1L EGFR-mutant NSCLC - AstraZeneca
Discover KOL Sentiment on FLAURA2 →Design - Phase 3 osimertinib + platinum-pemetrexed chemotherapy vs osimertinib monotherapy, first-line EGFR-mutated advanced NSCLC (NCT04035486).
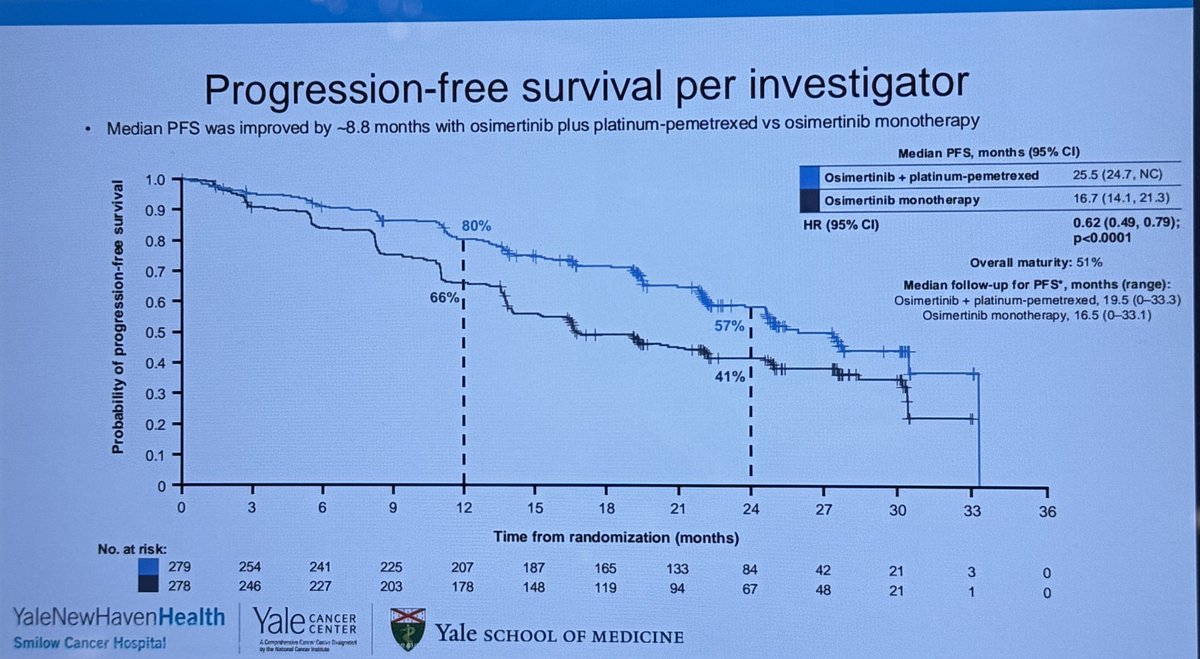
