Phase 3 trial of lorlatinib (Lorbrena) vs crizotinib as first-line therapy for advanced ALK-positive NSCLC. The 7-year update presented at ASCO 2026 (Abstract 8502) — among the longest Phase 3 follow-up datasets ever reported in 1L NSCLC — shows the median PFS still not reached, with KOLs calling it practice-defining for ALK+ disease.
CROWN: A Randomized, Global, Phase 3 Study
Primary endpoint
Lorlatinib 100 mg once daily
Key eligibility criteria
n=149
PFS by BICR
Stage IIIB/IV ALK+ NSCLC
Key secondary endpoint
No prior systemic treatment for
OS
Stratified by:
metastatic disease
Presence of brain metastases
Other secondary endpoints
ECOG PS 0-2
Randomized
(yes vs no)
PFS by investigator
Asymptomatic treated or untreated
1:1
Ethnicity
ORR by BICR and investigator
CNS metastases were permitted
N=296
(Asian vs non-Asian)
IC ORR, IC TTP. DOR, IC DOR,
TTR and IC TTR by BICR and
21 extracranial measurable target
Crizotinib 250 mg twice daily
investigator
lesion (RECIST 1.1) with no prior
radiation required
n=147
Safety
Quality of life
No crossover between treatment arms was permitted
Biomarker analyses
In this post hoc analysis with 7 years of follow-up, we present investigator-assessed efficacy outcomes,
safety, and biomarker analyses (data cutoff: October 31, 2025)
At data cutoff, the required number of OS events for a protocol-specified second interim analysis (at least
139 deaths) has not been reached; 123 of 296 (42%) discontinued the study in both arms due to death
ALK, anaplastic tymphoma knase; BICR binded independent central review, CNS, central nervous system DOR, duration of response ECOG Eastern Cooperative Oncology Group HR, hazard ratio; IC intracranial NSCLC non-small cell lung cancer, ORR,
objective response rate, OS, overall survival PFS. progression free survival PS performance status, RECIST Response Evaluation Critena in Sold Tumors TTP. time to tumor progression TTR, time to tumor response
*Defined as the time from randomization to RECIST defined progression or death due to any cause
2026 ASCO
#ASCO26
PRESENTED BY: Tony S. K. Mok. MD (tony@clo.cuhk.edu.hk)
ASCO
AMERICAN
CUNCAL ONCOLOGY
ANNUAL MEETING
Presentation property of the author and ASCO Permission required for - permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
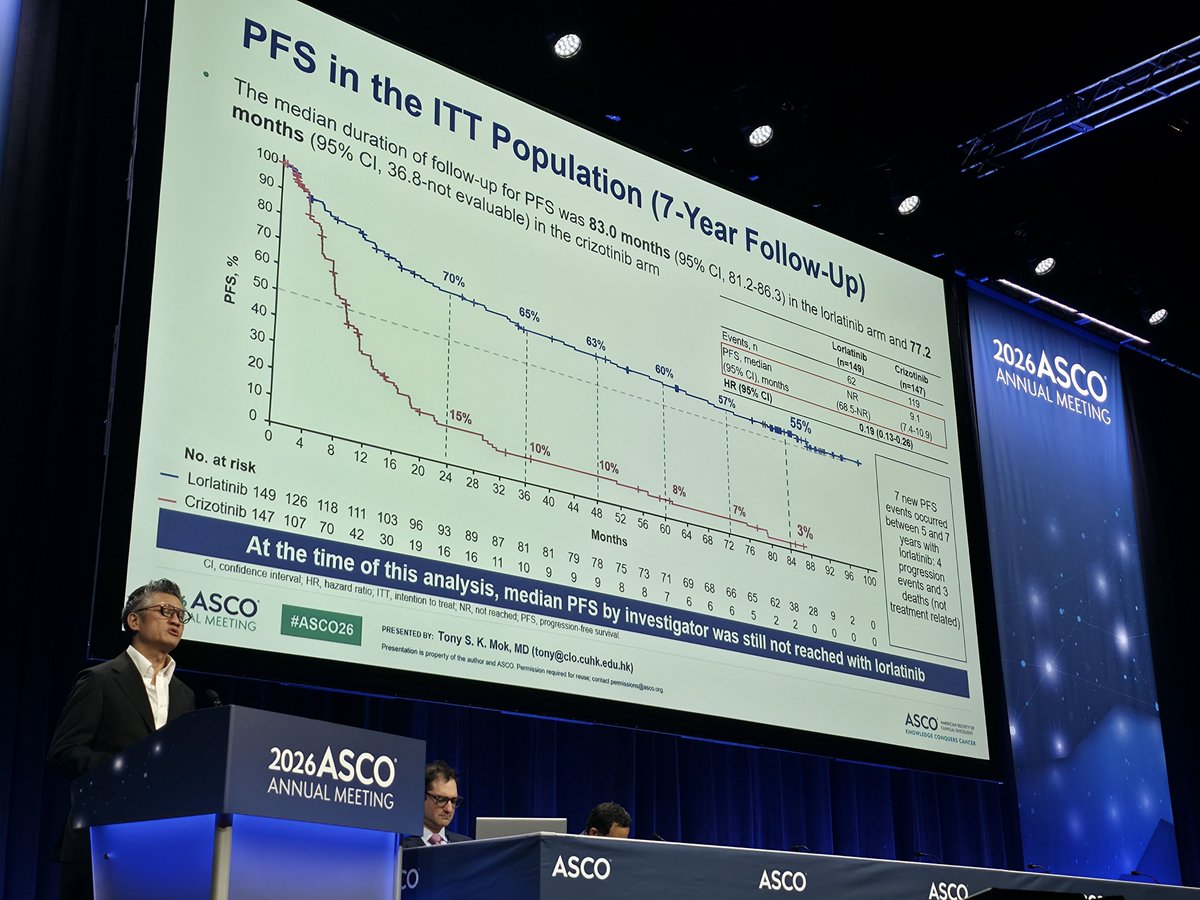
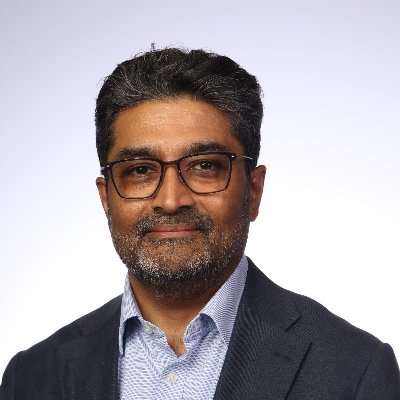
PFS in the ITT Population (7-Year Follow-Up)
The median duration of follow-up for PFS was 83.0 months (95% CI, 81.2-86.3) in the lorlatinib arm and 77.2
months (95% CI, 36.8-not evaluable) in the crizotinib arm
Lorlatinib
Crizotinib
100
(n=149)
(n=147)
90
Events, n
62
119
PFS, median
NR
9.1
80
70%
(95% CI), months
(68.5-NR)
(7.4-10.9)
70
65%
63%
HR (95% CI)
0.19 (0.13-0.26)
60%
60
57%
55%
PFS, %
50
40
7 new PFS
events occurred
30
between 5 and 7
20
15%
10%
10%
years with
8%
10
7%
3%
lorlatinib: 4
progression
0
events and 3
