugate (n=1)
Supportive therapy (n=1)
30%
Afatinib (n=2)
Other
Participants (%)
Osimertinib (n=2)
Catequentinib (n=1)
TKI-based regimens
Ruserontinib (n=1)
Platinum-based chemotherapy-
Carboplatin-pemetrexed (n=4)
Cisplatin-pemetrexed (n=1)
containing regimens
Carboplatin-pernetrexed bevacizumab (n=3)
55%
Carboplatin-pemetrexed pembrolizumab (n=1)
Carboplatin-pernetrexed ivonescimab (n=1)
Carboplatin-paclitaxel + bevacizumab (n=1)
Amivantamab + lazertinib
(n=20)
2026 ASCO
PRE SENTED BY: Joel W Neal
Copies of his sade deck obtained through Quick Response (QR)
#ASCO26
Code are for personal ine only and may not be reproduced without
ASCO
CANCAL PHODUCE
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required or reuse, contact permissions@ason.org
permission from ASCO or the authors of these sades
KNOWLEDGE CONQUERS CANCER
---
Time on Treatment With Baseline Characteristics
CHRYSALIS-2
The median duration of treatmentᵃ with 1L amivantamab + lazertinib was 13.3 months (range, <0.1-53.2)
Alysical EGFR+
NSCLC
39% of 1L participants remained on treatment for >2 years
≥65y Asian CNS
PR
SD
PD
Ongoing
FO
0
6
12
18
24
30
36
42
48
54
Time on treatment (months)
"Treatment duration is defined as the duration from the day of the first dose of study drug to the day after the last dose of study drug.
PRE SENTED BY: Joel W Neal
Copies of this slide deck obtained through Quick Response (QR)
ASCO
AMERICAN DE
2026 ASCO
#ASCO26
Code are for personal use only and may not be reproduced without
CLINICAL SHCOLOGY
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco. org.
permission from ASCO or the authors of these slides
KNOWLEDGE CONQUERS CANCER
ANNUAL MEETING
Overall Survival
CHRYSALIS 2
1L Ami Laz in
Alypical EGFR+
NSCLC
100
85%
80
72%
Participants who are surviving (%)
60
55%
40
Median os
Median follow-up, 31.3 mo
(95% CI)
Amivantamab
+ lazertinib
41.0 mo (27.7-NE)
20
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
No. at risk
Months
Amivantamab lazertinib 49
44
37
37
36
36
36
34
29
27
26
22
19
15
10
10
8
1
0
2026 ASCO
#ASCO26
PRE SENTED BY: Joel W Neal
Copies of this slide deck obtained through Quick Response (QR)
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco org.
Code are for personal use only and may not be reproduced without
ASCO
AMERICAN SOCIETY or
permission from ASCO® or the authors of these slides.
CURICAL ONCOLOGY
KNOWLEDGE CONQUERS CANCER
---
Time on Treatment With Mutation Type/TP53 Status
CHRYSALIS-2
1L Ami Laz in
Atypical EGFR+
NSCLC
Local data
Central data
PACC Classical-like
TP53mut
PR
SD
PD
Ongoing
PD
0
6
12
18
24
30
36
42
48
54
Note: Unavailable samples are indicated by grayed-out TOWS in the oncoplot.
Time on treatment (months)
UT MD Anderson Cancer Center EGFR classification was based on local data If local data were not available, ctDNA collected via central testing was used (cells labeled with asterisk) There was high degree of concordance for participants within both datasets, discrepancies are denoted with a
dagger. PACC mutations comprise mutations spanning exons 18-21 including G719X, L747X S7681, L792X and T8541 and have been predicted to after the orientation of the P-loop or helix. Classical like, atypical EGFR mutations are distant from the ATP-binding pocket and are sensitive and
selective for all classes of EGFR TKis, ctDNA was collected via central testing and was not available for all participants
1. Robichaux JP, et al. Nature. 2021;597(7878):732-737.
2026 ASCO
PRESENTED BY: Joel W Neal
Copies of this side deck obtained through Quick Response (QR)
#ASCO26
ASCO
AMERICAN SOCIETY OF
Code are for personal use only and may not be reproduced without
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse; contact permissions@asco.org
permission from ASCO or the authors of these slides.
KNOWLEDGE CONQUERS CANCER
---
Uncommon EGFR mutations
EGFR
Function
ATP affinity
Prevalence
Have varying oncogenic
(within EGFR)
transformation potential
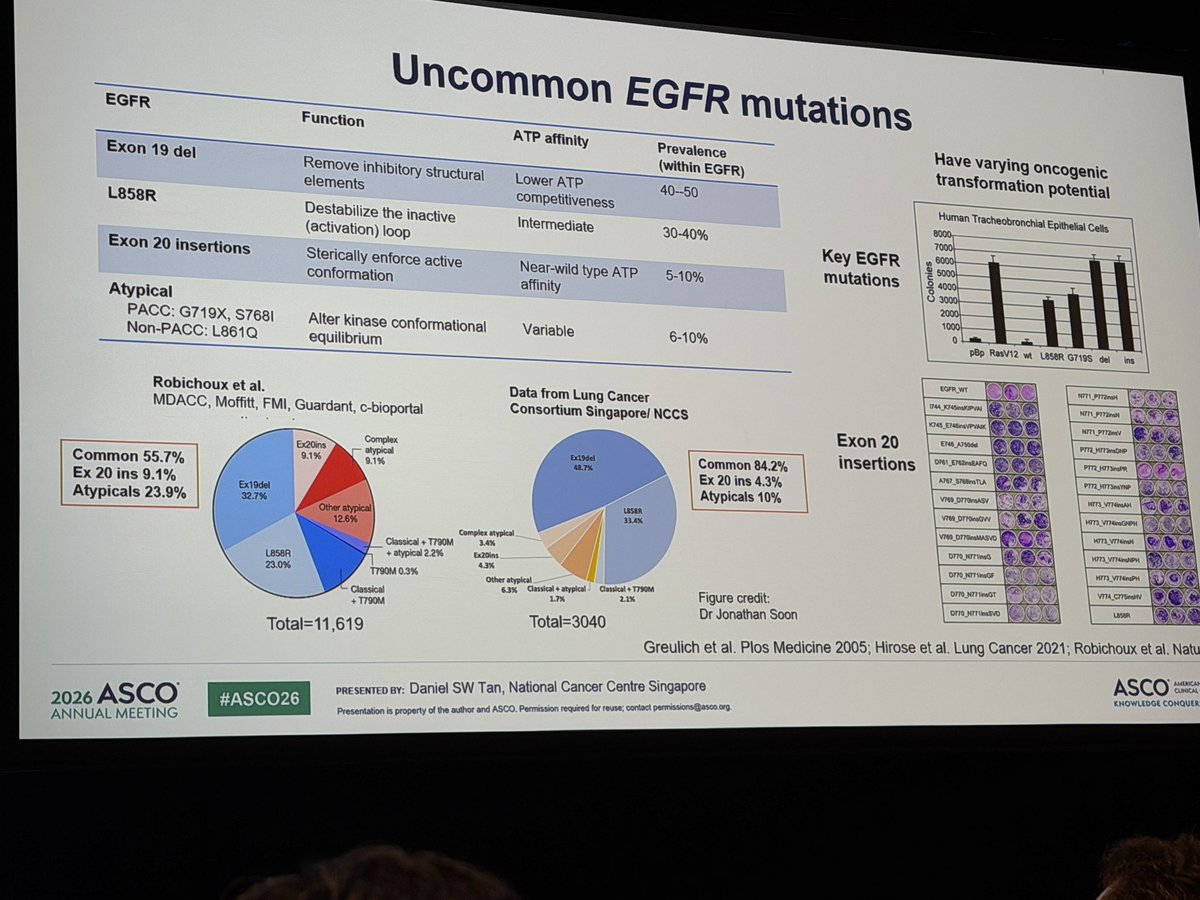
Exon 19 del
Remove inhibitory structural
Lower ATP
40-50
elements
competitiveness
Human Tracheobronchial Epithelial Cells
8000,
L858R
Destabilize the inactive
Intermediate
30-40%
7000
(activation) loop
Key EGFR
6000
Exon 20 insertions
Sterically enforce active
Near-wild type ATP
5-10%
Colonies
5000
mutations
4000
conformation
3000
affinity
2000
Atypical
1000
0
PACC: G719X, S7681
Alter kinase conformational
Variable
6-10%
pBp
RasV12
wt
L858R
G719S
del
ins
Non-PACC: L861Q
equilibrium
EGFR_WT
N771_P772naH
Robichoux et al.