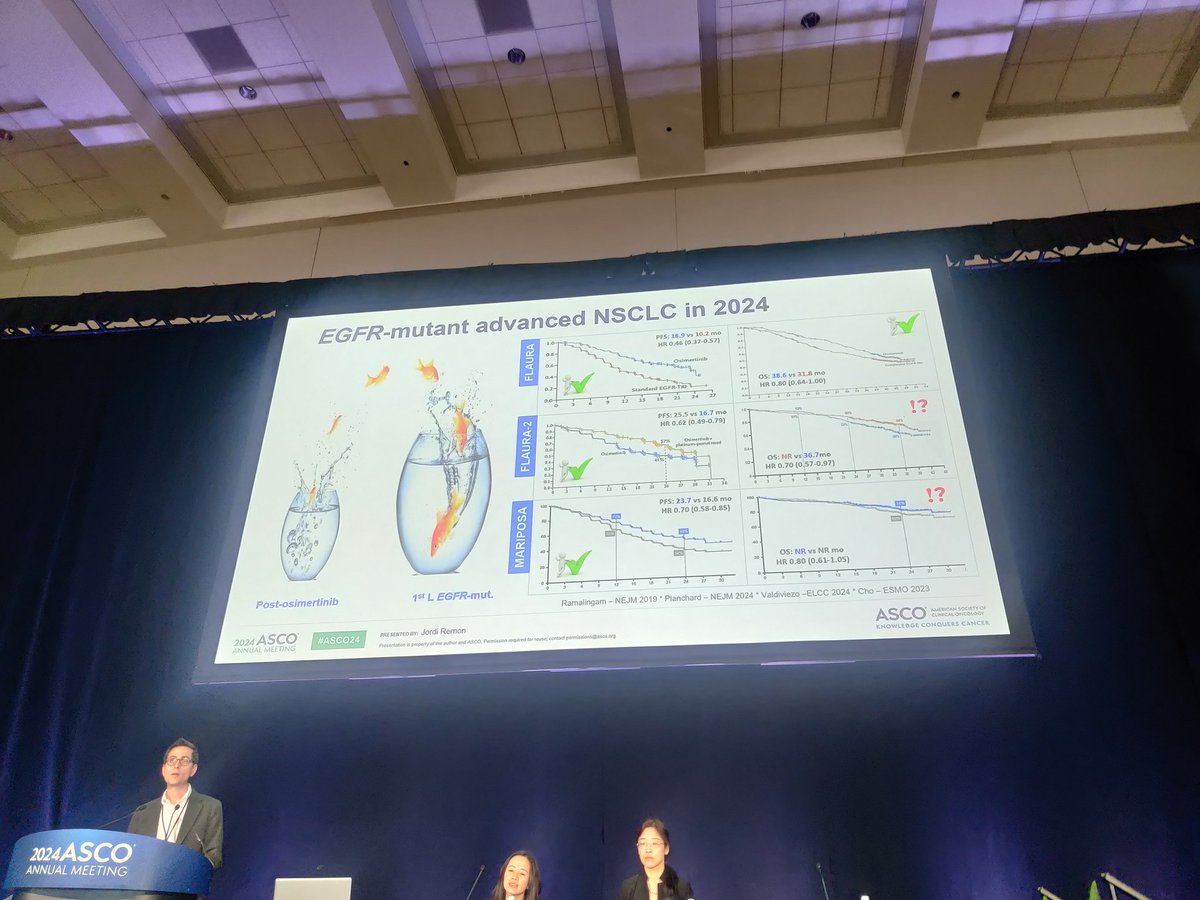
PFS (primary) - Median 25.5 vs 16.7 mo, HR 0.62 - a 38% reduction in risk of progression or death.
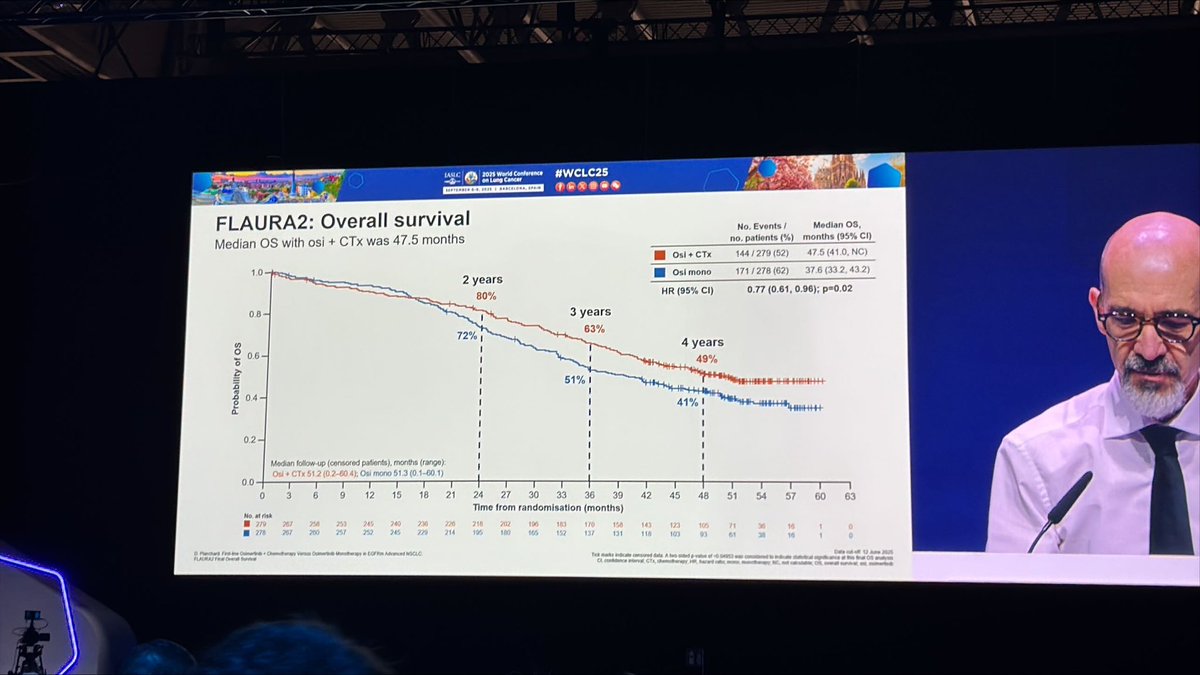
OS - Final median 47.5 vs 37.6 mo, HR 0.77 (p=0.02); 3-year OS 63% vs 51%.