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80 84 88
92 96 100
deaths (not
Months
No. at risk
treatment related)
Lorlatinib 149 126 118 111 103 96 93 89 87 81 81 79 78 75 73 71 69 68 66 65 62 38 28 9 2 0
Crizotinib 147 107 70 42 30 19 16 16 11 10 9 9 9 8 8 7 6 6 6 5 2 2 0 0 0 0
At the time of this analysis, median PFS by investigator was still not reached with lorlatinib
CI, confidence interval HR, hazard ratio, ITT, intention to treat, NR not reached PFS, progression free survival
2026 ASCO
#ASCO26
PRESENTED BY: Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation - property of the author and ASCO Permission required for - conted
KNOWLEDGE CONQUERS CANCER
---
Time to IC Progression by Brain Metastases
With baseline brain metastases
Without baseline brain metastases
Lorlatinib
Crizotinib
Lorlatinib
Crizotinib
(n=35)
(n=38)
(n=114)
(n=109)
Events, n
5
26
Events, n
4
40
Time to IC progression,
NR
7.2
Time to IC progression,
NR
23.9
months, median (95% CI)
(NR-NR)
(3.7-11.0)
months, median (95% CI)
(NR-NR)
(16.4-30.8)
HR (95% CI)
0.03 (0.01-0.13)
HR (95% CI)
0.04 (0.02-0.12)
96%
96%
96%
96%
96%
96%
100
100
90%
90
83%
83%
83%
83%
83%
90
Patients without IC progression, %
80
80
70
Patients without IC progression, %
70
60
60
50
50
40
40
30
30
49%
33%
20
20
33%
29%
29%
10
10
22%
0
0
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80
84
88
92
96100
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80
84
88
92
96100
No. at risk
Months
No. at risk
Months
Loriatinib 35 32 29 28 28 26 26 25 22 22 20 20 20 20 20 20 18 18 18 18 17 11 7 3 1 0
—
Lortatinib
114
96
90
84
77
72
70
67
67
64
64
61
61
60
58
56
54
51
51
50
47
30
22
6
1
0
—
Crizotinib 109 86 63 41 31 21 19 18 12 10 10 10 9 8 8 7 6 6 6 5 2 2 0 0 0 0
Sustained plateau in time to IC progression indicates a prolonged protective effect against the
development of new brain metastases and a sustained control of the existing ones
CI, confidence interval HR, hazard ratio, IC intracranial; NR, not reached
2026 ASCO
#ASCO26
PRESENTED BY: Tony S.K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation - property of the author and ASCO Permission required for - contact
KNOWLEDGE CONQUERS CANCER
---
Conclusions
After 7 years of follow-up in the phase 3 CROWN study, with lorlatinib treatment:
PFS exceeds 7 years with 7-year PFS of 55%
2026ASCO
ANNUAL MEETING
Patients without progression within 24 months on lorlatinib had a 79% probability of being alive and
free of progression at 7 years
PFS benefit was consistent across all prespecified subgroups
7-year IC time to progression was 92%, with a sustained plateau from 30 months onward, indicating
long-term CNS protection
OS follow-up is ongoing and results will be presented in the future
No new safety signals were identified, and all treatment-related discontinuations occurred within the
first 26 months
ctDNA analysis showed no emerging new ALK resistance mutations