Data from Lung Cancer
MDACC, Moffitt, FMI, Guardant, c-bioportal
Consortium Singapore/ NCCS
K745_E74BinsVPVAIK,
N771_PT72mV
Exon 20
E746_A7500d
Complex
Ex20ins
atypical
Ex19del
Common 55.7%
9.1%
Common 84.2%
insertions
D761_E762insEAFQ
9.1%
48.7%
Ex 20 ins 4.3%
A767_S766insTLA
Ex 20 ins 9.1%
Ex19del
Atypicals 10%
V769_D770msASV
HITS_V774insAH
Atypicals 23.9%
32.7%
Other atypical
LBSBR
V769_D770msGW
12.6%
33.4%
V769_D770insMASVO
Complex atypical
K773_V774mH
Classical T790M
3.4%
D770_N771ineG
L858R
atypical 2.2%
Ex20ins
23.0%
4.3%
T790M 0.3%
HIT3_V776insPH
Other atypical
Classical
6.3%
Classical atypical
Classical T790M
DF70_N771wwGT
V774_C775edWV
T790M
1.7%
2.1%
Figure credit:
Dr Jonathan Soon
D770_NF71lesSVD
LBSBR
Total=11,619
Total=3040
Greulich et al. Plos Medicine 2005; Hirose et al. Lung Cancer 2021; Robichoux et al. Natu
2026 ASCO
PRESENTED BY: Daniel SW Tan, National Cancer Centre Singapore
ASCO
AMERICAN
CUNICAL
#ASCO26
KNOWLEDGE CONQUER
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse; contact permissions@asco.org
---
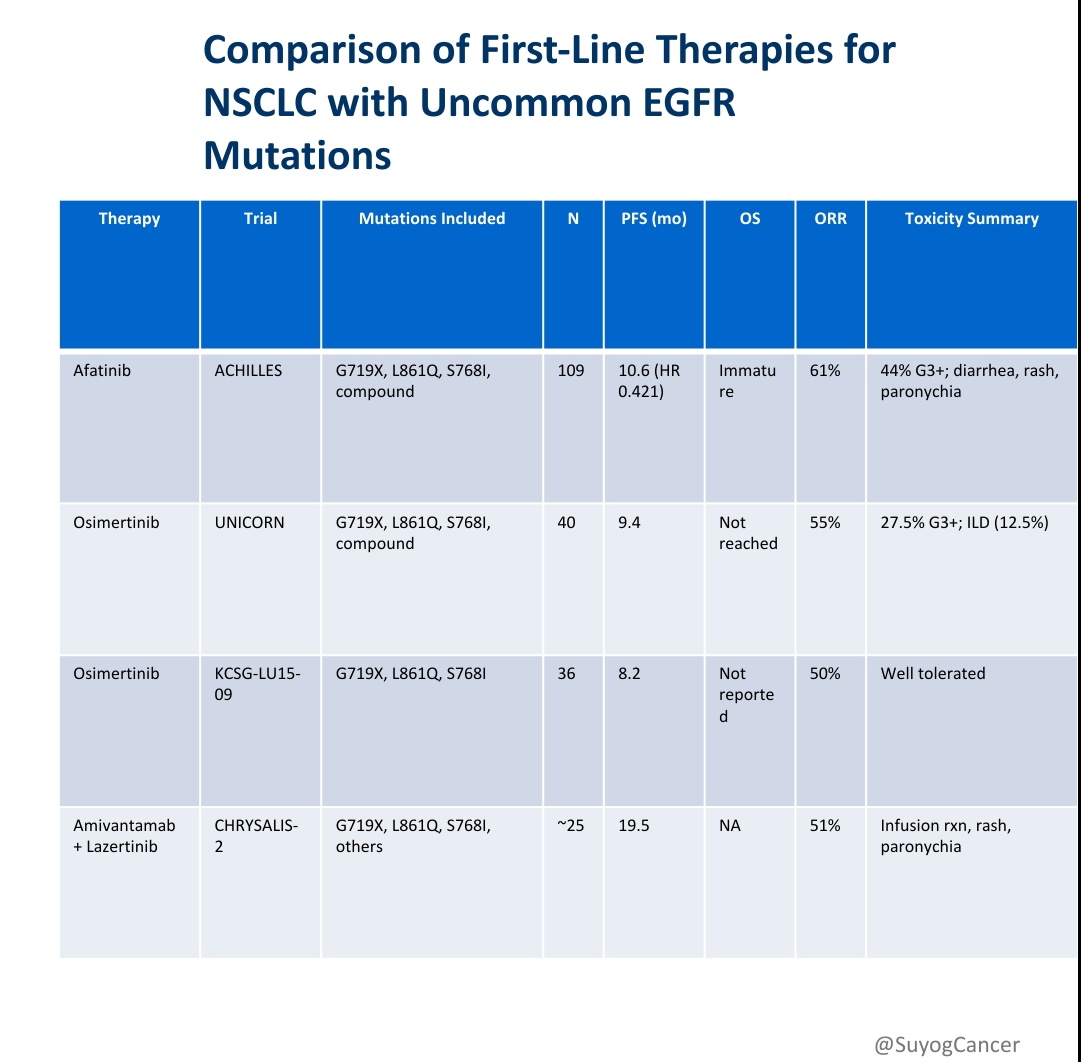
Selected therapeutic agents in atypical EGFR mutations
Trial
Phase
Drug
N=
ORR
mPFS
mDoR
OS
LUX post hoc
Retrospective
Afatinib
38
71.1%
10.7 m
11.1 m
19.4 m
ACHILLES/TORG1834
Randomised
Afatinib
73
61.4% V 47.1%
10.6 mv 5.7 m
10.6 mv 5.6 m
NR
phase Il
HR 0.421 [0.251-0.706]
HR 0.348 [0.16-0.758]
40 mg: HR 0.128, p<0.001
30 mg: HR 0.704, P 0.32
KCSG-LU15-09
Phase Il
Osimertinib
37
50%
8.2 m
11.2 m
NR
CNS (n=9) 5.4 m V 9.8 m
UNICORN
Phase Il
Osimertinib
42
55%
9.4 m
22.7 m
NR
FURTHER
Phase lb
Firmonertinib
45
160 mg: 43.5%
160 mg: 11.1 m
160 mg: 14.6 m
NR
240 mg: 68.2%
240 mg: 16 m
240 mg: NR
NCT05256290
Phase Il
Silevertinib
43
200 mg: 60%
15.2 m
NR
NR
