The first multinational Phase 3 trial of oral sunvozertinib (Zegfrovy) vs platinum-pemetrexed chemotherapy in treatment-naïve EGFR exon20-insertion NSCLC. Presented at ASCO 2026 (LBA8500), published simultaneously in NEJM.
Abstract LBA8500
X
Sunvozertinib monotherapy versus platinum-based
chemotherapy as first-line treatment for advanced
NSCLC with EGFR exon20ins: Primary analysis of a
multinational phase 3 randomized study (WU-KONG28).
Snangnai, China
Background:
Sunvozertinib has been granted accelerated approval in
the US and China for the treatment of patients with
advanced non-small cell lung cancer (NSCLC) harboring
epidermal growth factor receptor exon 20 insertion
mutations (EGFR exon20ins) who failed platinum-based
chemotherapy, based on results from two phase 2 single
arm pivotal studies (WU-KONG1B [NCT03974022] and WU-
KONG6 [NCT05712902]). WU-KONG28 (NCT05668988) is a
multinational randomized confirmatory phase 3 study to
compare sunvozertinib versus platinum-based
chemotherapy as first-line treatment in advanced NSCLC
patients with EGFR exon20ins. Here we reported the
primary analysis of WU-KONG28 study results.
---
Methods:
Eligible patients were randomized in a 1:1 ratio, stratified
by baseline brain metastasis status, to receive either
sunvozertinib 300 mg once daily or chemotherapy
(carboplatin [AUC5] and pemetrexed [500 mg/m²]) once
every 3 weeks for up to 6 cycles, followed by pemetrexed
maintenance therapy until disease progression or other
discontinuation criteria were met. Patients in the
chemotherapy arm could cross over to receive
sunvozertinib upon confirmed progressive disease by the
blinded independent central review (BICR). The primary
endpoint was progression free survival (PFS) assessed by
BICR per RECIST 1.1. Secondary endpoints included overall
survival (OS), objective response rate (ORR), duration of
response (DoR), and safety profile. PFS and os were
analyzed using log-rank test and Cox proportional hazards
model. The data cutoff date was Jan 16, 2026.
---
Results:
A total of 324 patients were randomized to receive
sunvozertinib (N=163) or chemotherapy (N=161). Baseline
characteristics were generally balanced between the two
arms. PFS by BICR was significantly longer with
sunvozertinib than chemotherapy (median: 10.3 vs 7.5
months; hazard ratio [HR]: 0.65, 95% confidence interval
[CI]: 0.50, 0.85, p=0.0008). The PFS benefit was consistent
in trends across subgroups. In the chemotherapy arm,
90.2% of patients with BICR-confirmed disease
progression crossed over to receive sunvozertinib. The os
data were immature. Patients in the sunvozertinib arm
showed higher confirmed ORR (58.9% vs 31.1%) and
longer median DoR (11.2 vs 7.1 months). Safety profile of
sunvozertinib was similar to what was previously reported.
Drug-related treatment emergent adverse events (TEAEs)
leading to treatment discontinuation occurred in 7.4% of
patients. No drug-related TEAE leading to fatal outcome
was reported.
---
Conclusion:
Sunvozertinib demonstrated significantly superior
antitumor efficacy than chemotherapy with a manageable
safety profile. These results support sunvozertinib as a
first-line treatment for advanced NSCLC harboring EGFR
exon20ins.
MEDICINE OF 1926 1812 NEW NOR ENGLAND
The NEW ENGLAND
JOURNAL
JOURNAL of MEDICINE
ORIGINAL ARTICLE
f X in
x
First-Line
Sunvozertinib in
NSCLC with EGFR Exon
20 Insertion Mutations
Authors: Caicun Zhou, M.D., Ph.D., Laurent
Greillier, M.D., Ph.D., Geoffrey Liu, M.D.,
Thomas John, M.B., B.S., Ph.D., Ligang Xing,
M.D., Ph.D., Dariusz Kowalski, M.D., Ph.D.,
Regan M. Memmott, M.D., Ph.D., +23 , for the
WU-KONG28 Investigators* Author Info &
Affiliations
Published May 29, 2026
100
Median
90
Progression-free
Survival
80
(95% CI)
70
mo
Percentage of Patients
60
Sunvozertinib
10.3 (8.3-14.0)
Chemotherapy
7.5 (6.7-8.5)
50
46.1
Hazard ratio for disease
40
33.2
progression or death,
30
0.65 (95% CI, 0.50-0.85)
Sunvozertinib
P<0.001
20
26.7
Chemotherapy
10
17.1
0
0
3
6
9
12
15
18
21
24
27
30
33
Months since Randomization
No. at Risk
Sunvozertinib
163
143
108
74
60
48
34
26
18
9
3
0
Chemotherapy 161
128
84
51
28
22
14
7
6
2
1
0
---
Table 2. Key Efficacy End Points.*
Sunvozertinib
Chemotherapy
Treatment Effect
End Point
(N=163)
(N=161)
(95% CI)T
P Value
Progression-free survival
Median (95% CI) - mo
10.3 (8.3-14.0)
7.5 (6.7-8.5)
0.65 (0.50-0.85)
<0.001
Percentage of patients (95% CI)
At 12 mo
46.1 (37.9-53.9)
26.7 (19.3-34.6)
NA
NA
At 18 mo
33.2 (25.3-41.3)
17.1 (10.7-24.7)
NA
NA
At 24 mo
23.0 (15.8-31.0)
10.3 (5.1-17.6)
NA
NA
Objective response:-
Percentage of patients (95% CI)
58.9 (50.9-66.5)
31.1 (24.0-38.8)
3.2 (2.0-5.0)
NA
Duration of response
Median (95% CI) - mo
11.2 (8.2-13.9)
7.1 (6.9-11.1)
NA
NA
Overall survival
Median (95% CI) — mo
29.8 (21.8-NE)
28.8 (20.7-NE)
0.99 (0.70-1.40)
0.48
Percentage of patients (95% CI)
At 18 mo
65.5 (56.9-72.9)
67.2 (58.4-74.5)
NA
NA
At 24 mo
57.4 (48.3-65.4)
56.2 (46.9-64.5)
NA
NA
At 30 mo
50.0 (39.4-59.6)
49.1 (39.4-58.1)
NA
NA
* The efficacy population included all the patients who had undergone randomization. NA denotes not applicable, and
NE could not be estimated.
t The treatment effect is shown as a hazard ratio for progression-free survival and overall survival and as an odds ratio
for objective response.