Early progressors had a higher number of alterations and a higher tumor mutation burden compared
with long-term responders
ALK inaplistic tymphoms knase CNS contral norvous system, clDNA, circulating turnor DNA K. intracranial os, overall survival PFS, progression free survival
2026 ASCO
#ASCO26
PRESENTED BY: Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
AMERICAN
CUNICAL CHOCOLOGY
ANNUAL MEETING
Presentation - property of the author and ASCO Permission wgared for - contact
KNOWLEDGE CONQUERS CANCER
2026ASCO
PFS in the ITT Population (7-Year Follow-Up)
ANNUAL MEETING
The median duration of follow-up for PFS was 83.0 months (95% CI, 81.2-86.3) in the lorlatinib arm and 77.2
months (95% CI, 36.8-not evaluable) in the crizotinib arm
Lorlatinib
Crizotinib
100
(n=149)
(n=147)
90
Events, n
62
119
PFS. median
NR
9.1
80
70%
(95% CI), months
(68.5-NR)
(7.4-10.9)
70
65%
63%
HR (95% CI)
0.19 (0.13-0.26)
60%
60
57%
55%
PF PFS, %
50
40
7 new PFS
events occurred
30
between 5 and 7
20
15%
10%
10%
years with
8%
10
7%
3%
lorlatinib: 4
progression
0
events and 3
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80
84
88
92
96
100
deaths (not
Months
No. at risk
treatment related)
-
Lorlatinib 149 126 118 111 103 96 93 89 87 81 81 79 78 75 73 71 69 68 66 65 62 38 28 9 2
0
-
Crizotinib 147 107 70 42 30 19 16 16 11 10 9 9 9 8 8 7 6 6 6 5 2 2 0 0 0 0
At the time of this analysis, median PFS by investigator was still not reached with lorlatinib
C, confidence intervet HR haved rate, ITE, visition to treat, NR, not eached, PFS, progression the survival
2026 ASCO
ASCO26
PRESENTED RY: Tony $. K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
ANNUAL MEETING
I
I
-
-
seried
KNOWLEDGE CONQUERS CANCER
LOSS
SSO
ASCO
A
SCO
ASCO
---
ASCO
Estimated Proportion of PFS Events With Lorlatinib
MEETING
Conditional PFS beyond 2 years
PFS
Measure
estimate
Estimated proportion of PFS events
100
PFS at years
70%
PFS at years
55%
90
*Conditional
80
79%
70%
PFS (7Y/2Y)
20%
70
"Estimated as the ratio of the
10%
55%
Kaplan-Meler PFS estimates at 7
60
5%
and 2 years: (55%/70%)
2%
PF PFS, %
3%
50
3%
2%
40
30
20
10
0
Year 1
Year 2
Year 3
Year 4
Year 5
Year 6
Year 7
No. at risk
- Lorlatinib 149 126 118 111 103 96 93 89 87 81 81 79 78 75 73 71 69 68 66 65 62 38 28 9 2 0
Patients without a PFS event in the first 24 months on lorlatinib have a
79%* probability of remaining alive and progression-free at 7 years
PFS, progression free survival
2026 ASCO
PRESENTED BY: Tony S.K. Mok, MD (tony@clo.cuhk.edu.hk)
#ASCO26
ASCO
ANNUAL MEETING
I
property
author
ASCO
Permission
I
-
I
contact
KNOWLEDGE CONQUERS CANCER
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
2026A
ANNUAL N
2026ASCO
ANNUAL MEETING
1
ASCO
ASCO
ASO
ASCO
ASCO
ASCO
---
PFS in the ITT Population (7-Year Follow-Up)
The median duration of follow-up for PFS was 83.0 months (95% CI, 81.2-86.3) in the lorlatinib arm and 77.2