CHRYSALIS-2
Phase Il
Amivantamab-
105
1L: 57%
1L: 19.5 m
1L: 20.7 m
1L: NR
Lazertinib
2L: 48%
2L: 7.8 m
>2L: 11.0 m
>2L: 22.8 m
Afatinib is FDA/ EMA approved based on LUX post hoc analysis
Osimertinib has been incorporated into guidelines
ALPACCA [NCT07185997] : First randomized phase III trial for PACC
mutations comparing firmonertinib 240 mg V afatinib/ osimertinib (n=480)
Yang TLO 2015; Miura JCO 2025; Cho JCO 2020; Akuma JAMA Oncology 2024; Le WCLC 2025; Tomasini JCO 2025; Black Diamond press release/ Rotow ASCO 2026
2026 ASCO
#ASCO26
PRESENTED BY: Daniel SW Tan, National Cancer Centre Singapore
ASCO
AMERICAN SOCIETY OI
ANNUAL MEETING
CUNICAL ONCOLOGY
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
ASCO 2026
CHRYSALIS-2
MV Onco
1L Amivantamab + Lazertinib
in Atypical EGFR NSCLC
Updated Overall Survival Analysis
1
Historically Difficult
EGFR Biology
EGFR
Atypical EGFR mutations
historically show inferior
outcomes versus classical
Can deeper
EGFR disease.
EGFR pathway
suppression
Prior afatinib global OS:
improve survival?
~19 months
2
Dual EGFR Pathway Suppression
Extracellular
Blockade
Amivantamab
Intracellular
Lazertinib
EGFR-MET
Inhibition
3rd-Generation
Bispecific Antibody
EGFR TKI
Biologic dual targeting for uncommon EGFR disease
3
The Survival Headline
Median OS
41.0
Months
~3.5 Years Survival
55%
46%
alive at 3 years
alive at 4 years
4
Long-Term Disease Control
20%
Some
7 patients
still on
beyond
continued
treatment
4 years
>3 years
Durable disease suppression appears achievable
in selected atypical EGFR tumors.
5
One Core Clinical Takeaway
"
Atypical EGFR NSCLC may no longer
represent a uniformly poor-prognosis
EGFR subgroup.
Amivantamab lazertinib demonstrated
clinically meaningful long-term survival in a