# Progression-free survival and objective response were assessed by blinded independent central review.
---
Drug
Sponsor
Study ID
Treatment regimen
Enrollment
Primary
Status
endpoint
Scope
Furmonertinib 240 mg (oral)
FURVENT /
Furmonertinib
R
Recruitment
Allist
NCT05607550
N=375
Furmonertinib 160 mg (oral)
375
PFS
1:1:1
completed
International
Platinum-based chemotherapy (IV)
WU-KONG 28 /
Sunvozertinib (oral)
Dizal
R
Primary readout
Sunvozertinib
N=320
320
PFS
NCT05668988
International
1:1
expected in 2026
Platinum-based chemotherapy (IV)
PLB1004 (oral)
Andamertinib
Avistone
NCT06281964
N=327
R
327
PFS
Active, recruiting
China only
(PLB1004)
1:1
Platinum-based chemotherapy (IV)
± sintilimab (IV)
Zipalertinib (oral) +
Taiho /
R
Platinum-based chemotherapy (IV)
Zipalertinib
NCT05973773
N=260
260
PFS
Active, recruiting
International
Cullinan
1:1
Chemotherapy (IV)
YK-029A (oral)
Suzhou
CTR20230490/
R
N=350
350
PFS
YK-029A
Recruiting
China only
Puhe
NCT05767892
1:1
Platinum-based chemotherapy (IV)
JMT101 (oral) + osimertinib (oral)
Shanghai
CTR20241252/
R
JMT101
N=398
398
PFS
Active, recruiting
China only
JMT-Bio
NCT06380348
1:1
Cisplatin (IV) + pemetrexed (IV)
Experimental arm
Control arm
IV: Intravenous
PFS: Progression-free survival
R
Randomization
---
Sequential treatment in the future?
Chemotherapy +
Amivantamab
EGFR ex20ins TKI
ADC +/- EGFR ex20ins TKI
EGFR ex20ins TKI
Chemotherapy +
ADC +/- EGFR ex20ins TKI
Amivantamab
EGFR ex20ins TKI +
Amivantamab
ADC +/- EGFR ex20ins TKI
Chemotherapy
Amivantamab +
Chemotherapy +/- EGFR
ADC +/- EGFR ex20ins TKI
EGFR ex20ins TKI ???
ex20ins TKI
WU-KONG28 Study Design
202
ANN
Sunvozertinib
(300 mg, once daily, orally)
Key Eligibility Criteria
Cytologically/histogicall
confirmed locally advanced or
Randomized at 1:1
metastatic non-sq NSCLC
Stratified by baseline
Documented EGFR exon20ins
brain metastasis (Y/N)
Newly diagnosed or treatment naïve
Platinum-based Chemotherapy
ECOG: 0 or 1
(Carboplatin, AUC5 + pemetrexed, 500
Sunvozertinib
PD
mg/m2, Q3W up to 6 cycles, followed by
(300 mg, once
Primary Endpoint:
pemetrexed maintenance therapy).
daily, orally)
PFS assessed by BICR a
intravenous infusion
Secondary Endpoints:
OS (Key secondary)
Crossover to sunvozertinib was allowed
PFS assessed by investigator
upon BICR-confirmed progressive disease
ORR, DCR, DoR, and tumor size change
Safety, Pharmacokinetics
Exploratory Endpoints:
PFS2 etc.
for analysis: January 16, 2026; Abbreviation: AUC, Area Under Curve; BICR, Blinded Independent Central Non-small Review; Cell DCR, Lung Disease Cancer; Contral ORR, Objective Rate; DoR, Response Duration of Rate: Response; OS, Overall ECOG, Survival; Eastern PFS, Co-
Data cut-off date primary EGFR, Epidermal Growth Factor Receptor; Exon20ins, Exon 20 Insertion Mutations; PFS2 is NSCLC, defined as the time from randomization to objective tumor progression on next line therapy based on
operative Progression Oncology Free Survival; Group; PFS2, Second Progression Free Survival; QD, Once Daily; Q3W, Every 3 Weeks;
I investigator Tumor assessment was conducted per RECIST 1.1 every 6 weeks in the first year and 12 weeks thereafter.
assessment or death from any cause, whichever comes first.
4
0 OS follow-up was conducted every 3 months.
ASCO
-
-
PRESENTED BY: Dr. John V. Heymach, MD, PhD
KNOWLEDGE CONQUERS CANCER
ASCO
#ASCO26
Presentation 5 property of the author and ASCO Permission required for revse, contact permissions@asong
AL MEETING
2026ASCO
ANNUAL MEETING
ASCO
ASCO
---
Primary Endpoint: BICR-assessed PFS
202
ANN
100
Median
Hazard Ratio
P Value
90
(95% CI)
(95% CI)
80
Sunvozertinib 10.3 (8.3, 14.0) 0.65 (0.50, 0.85) 0.0008
Chemotherapy 7.5 (6.7,8.5)
Percentage of Patients
70
60
46.1%
50
33.2%
40
Sunvozertinib
30
26.7%
20
17.1%
Chemotherapy
10
0
18
21
24
27
30
33
0
3
6
9
12
15
Months since Randomization
Number At Risk:
26
18
9
3
0
48
34
74
60
108
7
6
2
1
0
Sunvozertinib 163
143
28
22
14
84
51
Chemotherapy 161
128
6
Median follow-up time: 24.0 months in the sunvozertinib arm and 18.0 months in the chemotherapy arm.
KNOWLEDGE ASCO CONQUERS CANCER
- CINCA $400,000
2026
ASCO
#ASCO26
PRESENTED Presentation is property of the author and ASCO. Permission required for neuse, contact permissions@asce.org
BT: Dr. John V. Heymach, MD, PhD
AL MEETING
2026ASCO
ASCO
ANNUAL MEETING
ASCO
ASCO
O
---
BICR-assessed Tumor Response
2020
100
80
Sunvozertinib Armª
Partial Response
100
ANN
Stable Disease
Partal Persponse
Progressive Deease
80
Chemotherapy Arm
State Doease
60
Not Evaluable
Progressive Doease
60
Not Evaluable
Best Tumor Change from Baseline (%)
40
40
20
20
0
0
-20
-20
40
40
-60
-60
-80
cORR: 58.9%
-80
CORR: 31.1%
Median tumor size shrinkage: 42.1%
-100
-100
Median tumor size shrinkage: 24.7%
Sunvozertinib (N=163)
Chemotherapy (N=161)
Best Objective Response Rate, % (95% CI)
68.1 (60.4,75.2)
35.4 (28.0,43,3)
Confirmed Objective Response Rate, % (95% CI)
58.9(50.9,66.5)
31.1 (24.0, 38.8)
Odds Ratio (95% CI); P value
3.2 (2.0, 5.0); P<0.0001
Disease Control Rate, % (95% CI)
94.5 (89.8,97.4)
85.7 (79.3,90.7)
Calculated in patients with measurable target lesions at baseline assessed by BICR, including 158 patients in the sunvozertinib arm and 154 patients in the chemotherapy am.
8
2026
ASCO
PRE SENTED BY: Dr. John V. Heymach, MD, PhD
#ASCO26
ASCO
CINICAL ONCOLOGY
AL MEETING
Presentation is property of the author and ASCO. Permission required for чи, contact permissions@asco org
KNOWLEDGE CONQUERS CANCER
---
Second Progression Free Survival (PFS2)
2026ASC
ANNUAL MEET
100
Median
Hazard Ratio
P Value
90
(95% CI)
(95% CI)
80
Sunvozertinib 21.7 (16.1, 24.3) 0.70 (0.52, 0.95) 0.0111
73.6%
Chemotherapy 15.5 (13.4, 18.6)
70
Percentage of Patients
67.8%
60
55.8%
First subsequent systemic therapy
50
Sunvozertinib arm
40
44.0%
Sunvozertinib
46.6% (76/163) started subsequent therapy
30
72.4% (55/76) received chemotherapy
20
Chemotherapy
Chemotherapy arm
10
72.0% (116/161) started subsequent therapy
0
91.4% (106ª/116) received sunvozertinib
0
3
6
9
12
15
18
21
24
27
30
33
36
(90.2% through in-study crossover)
Months since Randomization
Number At Risk:
157
142
116
95
77
60
49
31
16
11
2
0
Sunvozertinib 163
153
142
117
83
60
46
31
24
13
6
1
0
Chemotherapy 161
time: 23.6 months in the sunvozertinib arm and 24.1 months in the chemotherapy arm.