months (95% CI, 36.8-not evaluable) in the crizotinib arm
Loriatinib
Crizotinib
100
(n=149)
(n=147)
90
Events, n
62
119
PFS. median
NR
9.1
80
70%
(95% CI), months
(68.5-NR)
(7.4-10.9)
70
65%
63%
HR (95% CI)
0.19 (0.13-0.26)
60%
60
57%
55%
PFS, -
50
40
7 new PFS
events occurred
30
between 5 and 7
20
15%
10%
10%
years with
10
%
7%
3%
forlatinib: 4
progression
0
events and 3
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80 84 88
92 96 100
deaths (not
Months
No. at risk
treatment related)
- Lorlatinib 149 126 118 111 103 96 93 89 87 81 81 79 78 75 73 71 69 68 66 65 62 38 28 9 2 0
Crizotinib 147 107 70 42 30 19 16 16 11 10 9 9 9 8 8 7 6 6 6 5 2 2 0 0 0 0
At the time of this analysis, median PFS by investigator was still not reached with lorlatinib
a confidence information HI, have nation nimber for frood, NNL - marched RS progression Income survival
2026 ASCO
#ASCO26
-
Tony 5. K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
WREN
I
ANNUAL MEETING
Presentation - Permission - - - -
Commission CANCER
---
Estimated Proportion of PFS Events With Lorlatinib
Conditional PFS beyond 2 years
PFS
Measure
estimate
Estimated proportion of PFS events
100
PFS at 2 years
70%
PFS at 7 years
55%
90
*Conditional
80
79%
70%
PFS (7Y/2Y)
20%
70
"Estimated as the ratio of the
10%
55%
Kaplan-Meier PFS estimates at 7
60
5%
and 2 years: (55% / 70%)
2%
PFS, %
3%
50
3%
2%
40
30
20
10
0
Year 1
Year 2
Year 3
Year 4
Year 5
Year 6
Year 7
No. at risk
Lorlatinib 149 126 118 111 103 96 93 89 87 81 81 79 78 75 73 71 69 68 66 65 62 38 28 9 2 0
Patients without a PFS event in the first 24 months on lorlatinib have a
79%* probability of remaining alive and progression-free at 7 years
PFS, progression-free survival
2026 ASCO
#ASCO26
PRESENTED BY: Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
AMERICAN SOCIETY OF
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
PFS in the ITT Population (7-Year Follow-Up)
The median duration of follow-up for PFS was 83.0 months (95% CI, 81.2-86.3) in the lorlatinib arm and 77.2
months (95% CI, 36.8-not evaluable) in the crizotinib arm
Lorlatinib
Crizotinib
100
(n=149)
(n=147)
90
Events, n
62
119
PFS, median
NR
9.1
80
70%
(95% CI), months
(68.5-NR)
(7.4-10.9)
70
65%
63%
HR (95% CI)
0.19 (0.13-0.26)
60%
60
57%
55%
PFS, %
50
40
7 new PFS
events occurred
30
between 5 and 7
20
15%
years with
10%
10%
8%
10
7%
3%
lorlatinib: 4
progression
0
events and 3
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80
84
88
92
96
100
deaths (not
Months
treatment related)
No. at risk
Lorlatinib 149 126 118 111 103 96 93 89 87 81 81 79 78 75 73 71 69 68 66 65 62 38 28 9 2 0
Crizotinib 147 107 70 42 30 19 16 16 11 10 9 9 9 8 8 7 6 6 6 5 2 2 0 0 0 0
At the time of this analysis, median PFS by investigator was still not reached with lorlatinib
CI, confidence interval; HR, hazard ratio; ITT, intention to treat; NR, not reached; PFS, progression-free survival.