historically challenging population.
8
Joel Neal et al
ASCO 2026
CHRYSALIS-2
Educational infographic for oncology professionals. Source: Joel Neal Updated Overall Survival Analysis of CHRYSALIS-2. Presented at ASCO 2026.
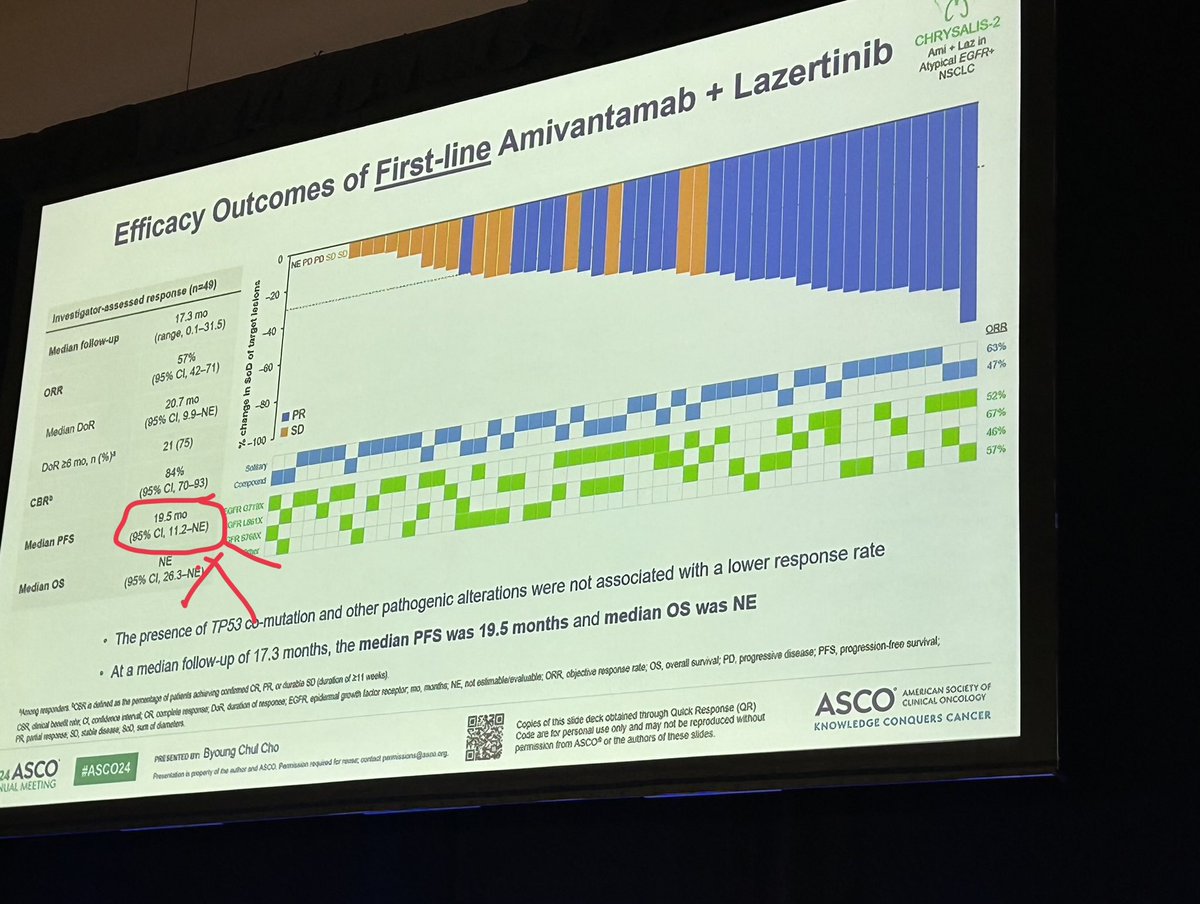
Efficacy Outcomes of First-line Amivantamab + Lazertinib
CHRYSALIS-2
Ami Laz in
Atypical EGFR+
NSCLC
0
Investigator-assessed response (n=49)
NE PD PD SD SD
17.3 mo
-20
Median follow-up
(range, 0.1-31.5)
(95% CI, 42-71)
change In SoD of target leclons
-40
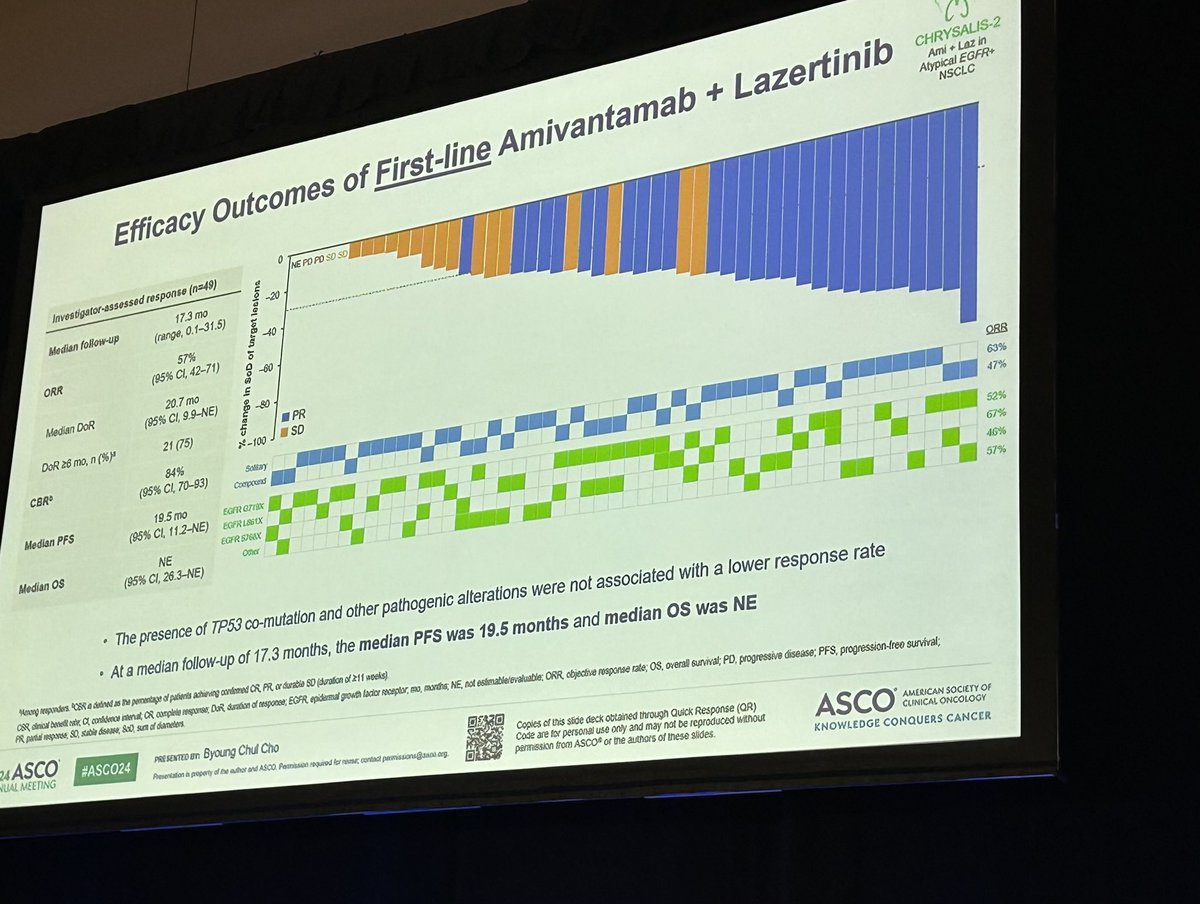
57%
ORR
-60
20.7 mo
Median DoR
(95% CI, 9.9-NE)
-80
PR
DoR 26 mo, n (%)*
21 (75)
N-100
SD
84%
ORR
CBR
Solitary
(95% CI, 70-93)
63%
Compound
47%
19.5 mo
Median PFS
EGFR G7TBX
(95% Cl, 11.2-NE)
52%
EGFR LS61X
67%
EGFR STATE
NE
46%
Median OS
Other
(95% Cl, 26.3-NE)
57%
The presence of TP53 co-mutation and other pathogenic alterations were not associated with a lower response rate
At a median follow-up of 17.3 months, the median PFS was 19.5 months and median OS was NE
4mmg responders CSR 0 defined 15 the percentage of patients achieving condinmed CR PR or durable SD (duration of 211 weeks)
PR CSR partial clinical response, benefit SO, stable a confidence disease, internal SoD, sun OR of complete diameters response Dar duration of response; EGFR epidemal growth lador receptor, no, munths, NE, not eslimable/evaluable: ORR objective response rate; OS, overall survival; PD, progressive disease; PFS, progression-free survival;
24
ASCO
#ASCO24
PRESENTED un Byoung Chul Cho
Copies of this slide deck obtained through Quick Response (QR)
UAL MEETING
ASCO®
AMERICAN SOCIETY OF
Presentation a property of the author and ASCO. Permission required for contact permissions@daco.com org.