Median follow-up defined as the time from the date of randomization to the time of second disease progression or death, whichever comes outside first, of after the the study first subsequent anti-cancer therapy.
10
PFS2 a Including is 101 patients (90.2%) who received sunvozertinib via in-study crossover and 5 patients who received sunvozertinib
ASCO
MOIOR
CINCE INCOLOGY
PRE SENTED BY: Dr. John V. Heymach, MD, PhD
2026 ASCO
ENOWLEDGE CONQUERS CANCER
#ASCO26
Presentation property of he author and ASCO. Permission required for reuse, contact permissions@asco.org
AL MEETING
2026ASCO
ANNUAL MEETING
ASCO
ASCO
O
2026
ASCO
NG
ANNUAL MEETING
Sunvozertinib Monotherapy versus Platinum-based
Chemotherapy as First-line Treatment for Advanced NSCLC
with EGFR Exon20ins: Primary Analysis of A Multinational
Phase 3 Randomized Study (WU-KONG28)
John V. Heymach1, Geoffrey Liu², Ligang Xing³, Laurent Greiller', John Thomas⁵, Ozan Yazic/5, Meil Sun Yun Fan*, Chengzhi Zhou
Mengzhao Wang Regan M Memmott Dariusz Kowalski¹, Catherine Shu¹³, Elaine Shum14, Elvire Pons-Tostivint Federica Bertolini
Gonzalo Fernandez Hinojan Lorenzo Antonuzzo¹⁸, Yiman Wang", Calcun Zhou
Department of Thoracic/Head and Neck Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX, the USA Department of Medical Oncology and
Hematology, University Health Network, Princess Margaret Cancer Centre, Toronto, ON, Canada; Department of Radution Ononiogy, Shandong Cancer Hospital and institute, Jhan, China, "Department of
Multidisciplinary Oncology and Therapeutic Innovations, Assistance Publique-Höpitaux de Marselle, Ax Marseile University, Marseille, France, Department of Medical Oncology, Peter MacCalium Cancer Centre,
Melbourne, Australia; Department of Medical Oncology, Gazi University Hospital, Arkara, Turkey, Department of Oncology, Jinan Central Hospital, Shandong University, Jhan, China, Department of Thoracic
Medical Oncology, Zhejang Cancer Hospital, Hangzhou, China; Department of Oncology, the First Affiliated Hospital of Guangzhou Medical University, Guangzhou, China, "Department of Respiratory and Critical
Care Medicine, Peking Union Medical College Hospital, Beijing, China; "Department of Internal Medicine, The Ohio State University James Comprehensive Cancer Center, Columbus, OM, the USA Department
USA; Division of Medical Oncology and Hematology, Perimuter Cancer Center, NYU Langone Health, New York, NY, the USA, "Department of Medical Oncology, Nantes University Hospital, Nantes, France
of Lung Cancer and Thoracic Tumors, Maria Sklodowska-Curie National Research institute of Onoology, Warsaw, Poland, "Department of Medicine, Columbia University inving Medical Center, New York, NY, the
"Division of Oncology, Department of Oncology and Hematology, Modena University Hospital, Modena, Italy, "Department of Medical Onoology, Clinica Universidad de Navama, Madrid, Spain; "Department of of
Experimental and Clinical Medicine, University of Florence, and the Medical Oncology Unit Careggi University Hospital, Florence, italy, "Dizal (Jangsu) Pharmaceutical Co. Ltd. Shanghai, China POepartment
Oncology, Shanghai Pulmonary Hospital; Shanghai East Hospital, Shanghai, China
PAL SENTED BY: Dr. John V. Heymach, MD, PhD
ASCO
2026 ASCO
#ASCO26
KNOWLEDGE COMQUARA CANCER
ANNUAL MEETING
I
importy
author
and ASCO
Person
2026ASCO
A
ANNUAL MEETING
A
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
A
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
A
ASCO
ASC
ASCO
ASCO
ASCO
ASCO
---
CO
Key Takeaways
EETING
EFFICACY
SAFETY
Sunvozertinib vs Chemotherapy
Sunvozertinib
WU-KONG28 met its primary endpoint: statistically significant
Safety profile similar to previous
and clinically meaningful PFS improvement with sunvozertinib
reports and manageable
Improved ORR and prolonged DoR with sunvozertinib
No new safety signals
2
2026 ASCO
ASCO26
PRESENTED BY Dr. John V. Heymach, MD, PhD
ASCO
ANNUAL MEETING
- - - and ABOD - - -
ENGWLEDGE CONDUERS CANCER
2026ASCO
ANNUAL MEETING
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
AS
A
ASCO
ASCO
ASCO
ASCO
ASCO
The NEW ENGLAND JOURNAL of MEDICINE
ORIGINAL ARTICLE
First-Line Sunvozertinib in NSCLC
with EGFR Exon 20 Insertion Mutations
Caicun Zhou,¹ L. Greillier,² G. Liu,³ T. John,⁴ L. Xing,⁵ D. Kowalski,6
R.M. Memmott,⁷ O. Yazici,⁸ M. Sun,⁹ C. Shu, 10 E. Pons-Tostivint, 11 Y. Fan, 12
G. Fernandez-Hinojal, 13 E. Shum,¹ 14 M. Wang, 15 F. Bertolini, 16 D.R. Camidge,¹⁷
Chengzhi Zhou, 18 L. Doucet, 19 Q. Hong, J. Fang,²¹ D. Huang, 22 B. Jin, Y. Yu, 24
L. Antonuzzo,²⁵ D. Moro-Sibilot, J. Bennouna, 27 G. de Castro, Jr., 28 L. Zheng,²⁹
and J.V. Heymach,30 for the WU-KONG28 Investigators*
100
Median
90
Progression-free
Survival
80
(95% CI)
70
mo
Percentage of Patients
60
Sunvozertinib
10.3 (8.3-14.0)
Chemotherapy
7.5 (6.7-8.5)
50
46.1
Hazard ratio for disease
40
33.2
progression or death,
30
0.65 (95% CI, 0.50-0.85)
Sunvozertinib
P<0.001
20
26.7
Chemotherapy
10
17.1
0
0
3
6
9
12
15
18
21
24
27
30
33
Months since Randomization
No. at Risk
Sunvozertinib 163
143
108
74
60
48
34
26
18
9
3
0
Chemotherapy 161
128
84
51
28
22
14
7
6
2
1
0
Figure 1. Progression-free Survival.
Shown are Kaplan-Meier estimates of progression-free survival as assessed by blinded independent central review
in the efficacy population, which included all the patients who had undergone randomization. The tick marks indi-
cate censoring of data.