Safety - Grade 3+ AEs 70% vs 34% (chemotherapy-driven myelosuppression); osimertinib discontinuation 12% vs 7%.
Regulatory - FDA approved February 16, 2024.
Sponsor / drug - AstraZeneca; osimertinib (Tagrisso) + chemotherapy.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.



























Top 10 by impressions - click to view on X
FDA has no standards Approving chemo + Osi based on FLAURA2 is a terrible decision Osi -> chemo may have similar or better OS with better QoL. FDA has no clue. They are permitting an option...
So much awaited data of flaura2 .29 .4 months. Very good PFS for CNS mets also. 24.9 months . But no OS as of now . Is more toxicity justified if NO OS ? @JackWestMD...
FLAURA2 now FDA approved. It’s the biggest change in this space for some years. I’ll be fascinated to see how this gets used. All comers? Brain mets predominantly? Many patients welcome the...
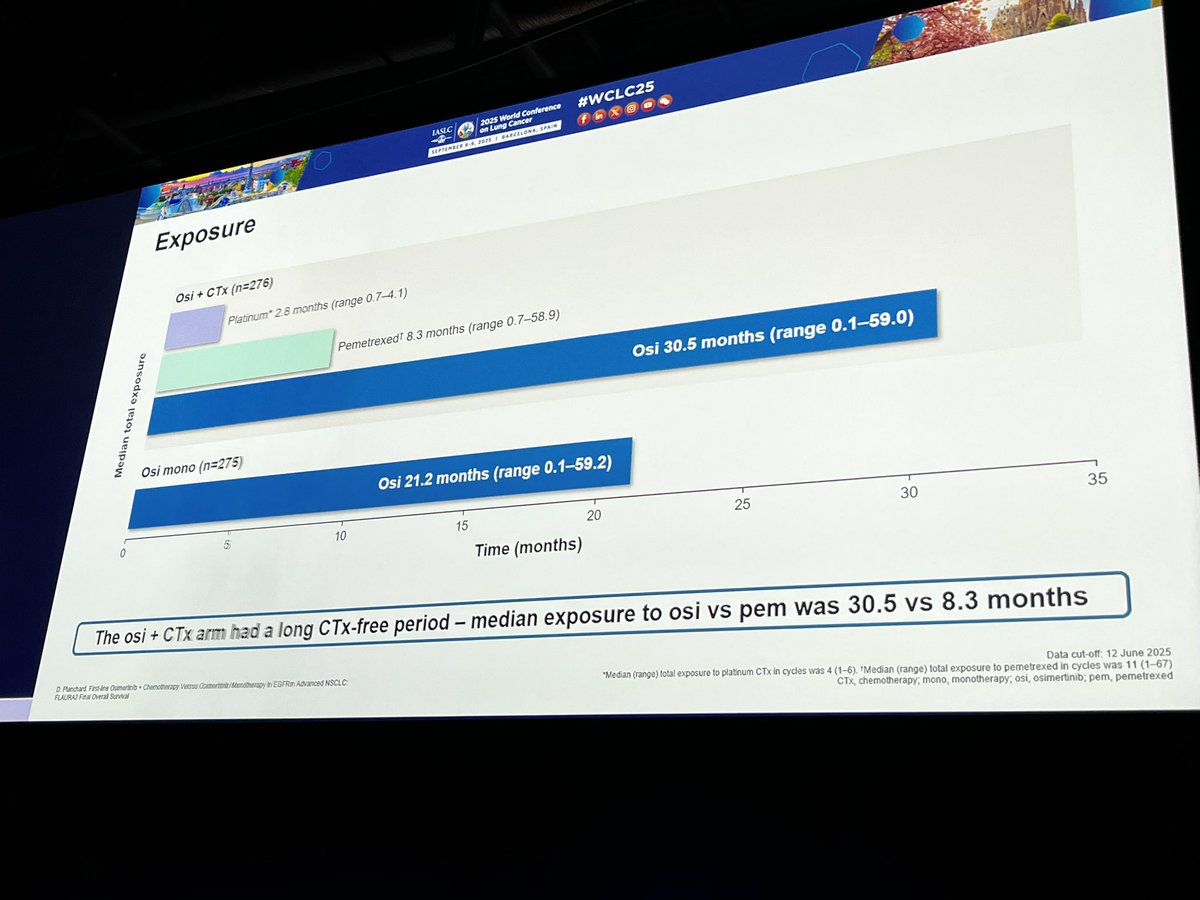
Dr. @dplanchard at #WCLC25 with highly anticipated Presidential Plenary presentation with OS results from FLAURA2: first line chemo + osimertinib improves OS from 37.6 to...