Code are for personal use only and may not be reproduced without
CUNICAL ONCOLOGY
permission from ASCO or the authors of these slides
KNOWLEDGE CONQUERS CANCER
---
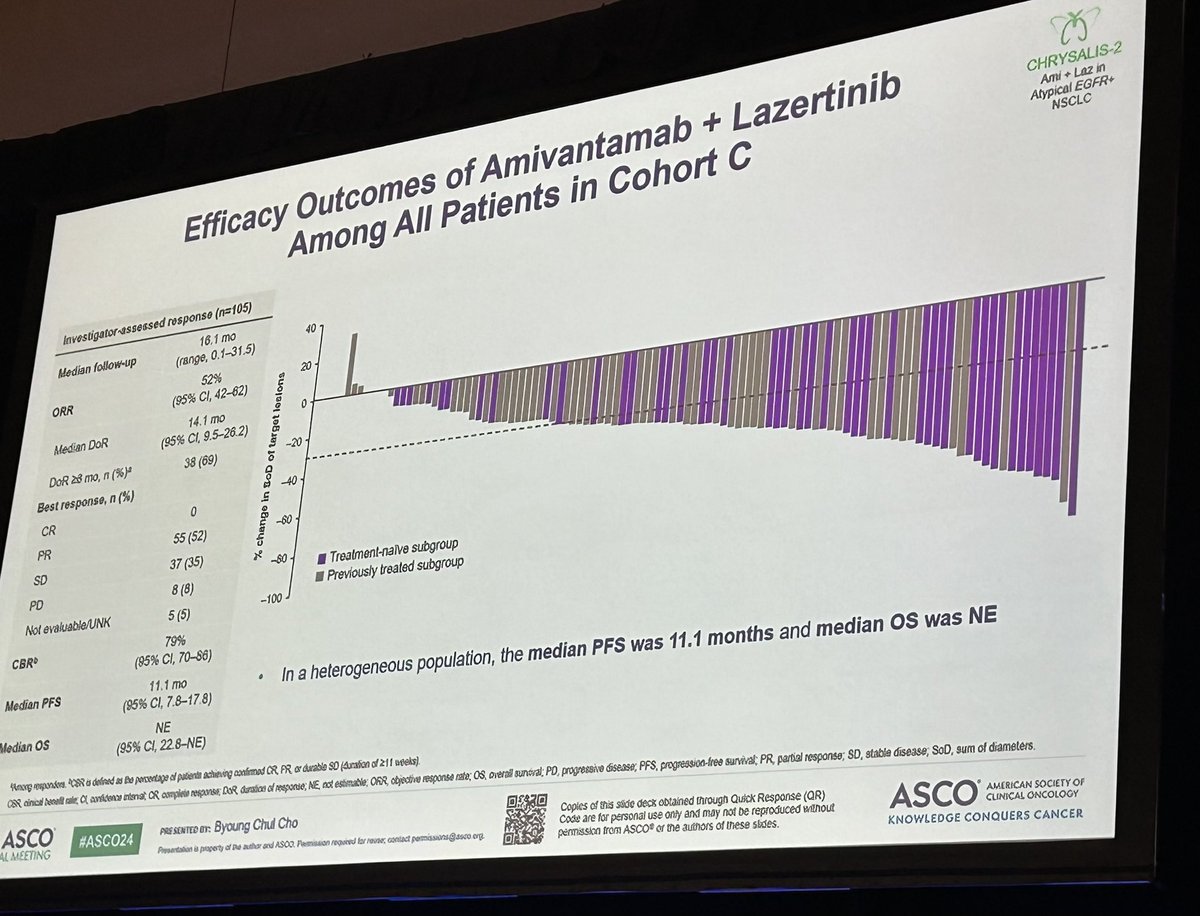
Efficacy Outcomes of Amivantamab + Lazertinib
CHRYSALIS-2
Ami Laz in
Among All Patients in Cohort C
Atypical EGFR+
NSCLC
Investigator-assessed response (n=105)
16.1 mo
Median follow-up
40
(range, 0.1-31.5)
52%
20
ORR
(95% CI, 42-62)
14.1 mo
0
Median DoR
(95% CI, 9.5-26.2)
DoR 28 mo, n (%)*
38 (69)
% change in BOD of target lesions
-20
Best response, n (%)
-40
CR
0
PR
55 (52)
-60
SD
37 (35)
-80
Treatment-nalve subgroup
PD
8 (8)
Previously treated subgroup
Not evaluable/UNK
5 (5)
-100
79%
CBR
(95% CI, 70-86)
Median PFS
11.1 mo
In a heterogeneous population, the median PFS was 11.1 months and median os was NE
(95% Cl, 7.8-17.8)
NE
Median OS
(95% CI, 22.8-NE)
Rong responders. RSR 0 defined 35 to percentage of patients achieving confirmed CR FR or durable SD (Auration of 211 weeks)
CSR oinical will cale, a confidence intenat OR complete response; DOR duration of response; NE, not estimable; ORR, objective response rate: OS, overall survival; PD, progressive disease; PFS, progression-free survival; PR, partial response; SD, stable disease; SoD, sum of diameters.
ASCO
#ASCO24
PRE SENTED or: Byoung Chul Cho
Copies of this stide deck obtained through Quick Response (QR)
LL MEETING
Presentation il property of Do author and ASOO Permission required for rouse, contact permissions@asco erg.
Code are for personal use only and may not be reproduced without
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
permission from ASCO® or the authors of these studes.
KNOWLEDGE CONQUERS CANCER
Efficacy Outcomes of First-line Amivantamab + Lazertinib
CHRYSALIS-2
Ami Laz in
Atypical EGFR+
NSCLC
0
Investigator-assessed response (n=49)
NE PD PD SD SD
17.3 mo
-20
Median follow-up
(range, 0.1-31.5)
(95% CI, 42-71)
2-100 change In SOD of target lecions
-40
57%
ORR
-60
20.7 mo
Median DoR
(95% CI, 9.9-NE)
-80
PR
DoR 26 mo, n (%)*
21 (75)
SD
84%
ORR
CBR
Solitary
(95% CI, 70-93)
63%
Compound
47%
19.5 mo
Median PFS
GFR
52%
(95% Cl, 11.2-NE)
GFR L861X
67%
S7GAX
46%
NE
Median OS
57%
(95% CI, 26.3-NE
The presence of TP53 co-mutation and other pathogenic alterations were not associated with a lower response rate
At a median follow-up of 17.3 months, the median PFS was 19.5 months and median os was NE
Menorg CSN 0 delined 35 the permentage of patients achieving confirmed CR PR or durable SD (duration of 11 weeks)
PR partial response, SO, stable disease, SoD, sun of diameters
CSR clinical boned NOR a confidence and CR complete response Dan duration of response; EGFR epidemal growth lactor receptor, no, months; NE, not estimable/evaluable; ORR objective response rate; OS, overall survival; PD. progressive disease; PFS, progression-free survival;
24 ASCO
#ASCO24
PRESENTED un Byoung Chul Cho
Copies of this slide deck obtained through Quick Response (QR)
UAL MEETING
ASCO®
AMERICAN SOCIETY OF
Presentation a property of the why and ASCO. Permission required for - contact permissions@asoo org.
Code are for personal use only and may not be reproduced without
CLINICAL ONCOLOGY
permission from ASCO or the authors of these slides.