WU-KONG28 Study Design
Sunvozertinib
(300 mg, once daily, orally)
Key Eligibility Criteria
Cytologically/histologically
confirmed locally advanced or
Randomized at 1:1
metastatic non-sq NSCLC
Stratified by baseline
Documented EGFR exon20ins
brain metastasis (Y/N)
Newly diagnosed or treatment naïve
Platinum-based Chemotherapy
ECOG: 0 or 1
(Carboplatin, AUC5 + pemetrexed, 500
Sunvozertinib
PD
mg/m2, Q3W up to 6 cycles, followed by
(300 mg, once
Primary Endpoint:
pemetrexed maintenance therapy),
daily, orally)
PFS assessed by BICR a
intravenous infusion
Secondary Endpoints:
OS (Key secondary)
Crossover to sunvozertinib was allowed
PFS assessed by investigator a
upon BICR-confirmed progressive disease
ORR, DCR, DoR, and tumor size change
Safety, Pharmacokinetics
Exploratory Endpoints:
PFS2 etc.
Data cut-off date for primary analysis: January 16, 2026; Abbreviation: AUC, Area Under Curve; BICR, Blinded Independent Central Review; DCR, Disease Contral Rate; DoR, Duration of Response; ECOG, Eastern Co-
operative Oncology Group; EGFR, Epidermal Growth Factor Receptor; Exon20ins, Exon 20 Insertion Mutations; NSCLC, Non-small Cell Lung Cancer; ORR, Objective Response Rate; OS, Overall Survival; PFS,
Progression Free Survival; PFS2, Second Progression Free Survival; QD, Once Daily; Q3W, Every 3 Weeks; PFS2 is defined as the time from randomization to objective tumor progression on next line therapy based on
Investigator assessment or death from any cause, whichever comes first.
a
Tumor assessment was conducted per RECIST 1.1 every 6 weeks In the first year and 12 weeks thereafter.
4
b
OS follow-up was conducted every 3 months.
2026 ASCO
PRESENTED BY: Dr. John V. Heymach, MD, PhD
#ASCO26
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse; contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
Primary Endpoint: BICR-assessed PFS
100
Median
Hazard Ratio
P Value
90
(95% CI)
(95% CI)
80
Sunvozertinib
10.3 (8.3, 14.0)
0.65 (0.50, 0.85)
0.0008
Percentage of Patients
70
Chemotherapy
7.5 (6.7, 8.5)
60
50
46.1%
40
33.2%
30
Sunvozertinib
20
26.7%
10
17.1%
0
Chemotherapy
0
3
6
9
12
15
18
21
24
27
30
33
Months since Randomization
Number At Risk:
Sunvozertinib 163
143
108
74
60
48
34
26
18
9
3
0
Chemotherapy 161
128
84
51
28
22
14
7
6
2
1
0
Median follow-up time: 24.0 months in the sunvozertinib arm and 18.0 months In the chemotherapy arm.
6
2026 ASCO
PRESENTED BY: Dr. John V. Heymach, MD, PhD
#ASCO26
ASCO
AMERICAN SOCIETY OF
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse; contact permissions@asco.or
CLINICAL ONCOLOGY
KNOWLEDGE CONQUERS CANCER
---
Subgroup Analysis of BICR-assessed PFS
Subgroup
No. of Events/Patients
Hazard Ratio(95%CI)
Sunvozertinib
Chemotherapy
Overall
111/163
115/161
0.65 (0.50, 0.85)
Age Group
<65 years
66/89
71/93
0.62 (0.44, 0.87)
>65 years
45/74
44/68
0.71 (0.46, 1.07)
Sex
Female
54/87
70/105
0.68 (0.48, 0.97)
Male
57/76
45/56
0.58 (0.39,0.85)
Race
Asian
77/102
79/102
0.56 (0.41, 0.77)
Non-Asian
34/61
36/59
0.93 (0.58,1.48)
Region
North America EU
27/50
33/52
0.78 (0.47, 1.30)
Others
84/113
82/109
0.62 (0.45,0.84)
Smoking History
Never
64/101
74/107
0.61 (0.43,0.85)
Ever
47/62
41/54
0.73 (0.48,1.11)
Baseline ECOG
0
28/46
26/43
0.77 (0.45,1.31)
>1
83/117
89/118
0.62 (0.46,0.84)
Brain Metastasis at Baseline
With
14/21
12/20
0.96 (0.44, 2.08)
Without
97/142
103/141
0.62 (0.47,0.83)
EGFR Exon20ins Subtype
769 ASV
34/51
39/52
0.46 (0.29,0.73)
770_SVD
15/21
19/32
Other/Unknown
62/91
57/77
0.77 (0.53,1.10)
EGFR Exon20ins Region
Near loop
77/111
79/109
0.59(0.43,0.82)
Far loop
28/41
30/43
0.83 (0.49, 1.38)
C-helix/Unknown
6/11
6/9
Disease Related Surgery
With
21/34
19/31
0.55 (0.29, 1.02)
Without
90/129
96/130
0.69 (0.51,0.92)
0.2
1
2
4.5
Favors Sunvozertinib
Favors Chemotherapy
7
2026 ASCO
PRE SENTED BY: Dr. John V. Heymach, MD, PhD
#ASCO26
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse: contact permissions@asco.or
KNOWLEDGE CONQUERS CANCER
---
Interim Analysis of Overall Survival
100
Median
90
(95% CI)
Sunvozertinib 29.8 (21.8, NE)
80
Chemotherapy 28.8 (20.7, NE)
70
Percentage of Patients
60
Sunvozertinib
os data maturity
50
38.9% (126/324)
40
Chemotherapy
38.0% (62/163) in the sunvozertinib arm
30
39.8% (64/161) in the chemotherapy arm
20
In-study crossover
10
90.2% (101/112) patients with BICR-
0
confirmed progressive disease crossed
0
3
6
9
12
15
18
21
24
27
30
33
36
39
over to receive sunvozertinib treatment
Months since Randomization
Number At Risk:
Sunvozertinib 163
158
149
132
108
92
76
67
60
40
21
8
2
0
Chemotherapy 161
154
147
134
113
97
79
62
55
40
24
10
2
0
Median follow-up time: 26.1 months in the sunvozertinib arm and 26.7 months in the chemotherapy arm.
11
2026 ASCO
PRE SENTED BY: Dr. John V. Heymach, MD, PhD
#ASCO26
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
Primary Endpoint: BICR-assessed PFS
100
Median
Hazard Ratio
P Value
90
(95% CI)
(95% CI)
80
Sunvozertinib 10.3 (8.3, 14.0) 0.65 (0.50, 0.85) 0.0008
Percentage of Patients
70
Chemotherapy
7.5 (6.7, 8.5)
60
50
46.1%
40
33.2%
30
Sunvozertinlb
20
26.7%
17.1%
10
Chemotherapy
0
0
3
6
9
12
15
18
21
24
27
30
33
Months since Randomization
Number At Risk:
Sunvozertinib 163
143
108
74
60
48
34
26
18
9
3
0
Chemotherapy 161
128
84
51
28
22
14
7
6
2
1
0
Median follow-up time: 24.0 months in the sunvozertinib arm and 18.0 months in the chemotherapy arm.
6
2026 ASCO
PRE SENTED BY: Dr. John V. Heymach, MD, PhD
#ASCO26
ASCO
AMERICAN SOCIETY OF
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco.org org.