2026 ASCO
PRE SENTED BY: Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
AMERICAN SOCIETY OF
CUNICAL ONCOLOGY
#ASCO26
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asoo.org
KNOWLEDGE CONQUERS CANCER
Background & Methods
CROWN (NCT03052608): A Randomized, Global, Phase 3 Study
Lorlatinib is a preferred standard-of-care first-line therapy for
Key eligibility criteria
Lorlatinib 100 mg once daily
Stage IIIB/IV ALK+ NSCLC
patients with advanced ALK-positive NSCLC
No prior systemic treatment for
Stratified by:
metastatic disease
Presence of brain metastases (yes vs no)
Randomized
Ethnicity (Asian vs non-Asian)
At 5 years of follow-up, median PFS by investigator was not
ECOG performance status 0-2
1:1
reached with lorlatinib vs 9.1 months with crizotinib
Asymptomatic treated or untreated CNS
Crizotinib 250 mg twice daily
metastases were permitted
>1 extracranial measurable target lesion
No crossover between treatment arms was permitted
(RECIST 1.1) with no prior radiation
We report long-term outcomes from the phase 3 CROWN
required
Primary endpoint: PFS by BICR
proor
Secondary endpoints: overall survival (key secondary endpoint),
study after 7 years of follow-up
PFS by investigator, objective response, IC objective response, IC
time to progression, DOR, IC DOR, safety, and biomarker analyses
Results
Median PFS was still not reached with lorlatinib and
Time to IC progression was still not reached with lorlatinib and 16.4 months with
In the lorlatinib arm, no emerging new ALK resistance mutations
9.1 months with crizotinib after ~7 years of follow-up
crizotinib; no new IC progression events occurred after the first 30 months
were detected in the ctDNA samples at end of treatment
HR (95% CI): 0.19 (0.13-0.26)
HR (95% CI): 0.06 (0.03-0.12)
100
100
94%
92%
92%
92%
92%
92%
90
90
The safety profile of lorlatinib was similar to that reported in the
80
80
primary analysis of the CROWN study and in subsequent follow-
70%
65%
up analyses
70
63%
70
60%
60
57%
55%
PFS,%
40
30
Patients without progression,
60
The most common any-grade all-causality AEs were
50
50
hypercholesterolemia (73%), hypertriglyceridemia (71%), and
edema (58%)
40
30
There was no increase in the frequency of patients with
37%
20
15%
20
25%
25%
maximum grade 3 or 4 AEs since the 5-year analysis (77%)
Lorlatinib
10%
10%
10
8%
Lorlatinib
22%
7%
3%
22%
Crizotinib
10
16%
Crizotinib
No new treatment-related AEs led to treatment
0
0
discontinuation after the first 26 months
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80
84
88
92
96
100
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80
84
88
92
96
Months
Months
AE, adverse event; ALK, anaplastic lymphoma kinase; BICR, blinded independent central review; CNS, central nervous system; ctDNA, circulating tumor DNA; DOR, duration of response; ECOG, Eastern Cooperative Oncology Group; IC, intracranial; NSCLC, non-small cell lung cancer; PFS, progression- free survival.
Results from this 7-year analysis show that lorlatinib as a single agent is able to persistently control the disease, over the entire duration of treatment and has
the potential to transform advanced ALK-positive NSCLC into a chronic disease for a substantial proportion of patients
Efficacy in Patients With and Without Dose Reduction
Within 26 Weeks
PFS
Time to IC progression
With dose reduction
Without dose reduction
With dose reduction
Without dose reduction
(n=23)
(n=98)
(n=24)
(n=99)
Events, n
6
36
Events, n
0
6
PFS,
Time to IC progression,
NR
NR
NR
NR
months, median
months, median (95% CI)
(NR-NR)
(NR-NR)
(79.8-NR)
(81.9-NR)
100
(95% CI)
100
90
90
80
80
70
PFS, %
Patients without IC
70
60
progression, %
60
50
50
40
40
30
30
20
20
10
10
0
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80 84 88 92 96 100
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80 84 88 92 96 100
No. at risk
Months
No. at risk
Months
With dose 23 21 20 18 17 15 15 15 14 13 12 12 12 12 11 11 10 10 9 7 5 3 0 0 0 0
—