KNOWLEDGE CONQUERS CANCER
Amivantamab and lazertinib in patients with EGFR-mutant non-small cell
lung (NSCLC) after progression on osimertinib and platinum-based
chemotherapy: Updated results from CHRYSALIS-2
Presented by: Catherine Shu
Abstract #9006
Stage IV NSCLC mutated
EGFR ex 19del/L858R
Phase
10 Conor
day
n=162 (Cohort A)
-
dination
Amivantamab + Lazertinib
-
n=50 evaluable
Phase
the
I
I
PRIMARY OUTCOME: ORR
33%
MEDIAN DOR (MOS)
I
9.6
to
lines
I
149
I
Most common grade >3 treatment-related AEs (TRAEs) were infusion-related reactions (7%),
turner
1
Exclusion
Criteria
acneiform dermatitis (5%). and hypoalbuminemia (4%)
I
mm
VO %
I
Among an unselected population that has exhausted SOC osi and pt-chemo,
III
III
#
ami and laz demonstrates encouraging antitumor activity with a
+
-
manageable safety profile
https://bit.ly/5N9joqC
Created by:
@ADesaiMD
---
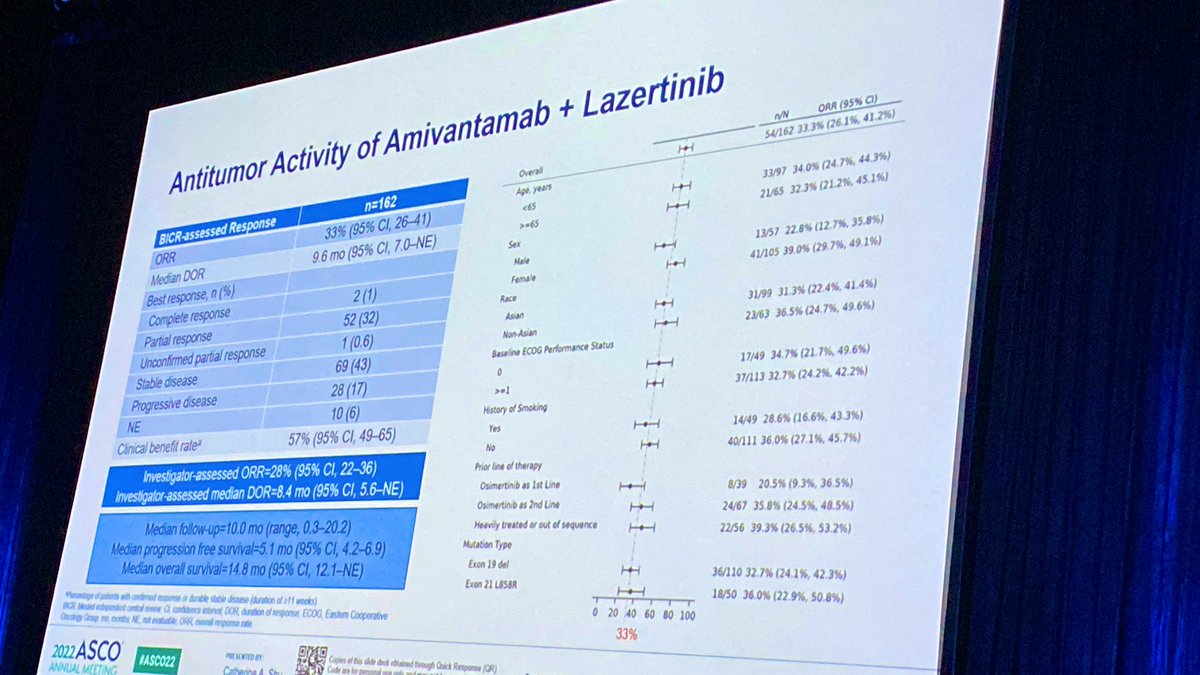
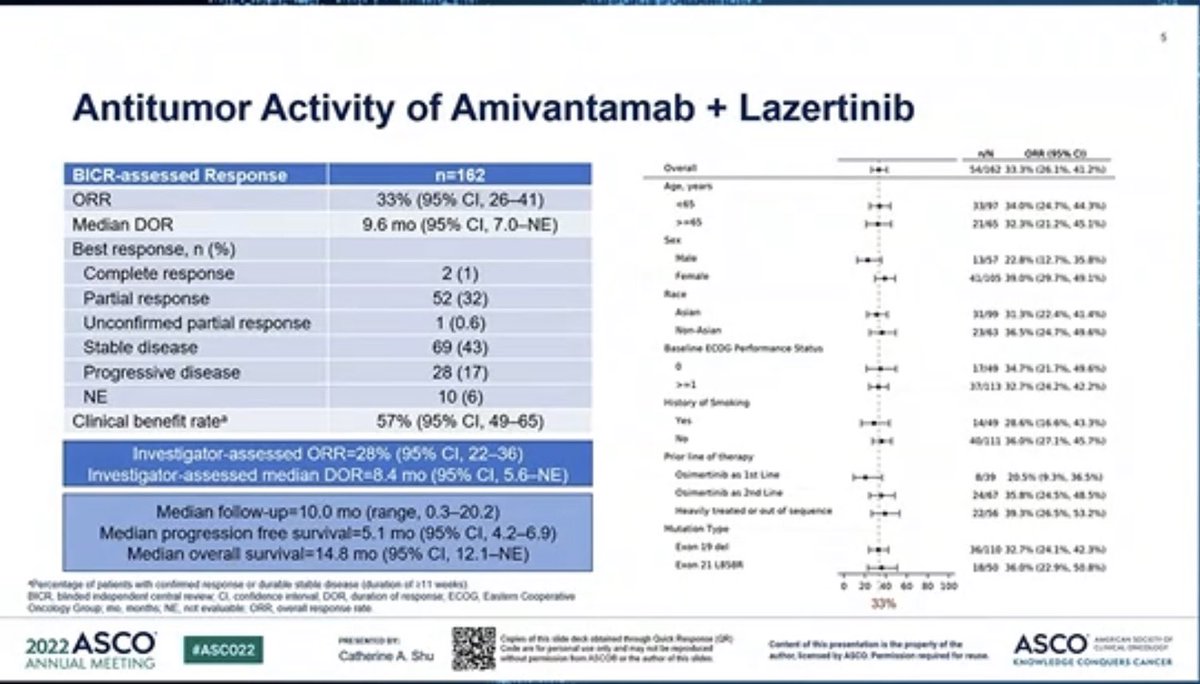
Antitumor Activity of Amivantamab + Lazertinib
n/N ORR (95% C)
Overall
I
54/162 33.3% (26.1%, 41.2%)
BICR-assessed Response
n=162
Age, years
33/97 34.0% (24.7%, 44.3%)
33% (95% CI, 26-41)
<65
ORR
>=65
21/65 32.3% (21.2%, 45.1%)
Median DOR
9.6 mo (95% Cl, 7.0-NE)
Sex
Best response, n (%)
Male
13/57 22.8% (12.7%, 35.8%)
Complete response
2(1)
Female
41/105 39.0% (29.7%, 49.1%)
Race
Partial response
52 (32)
Asian
31/99 31.3% (22.4%, 41.4%)
Unconfirmed partial response
1 (0.6)
Non-Asian
23/63 36.5% (24.7%, 49.6%)
Stable disease
69 (43)
Baseline ECOG Performance Status
Progressive disease
28 (17)
0
17/49 34.7% (21.7%, 49.6%)
>=1
NE
10 (6)
37/113 32.7% (24.2%, 42.2%)
History of Smoking
Clinical benefit rate
57% (95% CI, 49-65)
Yes
14/49 28.6% (16.6%, 43.3%)
No
investigator-assessed ORR=28% (95% CI, 22-36)
40/111 36.0% (27.1%, 45.7%)
Prior line of therapy
Investigator-assessed median DOR=8.4 mo (95% CI, 5.6-NE)
Osimertinib as 1st Line
Osimertinib as 2nd Line
8/39 20.5% (9.3%, 36.5%)
Median follow-up=10.0 mo (range, 0.3-20.2)
Median progression free survival=5.1 mo (95% CI, 4.2-6.9)
Heavily treated or out of sequence
24/67 35.8% (24.5%, 48.5%)
Mutation Type
22/56 39.3% (26.5%, 53.2%)
Median overall survival=14.8 mo (95% CI, 12.1-NE)
Exon 19 del
Fecentage BOR Meded of policity with confirmed tesponse a Surable dable disease (duration of
Exon 21 LBS8R
36/110 32.7% (24.1%, 42.3%)
Ottobogy Group m noths and NE, - NR evaluatie, a confidence ORR overal interval response DOR duration rate of response, 11 wooks) ECOG, Eastem Cooperative
18/50 36.0% (22.9%, 50.8%)
0 20 40 60 80 100
2022ASCO
33%
#ASCO22
PAY BY
DMO
ANNUAL MEETING
Catherine
L
is
Copies Code of for his dide deck obtained brough Chick Response (QR)
[Slide 1]
10
Conclusions
Amivantamab + lazertinib demonstrated durable antitumor activity in patients with EGFRm NSCLC. after
progressing on both osimertinib and platinum chemotherapy
Treatment
Activity is comparable to that in previously reported post-osimertinib, chemotherapy-nalve population, suggesting
Benefit
that intervening chemotherapy does not impact amivantamab + lazertinib activity
⑉
Safety profile of amivantamab + lazertinib is consistent with prior reports; no new safety signals were identified
Safety
Among a population that has exhausted standard of care including heavily pretreated patients, amivantamab
+
lazertinib demonstrated clinically significant and durable antitumor activity, without biomarker selection
The CHRYSALIS-2 study (ClinicalTrials.gov Identifier: NCT04077463) is ongoing. and the understanding of
underlying resistance mechanisms will be reported at a future meeting
Key
MARIPOSA (NCT04487080) and MARIPOSA-2 (NCT04988295). ongoing phase 3 randomized trials, are
evaluating amivantamab * lazertinib in the frontline and amivantamab + lazertinib carboplatin + pemetrexed in