KNOWLEDGE CONQUERS CANCER
---
BICR-assessed Tumor Response
Partial Response
100
Stable Disease
Partial Response
Chemotherapy Armᵃ
Progressive Disease
100
Stable Disease
80
Not Evaluable
Sunvozertinib Armᵃ
Progressive Disease
80
Not Evaluable
60
60
40
Best Tumor Change from Baseline (%)
40
20
20
0
0
-20
-20
-40
-40
-60
-60
cORR: 31.1%
cORR: 58.9%
-80
-80
Median tumor size shrinkage: 24.7%
Median tumor size shrinkage: 42.1%
-100
-100
Sunvozertinib (N=163)
Chemotherapy (N=161)
Best Objective Response Rate, % (95% CI)
68.1 (60.4, 75.2)
35.4 (28.0, 43.3)
Confirmed Objective Response Rate, % (95% CI)
58.9 (50.9, 66.5)
31.1 (24.0, 38.8)
Odds Ratio (95% CI); P value
3.2 (2.0, 5.0); P<0.0001
Disease Control Rate, % (95% CI)
94.5 (89.8, 97.4)
85.7 (79.3, 90.7)
Calculated in patients with measurable target lesions at baseline assessed by BICR, including 158 patients in the sunvozertinib arm and 154 patients in the chemotherapy arm.
8
ASCO
#ASCO26
PRE SENTED BT: Dr. John V. Heymach, MD, PhD
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
---
Second Progression Free Survival (PFS2)
100
Median
Hazard Ratio
P Value
90
(95% CI)
(95% CI)
80
Sunvozertinib 21.7 (16.1, 24.3) 0.70 (0.52, 0.95) 0.0111
73.6%
Chemotherapy
15.5 (13.4, 18.6)
70
Percentage of Patients
67.8%
60
55.8%
First subsequent systemic therapy
50
Sunvozertinib arm
40
44.0%
Sunvozertinib
46.6% (76/163) started subsequent therapy
30
72.4% (55/76) received chemotherapy
20
Chemotherapy
Chemotherapy arm
10
72.0% (116/161) started subsequent therapy
0
0
3
6
9
12
15
18
21
24
27
30
33
36
91.4% (106a/116) received sunvozertinib
(90.2% through in-study crossover)
Months since Randomization
Number At Risk:
Sunvozertinib 163
157
142
116
95
77
60
49
31
16
11
2
0
Chemotherapy 161
153
142
117
83
60
46
31
24
13
6
1
0
Median follow-up time: 23.6 months in the sunvozertinib arm and 24.1 months in the chemotherapy arm.
PFS2 is defined as the time from the date of randomization to the time of second disease progression or death, whichever comes first, after the first subsequent anti-cancer therapy.
a Including 101 patients (90.2%) who received sunvozertinib via in-study crossover and 5 patients who received sunvozertinib outside of the study
10
2026 ASCO
#ASCO26
PRESENTED BY: Dr. John V. Heymach, MD, PhD
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse; contact permissions@asco.org.
KNOWLEDGE CONQUERS CANCER
---
Subsequent Treatment
Sunvozertinib Arm
Chemotherapy Arm
100
100
90
90
80
80
70
57.8
63.9
64.5
70
1 line
73.0
With
1 line
60
Discontinued
60
84.5
85.3
Patients (%)
50
Patients (%)
Discontinued
With
50
40
40
30
30
23.3
2 lines
25.0
20
36.1
2 lines
20
27.0
Without
10
Ongoing
10
15.5
10.5
14.7
19.0
Ongoing
Without
>3 lines
23 lines
0
0
Sunvozertinib
Subsequent Therapy
Lines of Subsequent Therapy
Chemotherapy
Subsequent Therapy
Lines of Subsequent Therapy
(N=163)
(N=119)
(N=76)
(N=161)
(N=136)
(N=116)
Types of subsequent therapies included amivantamab, antiangiogenic therapy, chemotherapy, immunotherapy, targeted therapy (e.g., sunvozertinib and
other EGFR TKI) and Other
12
2026 ASCO
#ASCO26
PRESENTED BY: Dr. John V. Heymach, MD, PhD
ASCO
AMERICAN SOCIETY OF
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco.org org.
CLINICAL ONCOLOGY
KNOWLEDGE CONQUERS CANCER
Therapeutic advances in EGFR ex20 ins mutations
EXCLAIM
EXCLAIM-2
Accelerated approval
Mobocertinib vs
mobocertinib
Chemo
Structural basis
PFS:9.6v9.6m
resistance to 1G
Tmi
(months)
EGFR TKI in Ex20
CHRYSALIS
insertions
Accelerated approval
Roubichoux et al.
WU-KONG 1B
Yasuda STM 2013
- amivantamab
Structural-functional
Accelerated approval
(monotherapy)
basis classification
Sunvozertinib 200 mg
2013
2015
2017
2019
2021
2023
2024
2025
2026
Yang et al. Role of
Osimertinib 160 mg OM
PAPILLON
FAVOUR
WU-KONG 28
afatinib in uncommon
POSITION20
SoC chemo-
Firmonertinib
Phase III
mutations (LUX-2,
ORR 28% mPFS 6.8 m
amivantamab
ORR 78.6%
Sunvozertinib 300 mg
LUX-3, LUX-6)
ECOG ACRIN EA5162
mDoR 15.2 m
vs chemo
- 3 cohorts: Exon 20
ins/atypicals/ T790M
ORR 24%, mPFS 9.6 m
Limited efficacy for
/
-
afatinib in exon 20 ins
2026 ASCO
#ASCO26
PRESENTED BY: Daniel SW Tan. National Cancer Centre Singapore
ASCO
AMERICAN SOCIETY O
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation property of the author and ASCO Permission required for num
KNOWLEDGE CONQUERS CANCER
WU-KONG28 Study Design
Sunvozertinib
Key Eligibility Criteria
(300 mg, once daily, orally)
Cytologically/histogicall
confirmed locally advanced or
Randomized at 1:1
metastatic non-sq NSCLC
Stratified by baseline
Documented EGFR exon20ins
brain metastasis (Y/N)
Newly diagnosed or treatment naive
ECOG: 0 or 1
Platinum-based Chemotherapy
(Carboplatin, AUC5 + pemetrexed, 500
Sunvozertinib
PD
mg/m2, Q3W up to 6 cycles, followed by
Primary Endpoint:
(300 mg, once
PFS assessed by BICR a
pemetrexed maintenance therapy).
daily, orally)
intravenous infusion
Secondary Endpoints:
OS (Key secondary) b
Crossover to sunvozertinib was allowed
PFS assessed by investigator ᵃ
upon BICR-confirmed progressive disease
ORR, DCR, DoR, and tumor size change
Safety, Pharmacokinetics
Exploratory Endpoints:
PFS2 etc.
Data cut-off date for primary analysis: January 16, 2026; Abbreviation: AUC, Area Under Curve; BICR, Blinded Independent Central Review; DCR, Disease Contral Rate; DoR, Duration of Response; ECOG, Eastern Co-
operative Oncology Group; EGFR, Epidermal Growth Factor Receptor; Exon20ins, Exon 20 Insertion Mutations; NSCLC, Non-small Cell Lung Cancer; ORR, Objective Response Rate; os, Overall Survival; PFS,
Progression Free Survival; PFS2, Second Progression Free Survival; QD, Once Daily; Q3W, Every 3 Weeks; PFS2 is defined as the time from randomization to objective tumor progression on next line therapy based on
investigator assessment or death from any cause, whichever comes first.
a Tumor assessment was conducted per RECIST 1.1 every 6 weeks in the first year and 12 weeks thereafter.
b OS follow-up was conducted every 3 months.