With dose 24 21 20 18 17 15 15 15 14 13 13 13 13 13 11 11 11 11 10 8 5 3 0 0 0 0
reduction
reduction
--
Without 98 96 86 79 76 75 72 70 67 66 66 64 61 60 59 57 56 55 55 37 24 12 5 2 0 0
--
Without 99 96 88 82 79 78 75 73 70 68 68 67 66 64 63 58 58 57 57 39 25 12 5 2 0 0
dose
dose
reduction
reduction
Long-term efficacy with lorlatinib was similar between patients with and without dose reduction within
26 weeks. PFS and IC TTP were also consistent across lorlatinib dose levels (100, 75, or 50 mg)
CI, confidence interval; IC, intracranial; NR, not reached, PFS, progression-free survival
2026 ASCO
#ASCO26
PRESENTED BY: Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
Conclusions
After 7 years of follow-up in the phase 3 CROWN study, with lorlatinib treatment:
PFS exceeds 7 years with 7-year PFS of 55%
Patients without progression within 24 months on lorlatinib had a 79% probability of being alive and
free of progression at 7 years
PFS benefit was consistent across all prespecified subgroups
7-year IC time to progression was 92%, with a sustained plateau from 30 months onward, indicating
long-term CNS protection
OS follow-up is ongoing and results will be presented in the future
No new safety signals were identified, and all treatment-related discontinuations occurred within the
first 26 months
ctDNA analysis showed no emerging new ALK resistance mutations
Early progressors had a higher number of alterations and a higher tumor mutation burden compared
with long-term responders
ALK, anaplastic lymphoma kinase; CNS, central nervous system, ctDNA circulating tumor DNA IC, intracranial OS, overall survival PFS, progression-free survival
2026 ASCO
PRESENTED BY: Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
AMERICAN SOCIETY OF
#ASCO26
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
SCO
MEETING
Lorlatinib: Mechanism of Action
Lorlatinib is a highly potent third-generation ALK
Molecular structure of ofatinib
TKI, specifically developed to penetrate the
Macrocycle compound)
blood-brain barrier and is retained in the CNS at
0
the therapeutic levels¹²
F.
N
it is known to have broad activity against most
known ALK resistance mutations¹²
N
in addition, orlatinib has shown in viro activity
N
0
against ROS1 and NTRK mutations
H2N
N
N
--
.
a ASCO
MASCOON
-
-
ASCO -
---
CROWN: A Randomized, Global, Phase 3 Study
Primary endpoint
Lorlatinib 100 mg once daily
Key eligibility criteria
n=149
PFS by BICR
Key secondary endpoint
Stage IIIB/IV ALK+ NSCLC
OS
No prior systemic treatment for
Stratified by:
Presence of brain metastases
Other secondary endpoints
metastatic disease
ECOG PS 0-2
(yes vs no)
PFS by investigator
Randomized
Ethnicity
ORR by BICR and investigator
Asymptomatic treated or untreated
1:1
(Asian vs non-Asian)
№296
IC ORR, IC TTP, DOR, IC DOR,
CNS metastases were permitted
TTR and IC TTR by BICR and
21 extracranial measurable target
Crizotinib 250 mg twice daily
investigator
lesion (RECIST 1.1) with no prior
n=147
Safety
radiation required
Quality of life
No crossover between treatment arms was permitted
Biomarker analyses
In this post hoc analysis with 7 years of follow-up, we present investigator-assessed efficacy outcomes,
safety, and biomarker analyses (data cutoff: October 31, 2025)
At data cutoff, the required number of OS events for a protocol-specified second interim analysis (at least
139 deaths) has not been reached; 123 of 296 (42%) discontinued the study in both arms due to death
ALK, anaplastic lymphoma knase, BICR, blinded independent central review, CNS central nervous system DOR duration of response, ECOG. Eastem Cooperative Oncology Group HR, hazard ratio, IC, intracranal, NSCLC, non- small cell lung cancer, ORR,
objective response rate, OS, overall survival, PFS, progression-tree survival, PS. performance status; RECIST, Response Evaluation Criteria in Solid Tumors TIP, time to the progression; TTR, time in under response.
Defined as the time from randomization to RECIST defined progression or death due to any cause.