FLAURA2 regimen raises the bar! New data from a China study shows impressive PFS/OS gains for Osi + Chemo in EGFRm + TP53 co-mutated pts. Confirms 1L SOC status across the board: TP53 mut, WT, and...

Original Article: Survival with Osimertinib plus Chemotherapy in EGFR-Mutated Advanced NSCLC (FLAURA2 phase 3 trial) #ESMO25 | @myESMO
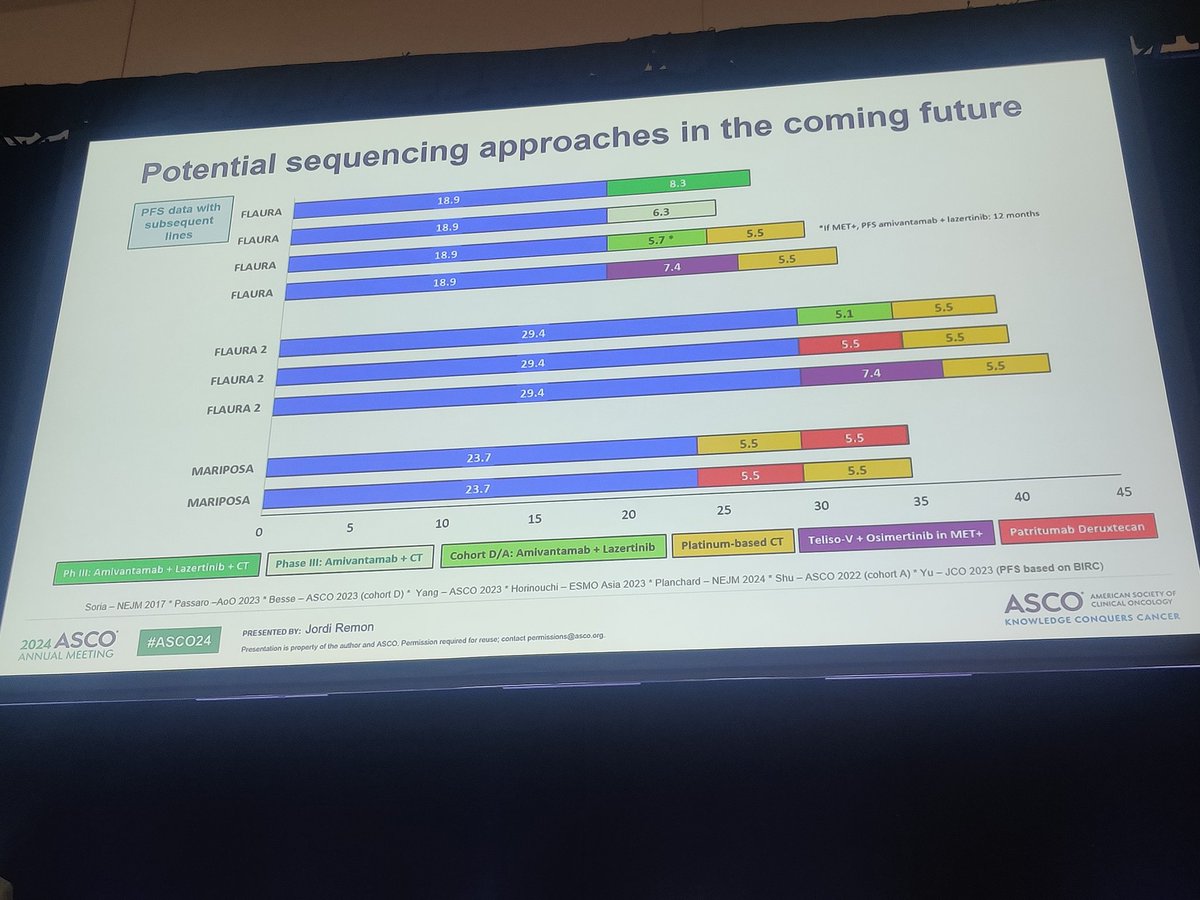
EGFR update 7 potential options: •3rd gen TKI: osimertinib, lazertinib, aumolertinib •Amivantamab •Pemetrexed •Carboplatin •Ivonescimab •Dato-DXd OS data favor combos upfront—but real-world ≠ trial....