PRESENTED BY: Dr. John V. Heymach, MD, PhD
ASCO
AMERICAN
CUNICAL
2026
ASCO
#ASCO26
KNOWLEDGE CONQUERS
NNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
---
Second Progression Free Survival (PFS2)
100
Median
Hazard Ratio
P
Value
90
(95% CI)
(95% CI)
80
Sunvozertinib 21.7 (16.1, 24.3) 0.70 (0.52, 0.95) 0.0111
73.6%
Chemotherapy
15.5 (13.4, 18.6)
70
Percentage of Patients
67.8%
60
55.8%
First subsequent systemic therapy
50
Sunvozertinib arm
40
44.0%
Sunvozertinib
46.6% (76/163) started subsequent therapy
30
72.4% (55/76) received chemotherapy
20
Chemotherapy
Chemotherapy arm
10
72.0% (116/161) started subsequent therapy
0
9
12
15
18
21
24
27
30
33
36
91.4% (106a/116) received sunvozertinib
0
3
6
(90.2% through in-study crossover)
Months since Randomization
Number At Risk:
Sunvozertinib 163
157
142
116
95
77
60
49
31
16
11
2
0
Chemotherapy 161
153
142
117
83
60
46
31
24
13
6
1
0
Median follow-up time: 23.6 months in the sunvozertinib arm and 24.1 months in the chemotherapy arm.
PFS2 is defined as the time from the date of randomization to the time of second disease progression or death, whichever comes first, after the first subsequent anti-cancer therapy
10
a Including 101 patients (90.2%) who received sunvozertinib via in-study crossover and 5 patients who received sunvozertinib outside of the study
2026 ASCO
PRESENTED BY: Dr. John V. Heymach, MD, PhD
ASCO
AMERICAN SOCIETY of
CUMICAL OHCOLOGY
#ASCO26
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco.org.
KNOWLEDGE CONQUERS CANCER
---
Overview of Safety
Sunvozertinib
Chemotherapy
(N=163)ᵃ
(N=150)ᵃ
Participants with Any TRAE
163 (100.0)
146 (97.3)
Any TRAE with Grade ≥3
100 (61.3)
74 (49.3)
Any Treatment-related SAE
30 (18.4)
19 (12.7)
Any TRAE Leading to Dose Interruption
74 (45.4)
41 (27.3)
Any TRAE Leading to Dose Reduction
66 (40.5)
36 (24.0)
Any TRAE Leading to Treatment Discontinuation
12 (7.4)
17 (11.3)
Any TRAE with Fatal Outcome
0 (0.0)
1 (0.7)b
In the sunvozertinib arm, the top TRAEs leading to dose interruption and reduction included blood CPK increased and
diarrhea, which did not lead to treatment discontinuation.
Abbreviation: SAE, Serious Adverse Event; TRAE, Treatment-related Adverse Event. TRAEs included any events considered as related to the randomized treatment.
a only included patients who received randomized treatment; b The drug-related TEAE with fatal outcome in the chemotherapy arm was pneumonia.
13
2026 ASCO
#ASCO26
PRESENTED BY: Dr. John V. Heymach, MD, PhD
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco.org
ASCO
AMERICAN GOCETY OF
CLINICAL CHICOLOGE
KNOWLEDGE CONQUERS CANCER
Overview of Safety
Sunvozertinib
Chemotherapy
(N=163)ᵃ
(N=150)a
Participants with Any TRAE
163 (100.0)
146 (97.3)
Any TRAE with Grade ≥3
100 (61.3)
74 (49.3)
Any Treatment-related SAE
30 (18.4)
19 (12.7)
Any TRAE Leading to Dose Interruption
74 (45.4)
41 (27.3)
Any TRAE Leading to Dose Reduction
66 (40.5)
36 (24.0)
Any TRAE Leading to Treatment Discontinuation
12 (7.4)
17 (11.3)
Any TRAE with Fatal Outcome
0 (0.0)
1 (0.7)b
In the sunvozertinib arm, the top TRAEs leading to dose interruption and reduction included blood CPK increased and
diarrhea, which did not lead to treatment discontinuation.
Abbreviation: SAE, Serious Adverse Event; TRAE, Treatment-related Adverse Event. TRAEs included any events considered as related to the randomized treatment.
13
a only included patients who received randomized treatment; b The drug-related TEAE with fatal outcome in the chemotherapy arm was pneumonia.
2026 ASCO
#ASCO26
PRESENTED BY: Dr. John V. Heymach, MD, PhD
ASCO
AMERICAN SOCIETY OF
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation
KNOWL EDGE CONQUERS ANCER
---
Common Treatment-related Adverse Events (≥ 20%)
Sunvozertinib (N=163)
Chemotherapy (N=150)
All Grade
≥ Grade 3
All Grade
≥ Grade 3
Participants with Any TRAE
163 (100.0)
100 (61.3)
146 (97.3)
74 (49.3)
Diarrhea
137 (84.0)
22 (13.5)
15 (10.0)
0 (0.0)
Blood creatine phosphokinase increased
90 (55.2)
33 (20.2)
5 (3.3)
1 (0.7)
Rash
84 (51.5)
1 (0.6)
8 (5.3)
0 (0.0)
Paronychia
79 (48.5)
6 (3.7)
0 (0.0)
0 (0.0)
Anemia
75 (46.0)
10 (6.1)
91 (60.7)
15 (10.0)
Weight decreased
56 (34.4)
5 (3.1)
15 (10.0)
1 (0.7)
Decreased appetite
52 (31.9)
1 (0.6)
39 (26.0)
2 (1.3)
Blood creatinine increased
50 (30.7)
1 (0.6)
12 (8.0)
0 (0.0)
Vomiting
40 (24.5)
3 (1.8)
32 (21.3)
3 (2.0)
Nausea
38 (23.3)
3 (1.8)
66 (44.0)
2 (1.3)
Aspartate aminotransferase increased
35 (21.5)
3 (1.8)
52 (34.7)
1 (0.7)
Lipase increased
35 (21.5)
9 (5.5)
8 (5.3)
1 (0.7)
Amylase increased
34 (20.9)
2 (1.2)
11 (7.3)
0 (0.0)
Alanine aminotransferase increased
25 (15.3)
2 (1.2)
50 (33.3)
2 (1.3)
Neutrophil count decreased
22 (13.5)
4 (2.5)
68 (45.3)
28 (18.7)
White blood cell count decreased
20 (12.3)
1 (0.6)
58 (38.7)
10 (6.7)
Platelet count decreased
11 (6.7)
2 (1.2)
32 (21.3)
10 (6.7)
Constipation
4 (2.5)
0 (0.0)
30 (20.0)
0 (0.0)
14
2026 ASCO
#ASCO26
PRESENTED BY: Dr. John V. Heymach, MD, PhD
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
Conclusion
In the primary analysis of WU-KONG28 study, sunvozertinib demonstrated significantly superior anti-
tumor efficacy than platinum-containing chemo doublet in 1L advanced NSCLC patients with EGFR
exon20ins:
Statistically significant and clinically meaningful improvement in PFS (mPFS: 10.3 VS 7.5 months;
HR: 0.65; P=0.0008)
Higher ORR (58.9% VS 31.1%) and DCR (94.5% VS 85.7%), and longer DoR (11.2 VS 7.1 months)
The OS data were immature (38.9% maturity). The PFS2 suggested a long-term survival benefit
with sunvozertinib (21.7 months VS 15.5 months)
The common TRAEs of sunvozertinib were related to wild-type EGFR inhibition and clinically
manageable
These results support sunvozertinib as first-line treatment for NSCLC patients with EGFR exon20ins,
with the advantage of a single oral agent
15
2026 ASCO
PRESENTED BY: Dr. John V. Heymach, MD, PhD
ASCO
AMERICAN SOCIETY OF
#ASCO26
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissiona@asco.org
KNOWLEDGE CONQUERS CANCER
WU-KONG28 (NCT05668988) is the first multinational, confirmatory Phase 3 randomized trial evaluating oral sunvozertinib monotherapy against platinum-pemetrexed chemotherapy as first-line treatment for advanced non-squamous NSCLC harboring EGFR exon 20 insertion mutations — a population historically underserved by classical EGFR TKIs. At ASCO 2026 (abstract LBA8500), the trial met its primary endpoint of blinded independent central review–assessed progression-free survival, with results published simultaneously in the New England Journal of Medicine. Sunvozertinib already holds FDA accelerated approval for previously treated EGFR exon20ins NSCLC and FDA Breakthrough Therapy Designation in the first-line setting; WU-KONG28 is the confirmatory study supporting potential first-line use.