2026 ASCO
PRE SENTED IT: Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
-
CANCA
#ASCO26
ANNUAL MEETING
Presentation . property of the author and ASCO Permission required for - contact permissions@aste.com
ENQUILED CONQUERS CANCER
2026ASCO
ANNUAL MEETING
SCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
CO
ASCO
---
PFS in the ITT Population (7-Year Follow-Up)
The median duration of follow-up for PFS was 83.0 months (95% CI, 81.2-86.3) in the lorlatinib arm and 77.2
months (95% CI, 36.8-not evaluable) in the crizotinib arm
Lorlatinib
Crizotinlb
100
(n=149)
(n=147)
90
Events, n
62
119
PFS, median
NR
9.1
80
70%
(95% CI), months
(68.5-NR)
(7.4-10.9)
70
65%
63%
HR (95% CI)
0.19 (0.13-0.26)
60%
60
57%
55%
PFS, %
50
40
7 new PFS
events occurred
30
between 5 and 7
20
15%
10%
10%
years with
8%
10
7%
3%
lorlatinib: 4
progression
0
events and 3
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80
84
88
92
96
100
deaths (not
Months
No. at risk
treatment related)
Lorlatinib
149
126
118
111
103
96
93
89
87
81
81
79
78
75
73
71
69
68
66
65
62
38
28
9
2
0
Crizotinib
147
107
70
42
30
19
16
16
11
10
9
9
9
8
8
7
6
6
6
5
2
2
0
0
0
0
At the time of this analysis, median PFS by investigator was still not reached with lorlatinib
Cl, confidence interval; HR, hazard ratio; U. intention to treat; NR, not reached; PFS, progression-free survival.
2026 ASCO
PRE SENTED BY: Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk).
#ASCO26
ASCO
AMERICAN SOCIETY OF
CLINICAL CHICOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse; contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
Adverse Events
AEs of special interest
Lorlatinib
Crizotinib
58%
Edema
43%
No increase in frequency of grade 3 or 4 AEs since
the 5-year analysis (77%)
71%
Hypertnglycoridomia®
6%
- Majority were due to an increase in lipid values
73%
Hypercholosterotemia®
4%
Despite higher rates of hyperlipidemia with
lorlatinib, no increase in cardiovascular AEs was
46%
Peripheral neuropathy
16%
observed compared with crizotinib
45%
Weight gain
13%
Frequency of CNS AEs was consistent with longer
30%
Cognitive offects
7%
follow-up; most were grade 1 or 2
Dose reductions were reported in 34% of patients
21%
Mood effects
7%
in the lorlatinib group; median time to dose
5%
Psychotic offects
1%
reduction was 25 weeks
Grade 1/2
All treatment-related discontinuations (5%)
6%
Speech offects
0%
Grade 1/2
Grade 3/4
Grade 3/4
occurred within the first 26 months
100
80
60
40
20
0
0
20
40
60
80
100
Incidence, %
Incidence, %
Safety profile of lorlatinib was consistent with prior
AE, adverse event; CNS, central nervous system.
analyses with no new safety signals with longer follow-up
Comprised 0 cluster of AEs that may represent similar clinical symptoms or syndromos.
2026 ASCO
PRE SENTED BY: Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk)
#ASCO26
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco org.
KNOWLEDGE CONQUERS CANCER
PFS in the ITT Population (7-Year Follow-Up)
The median duration of follow-up for PFS was 83.0 months (95% CI, 81.2-86.3) in the lorlatinib arm and 77.2
months (95% CI, 36.8-not evaluable) in the crizotinib arm
Lorlatinib
Crizotinib
100
(n=149)
(n=147)
2026ASCO
ANNUAL MEETING
90
Events, n
62
119
PFS, median
NR
9.1
80
70%
(95% CI), months
(68.5-NR)
(7.4-10.9)
70
65%
63%
HR (95% CI)
0.19 (0.13-0.26)
60%
60
57%
55%
PFS, %
50
40
7 new PFS
events occurred
30
between 5 and 7
20
15%
years with
10%
10%
8%
10
7%
3%
lorlatinib: 4
progression
0
events and 3
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80 84 88
92
96
100
deaths (not
Months
No. at risk
treatment related)
—
Lorlatinib
149
126
118
111
103
96
93
89
87
81
81
79
78
75
73
71
69
68
66
65
62
38
28
9
2
0
Crizotinib 147 107 70 42 30 19 16 16 11 10 9 9 9 8 8 7 6 6 6 5 2 2 0 0 0
0
At the time of this analysis, median PFS by investigator was still not reached with lorlatinib
CL confidence interval HR hazard ratio, 111. intention to treat, NR not reached PFS, progression free survival
2026 ASCO
#ASCO26
PRESENTED BY ST. Tony S.K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
-
CORREAL
ANNUAL MEETING
Presentation property the author and ASCO Permission required for - contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