Takeaway
post-osimertinib settings
and
Amivantamab monotherapy upcoming in METex14skip oral presentation (ASCO 2022 #9008)
Next Steps
EGFRm epidermal growth factor receptor-mutated NSOLC non-small cell lung cancer.
1. Baumi al. Presented at ASCO June 4-8 2024 9006 (onal)
2022
ASCO
PRESENTION
Capien
of
this
deck
ICAS
#ASC022
Cinde
the
Contact of dis presentation is the property of the
ASCO
Catherine A Shu
author licensed ity water Permission required for
ANNUAL MEETING
ENOWLEDGE CONQUERS CANCER
---
[Slide 2]
5
Antitumor Activity of Amivantamab + Lazertinib
N/M
044 (95% C)
Overall
BICR-assessed Response
n=162
H
14/042
ORR
33% (95% CI, 26-41)
-
3399 14.0% Q2.7% you
Median DOR
9.6 mo (95% CI, 7.0-NE)
I
21/65 45.1%
Best response, n (%)
Had
1363 22.8%
Complete response
2 (1)
H
40/305 29.0% (99.7%) 49.1%
Partial response
52 (32)
***
31/99 30.3%% (22.4%) m
Unconfirmed partial response
1 (0.6)
I
23/43 6.3% 24.7% 48.4%
Stable disease
69 (43)
Performance Status
Progressive disease
28 (17)
-
1349 M4%217% 49.6%
-
13/01/ 2.2%
NE
10 (6)
Clinical benefit rate
57% (95% CI, 49-65)
DANG 43.3%
-
40913
Investigator-assessed ORR=28% (95% CI, 22-36)
line of therapy
Investigator-assessed median DOR=8.4 mo (95% CI, 5.6-NE)
Osimertinio an 1st Line
8/39 20.5% (9.3% 36.5%
24/07 35.8% (34.5% 48.5%
Median follow-up=10.0 mo (range, 0.3-20.2)
22/54 13.2%
Median progression free survival=5.1 mo (95% CI, 4.2-6.9)
Multiation Type
(not 29 del
Median overall survival=14.8 mo (95% .1-NE)
wed
16/110 32.7% Q4.1% 42.3%
Exam 21 USSIA
use 36.0% (22.9%
of patients with confirmed response or durabile stable disease (duration if all works)
20
NO
40
so
300
BICR independent central review CI confidence anthonwal DOR duration of response ECOG Convinent Cooperative
Oncology Group months NE ALE evaluable ORR overall
33%
ASCO
-
2022
of
the
#ASC022
ASCO
Catherine A Shu
ANNUAL MEETING
---
[Slide 3]
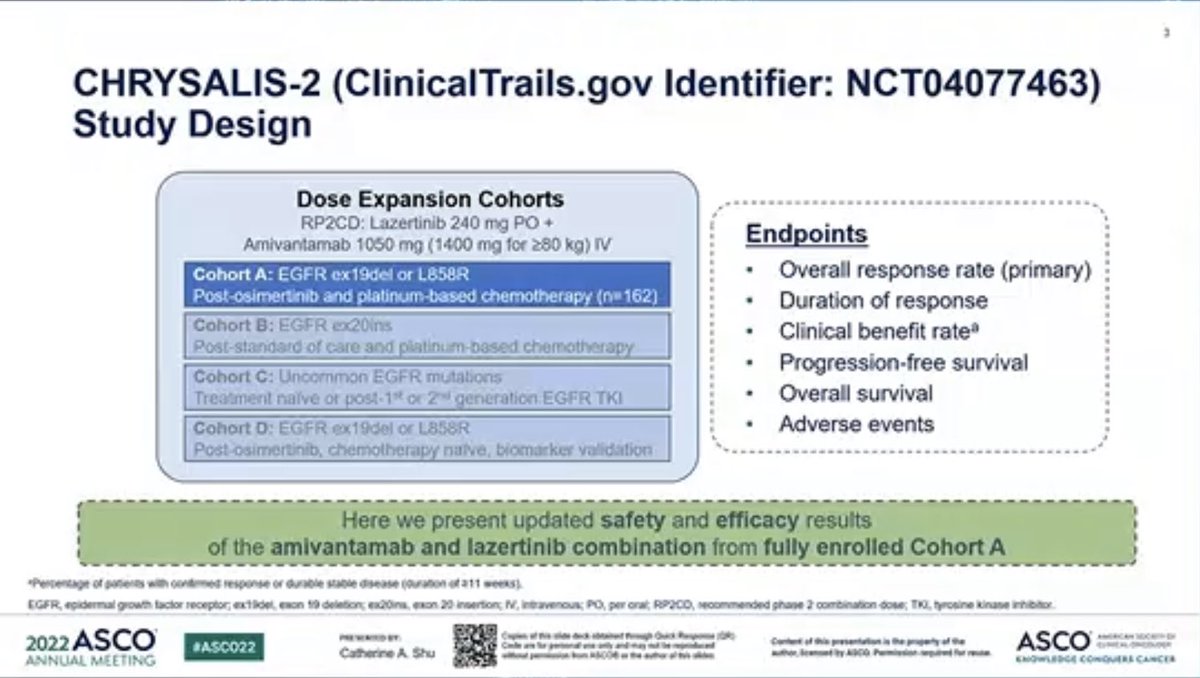
CHRYSALIS-2 (ClinicalTrails.gov Identifier: NCT04077463)
Study Design
Dose Expansion Cohorts
RP2CD: Lazertinib 240 mg PO +
Amivantamab 1050 mg (1400 mg for >80 kg) IV
Endpoints
Cohort A: EGFR ex19del or L858R
Overall response rate (primary)
Post-osimertinib and platinum-based chemotherapy (nu 162)
Duration of response
Cohort B: EGFR 20ins
Clinical benefit rate
Post-standard of care and platinum-based chemotherapy
Progression-free survival
Cohort C: Uncommon EGFR mutations
Treatment naive or post-1 or 2nd generation EGFR TKI
Overall survival
Cohort D: EGFR ex19del or L858R
Adverse events
Post-osimertinib, chemotherapy naive, biomarker validation
Here we present updated safety and efficacy results
of the amivantamab and lazertinib combination from fully enrolled Cohort A
*Percentage of patients with continued response or durable stable disease (duration of 211 weeks)
EGFR growth factor receptor; exticie each 19 deletion es20ins. exon 20 insertion; N. intravenous PO per onal RP2CO recommended phase 2 combination dose TO tyrosine kinane inhibitor
2022
ASCO
#ASC022
the property
ASCO
Catherine A Shu
was
ANNUAL MEETING
CHRYSALIS-2 (NCT04077463) is a global Phase 1/1b study of amivantamab (an EGFR-MET bispecific antibody) plus lazertinib (a CNS-penetrant third-generation EGFR-TKI). Cohort C enrolled treatment-naive patients with atypical EGFR mutations (uncommon mutations, excluding exon 20 insertions and co-mutations with classical EGFR) — a historically under-served population. At ASCO 2026 (Abstract 8501, presented May 30 by Joel W. Neal), investigators reported updated overall-survival data for the treatment-naive population (n=49). The primary endpoint was investigator-assessed ORR; OS was a key secondary endpoint.
Population
Treatment-naïve advanced NSCLC with atypical EGFR mutations (excluding exon 20 insertions and classical-EGFR co-mutations); <2 prior lines permitted (n=49).