Oral sunvozertinib 300 mg once daily vs carboplatin/pemetrexed with optional pemetrexed maintenance.
Primary Endpoint
Progression-free survival by blinded independent central review (RECIST 1.1).
Key Secondary
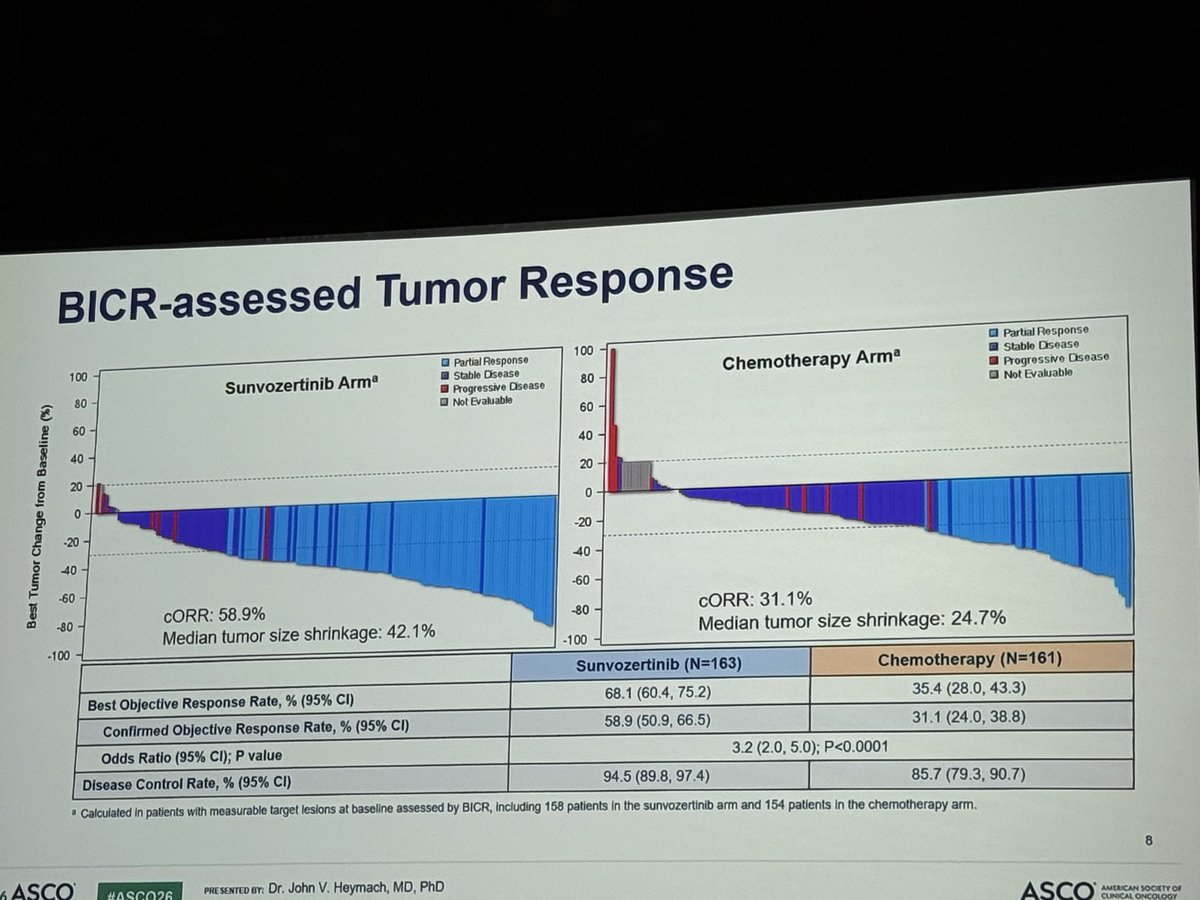
Overall survival, objective response rate (ORR), and duration of response (DOR).
Efficacy & Safety
Reported Results
Progression-Free Survival (Primary Endpoint)
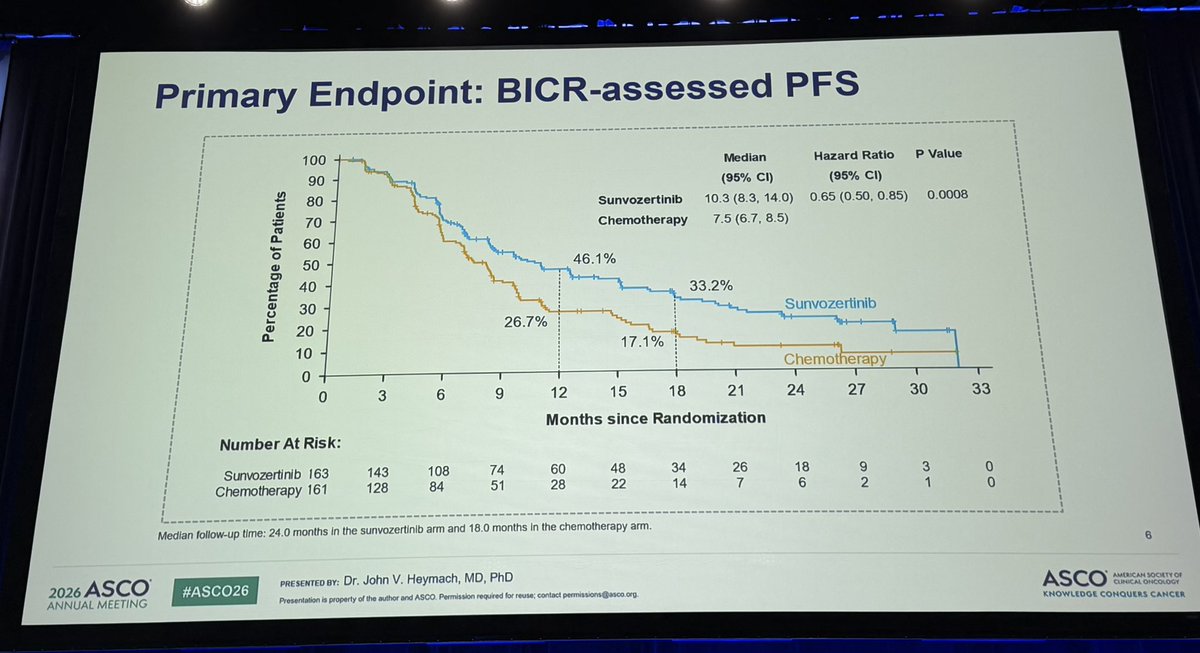
Sunvozertinib significantly improved median PFS to 10.3 months vs 7.5 months for chemotherapy (HR 0.65; 95% CI, 0.50–0.85; p=0.0008). The 12-month PFS rate was 46.1% vs 26.7%.