Same phenomenon occurs in #MARIPOSA as noted by Dr. @harpreet_md in #FLAURA2 - its minor but perhaps early increase toxicity with intensified treatment is...

@jillfeldman4 @EGFRResisters @OncoAlert @IASLC @RManochakian @CharuAggarwalMD @christine_lovly @LungCancerRx LOVE that this was...
🔥🚨Hot Off the Press #BigNews Press Release by @AstraZeneca ⭐️#FLAURA2 trial of #Osimertinib + #Chemotherapy vs...
FLAURA2 is a clinical trial evaluating Osimertinib + platinum-based chemotherapy in 1L EGFR-mutant advanced NSCLC. Sponsored by AstraZeneca. KOL discussion spans multiple conferences with 152 tracked posts from 73 oncology opinion leaders generating 549.4K total impressions.
Phase 3, randomized (1:1), open-label, multicenter trial comparing osimertinib plus pemetrexed and platinum-based chemotherapy versus osimertinib monotherapy in previously untreated EGFR-mutant locally advanced or metastatic NSCLC.
Adults with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R mutations, as detected by an FDA-approved test, with no prior systemic therapy for advanced disease.
Tagrisso (osimertinib) 80 mg daily plus pemetrexed (500 mg/m2) and investigator-choice cisplatin or carboplatin every 3 weeks for 4 cycles, then osimertinib plus pemetrexed maintenance, versus Tagrisso monotherapy.
Primary: investigator-assessed progression-free survival (PFS). Key secondary: overall survival (OS).
Osimertinib plus chemo reduced risk of progression or death by 38%. Median PFS 25.5 months versus 16.7 months (HR 0.62; 95% CI: 0.49-0.79; p<0.0001).
Final OS: median OS 47.5 months versus 37.6 months (HR 0.77; 95% CI: 0.61-0.96; p=0.02). Longest OS in global phase 3 EGFR NSCLC. 3-year OS: 63% vs 51%.
Grade 3+ AEs in 70% versus 34%, driven by chemo-related myelosuppression. Leukopenia 88%, thrombocytopenia 85%, neutropenia 85%. Tagrisso discontinuation rates low: 12% vs 7%.
FDA approved February 16, 2024. NCCN Category 1 for 1L EGFR NSCLC. 65-70% of patients now receive this over monotherapy. Finite 4-cycle chemo followed by oral maintenance is logistically preferred by patients over perpetual IV infusions.
FLAURA2 is a Phase 3 randomized trial (NCT04035486) comparing osimertinib (Tagrisso) plus platinum-based (pemetrexed) chemotherapy with osimertinib alone as first-line treatment for EGFR-mutated (exon 19 deletion or L858R) advanced non-small cell lung cancer. Progression-free survival was the primary endpoint.
Adding platinum-pemetrexed chemotherapy to osimertinib reduced the risk of progression or death by 38%: median PFS was 25.5 months versus 16.7 months (HR 0.62; p<0.0001). Final overall survival also favored the combination (median 47.5 vs 37.6 months, HR 0.77; p=0.02), with a 3-year OS of 63% versus 51%.
Yes. On February 16, 2024 the FDA approved osimertinib (Tagrisso) in combination with pemetrexed and platinum-based chemotherapy for the first-line treatment of locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R mutations, based on FLAURA2.
The efficacy gain comes with more toxicity: Grade 3 or higher adverse events occurred in 70% of combination patients versus 34% with osimertinib alone, driven by chemotherapy-related myelosuppression (leukopenia, neutropenia, thrombocytopenia). However, osimertinib discontinuation rates stayed low (12% vs 7%).
FLAURA2 supports osimertinib plus chemotherapy as a more intensive first-line option for EGFR-mutated advanced NSCLC, and NCCN lists it as a Category 1 option. Patient selection weighs the deeper, longer disease control against the added chemotherapy toxicity, so higher-risk patients who can tolerate chemotherapy are often prioritized; the choice is individualized between physician and patient.



