Intervention
IV amivantamab 1050 mg weekly (1400 mg if ≥80 kg) + lazertinib 240 mg orally once daily.
Primary Endpoint
Objective response rate by investigator (RECIST v1.1).
Key Secondary
Overall survival, duration of response, and progression-free survival.
Efficacy & Safety
Reported Results
Objective Response & PFS
Investigator-assessed ORR was 57% with a median duration of response of 20.7 months (95% CI, 9.9–NE). Median PFS was 19.5 months (95% CI, 11.2–NE).
At a median follow-up of 31.3 months (data cutoff Oct 31, 2025), median OS was 41.0 months (95% CI, 27.7–NE) — with 55% alive at 3 years and 46% at 4 years. As of cutoff, 20% of patients (10/49) remained on first-line treatment (range 2.5–4.4 years), and 7 had received amivantamab for >3 years.
The safety profile was consistent with prior reports of amivantamab + lazertinib, with no new signals on longer follow-up. The regimen produced a clinically meaningful median OS of nearly 3.5 years in a historically challenging population, with many patients staying on first-line therapy long term.
STATUSInvestigational in atypical EGFR — approved in classical EGFR & exon20ins
Amivantamab (Rybrevant) + lazertinib is FDA-approved for first-line classical EGFR (ex19del / L858R) advanced NSCLC (MARIPOSA), and amivantamab + chemotherapy is approved for EGFR exon 20 insertion NSCLC (PAPILLON). Use in atypical (uncommon, non-exon20ins) EGFR mutations — the CHRYSALIS-2 Cohort C population — is investigational; these data support that potential indication. A subcutaneous amivantamab formulation is also FDA-approved.
CHRYSALIS-2 (NCT04077463) is a global Phase 1/1b study of amivantamab (Rybrevant), an EGFR-MET bispecific antibody, plus lazertinib (Lazcluze), a CNS-penetrant third-generation EGFR tyrosine-kinase inhibitor. Cohort C enrolled treatment-naive patients with atypical (uncommon) EGFR mutations — excluding exon 20 insertions and classical-EGFR co-mutations. It is sponsored by Johnson & Johnson (Janssen).
What were the CHRYSALIS-2 Cohort C results?
In 49 first-line patients with atypical EGFR-mutated NSCLC, amivantamab plus lazertinib produced an investigator-assessed objective response rate of 57%, median duration of response 20.7 months, median progression-free survival 19.5 months and median overall survival 41.0 months at 31.3-month median follow-up (ASCO 2026, Abstract 8501), with 3-year and 4-year overall survival of 55% and 46%.
Is amivantamab plus lazertinib FDA approved for atypical EGFR mutations?
No. The atypical/uncommon EGFR-mutation use studied in CHRYSALIS-2 Cohort C is investigational. Amivantamab (Rybrevant) plus lazertinib (Lazcluze) is FDA approved (August 2024, based on MARIPOSA) for first-line NSCLC with the common EGFR exon 19 deletion or exon 21 L858R mutations — not for the atypical/uncommon mutations in Cohort C.
Why is CHRYSALIS-2 Cohort C important?
Atypical (uncommon, non-exon-20-insertion) EGFR mutations are a heterogeneous, historically under-served group with limited targeted options and generally poorer outcomes on standard EGFR TKIs. The Cohort C data suggest amivantamab plus lazertinib may offer meaningful, durable activity — a median overall survival of nearly 3.5 years — in this difficult population, supporting further study.
What is the safety profile of amivantamab plus lazertinib in CHRYSALIS-2?
The safety profile was consistent with prior reports of amivantamab plus lazertinib, with no new safety signals on longer follow-up. Known class effects of the combination include EGFR-related skin and nail toxicity, infusion-related reactions, and venous thromboembolism, which are managed with supportive care and prophylaxis in the broader amivantamab program.