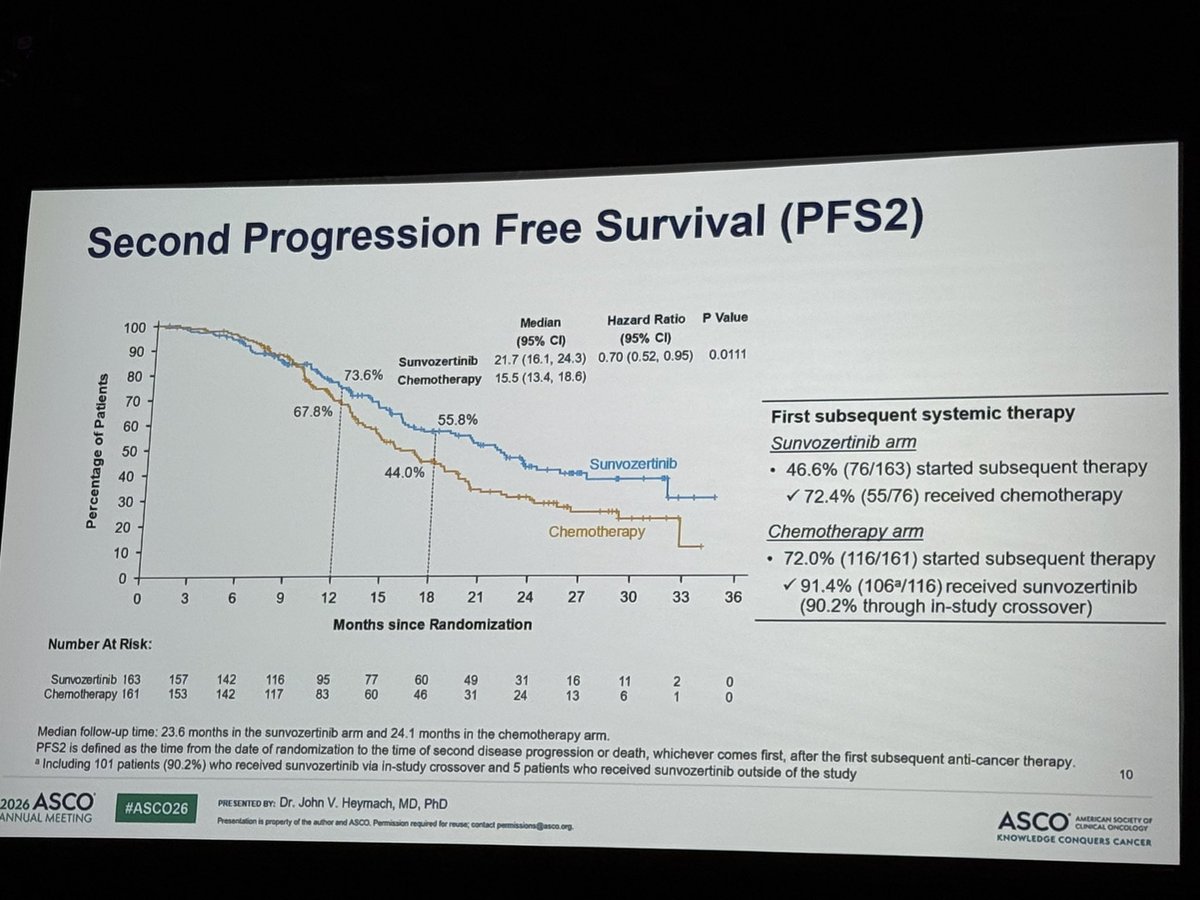
PFS2 — time from randomization to second progression or death — was a prespecified exploratory endpoint (not a secondary endpoint). In the ASCO oral presentation (LBA8500), median PFS2 was 21.7 months (95% CI, 16.1–24.3) with sunvozertinib vs 15.5 months (13.4–18.6) with chemotherapy (HR 0.70; 95% CI, 0.52–0.95; p=0.0111), suggesting the first-line benefit persists beyond initial progression — relevant context given that crossover to sunvozertinib was permitted, which dilutes the overall-survival comparison.
At the interim analysis (38.9% maturity), median OS was 29.8 months (95% CI, 21.8–NE) with sunvozertinib vs 28.8 months (20.7–NE) with chemotherapy — HR 0.99 (95% CI, 0.70–1.40; p=0.48), i.e. no separation yet. This is expected: 90.2% of chemotherapy patients with confirmed progression crossed over to sunvozertinib, which heavily confounds the OS comparison. OS remains immature and follow-up is ongoing.
Sunvozertinib was administered as an all-oral, chemotherapy-free regimen. Full adverse-event profiles from the Phase 3 dataset are reported in the NEJM publication; diarrhea and skin-related events are the class-typical EGFR-TKI toxicities discussed by KOLs. CNS coverage in monotherapy was raised as an open question (@TejasPatilMD).
STATUSSunvozertinib (Zegfrovy): approved in 2nd-line, investigational in 1st-line
Sunvozertinib holds FDA accelerated approval for adults with locally advanced or metastatic EGFR exon 20 insertion–positive NSCLC whose disease progressed on or after platinum-based chemotherapy (previously-treated setting). For the first-line setting evaluated in WU-KONG28, sunvozertinib has FDA Breakthrough Therapy Designation but is not yet approved — WU-KONG28 is the confirmatory Phase 3 trial supporting a potential first-line indication.
DEALAstraZeneca to globally develop & commercialize Zegfrovy
On July 14, 2026, AstraZeneca entered an exclusive global license agreement with Dizal Pharmaceutical for Zegfrovy (sunvozertinib), acquiring worldwide rights to develop and commercialize the drug. AstraZeneca will pay Dizal $600M upfront plus up to $900M in development, regulatory and sales-related milestones, plus tiered royalties on global sales. The transaction is expected to close in the second half of 2026. The agreement follows the positive first-line WU-KONG28 readout presented at ASCO 2026 and published in NEJM.