Γ
2026 ASCO J
ANNUAL MEETING
---
Time to IC Progression in the ITT Population
Lorlatinib
Crizotinib
100
94%
92%
92%
92%
92%
92%
(n=149)
(n=147)
2026ASCO
90
ANNUAL MEETING
Events, n
9
66
Patients without IC progression, %
80
Time to IC
NR
16.4
70
progression,
(NR-NR)
(12.7-21.9)
60
months, median
50
(95% CI)
40
HR (95% CI)
0.06 (0.03-0.12)
30
37%
20
25%
25%
22%
10
22%
16%
Tumor assessments, including brain
0
MRI, have been performed every 8
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80
84
88
92
96
weeks up to 5 years and every 16
No. at risk
Months
weeks afterwards in all patients
-
Lorlatinib
149
128
119
112
105
98
96
92
89
86
84
81
81
78
78
76
72
69
69
68
64
41
29
9
2
—
Crizotinib 147 107 75 46 34 22 19 18 12 12 10 10 9 8 8 7 6 6 6 5 2 2 0 0 0
throughout the study
No new IC progression events occurred after the first 30 months on lorlatinib
CI, confidence interval HR, hazard ratio, IC intracranial ITT. intention to treat MRI, magnetic resonance maging NR, not reached
2026 ASCO
#ASCO26
PRE MNITORY Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
CURRENT ORCOLOGY
ANNUAL MEETING
Presentation . property of the author and ASCO Permission required for - contact permissione@asco.org
KNOWLEDGE CONQUERS CANCER
2026 ASC
ANNUAL MEET
CROWN: A Randomized, Global, Phase 3 Study
Primary endpoint
Lorlatinib 100 mg once daily
Key eligibility criteria
n=149
PFS by BICR
Stage IIIB/IV ALK+ NSCLC
Key secondary endpoint
No prior systemic treatment for
OS
Stratified by:
metastatic disease
Presence of brain metastases
Other secondary endpoints
ECOG PS 0-2
Randomized
(yes vs no)
PFS by investigator
Asymptomatic treated or untreated
1:1
Ethnicity
ORR by BICR and investigator
CNS metastases were permitted
N=296
(Asian vs non-Asian)
IC ORR, IC TTP, DOR, IC DOR,
TTR and IC TTR by BICR and
≥1 extracranial measurable target
Crizotinib 250 mg twice daily
investigator
lesion (RECIST 1.1) with no prior
radiation required
n=147
Safety
Quality of life
No crossover between treatment arms was permitted
Biomarker analyses
In this post hoc analysis with 7 years of follow-up, we present investigator-assessed efficacy outcomes,
safety, and biomarker analyses (data cutoff: October 31, 2025)
At data cutoff, the required number of OS events for a protocol-specified second interim analysis (at least
139 deaths) has not been reached; 123 of 296 (42%) discontinued the study in both arms due to death
ALK, anaplastic ymphoma kinase; BICR, blinded independent central review; CNS, central nervous system; DOR, duration of response; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; IC, intracranial; NSCLC, non-small cell lung cancer; ORR,
objective response rate; OS, overall survival; PFS, progression-free survival; PS, performance status; RECIST, Response Evaluation Criteria in Solid Tumors; TTP, time to tumor progression; TTR, time to tumor response.
*Defined as the time from randomization to RECIST-defined progression or death due to any cause.
2026 ASCO
#ASCO26
PRESENTED BY: Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk)
ANNUAL MEETING
ASCO
AMERICAN SOCIETY OF
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco.org.
CUNICAL ONCOLOGY
KNOWLEDGE CONQUERS CANCER
---
PFS in the ITT Population (7-Year Follow-Up)
The median duration of follow-up for PFS was 83.0 months (95% CI, 81.2-86.3) in the lorlatinib arm and 77.2
months (95% CI, 36.8-not evaluable) in the crizotinib arm
Lorlatinib
Crizotinib
100
(n=149)
(n=147)
90
Events, n
62
119
PFS, median
NR
9.1
80
70%
(95% CI), months
(68.5-NR)
(7.4-10.9)
70
65%
63%
HR (95% CI)
60%
0.19 (0.13-0.26)
60
57%
55%
PFS, %
50
40
7 new PFS
30
events occurred
between 5 and 7
20
15%
10%
10%
years with
8%
10
7%
3%
lorlatinib: 4
0
progression
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
events and 3
80
84
88
92
96
100
deaths (not
Months
No. at risk
treatment related)
- Lorlatinib 149 126 118 111 103 96 93 89 87 81 81 79 78 75 73 71 69 68 66 65 62 38 28 9 2 0
-
Crizotinib 147 107 70 42 30 19 16 16 11 10 9 9 9 8 8 7 6 6 6 5 2 2 0 0 0 0
At the time of this analysis, median PFS by investigator was still not reached with lorlatinib
CI, confidence interval; HR, hazard ratio; U. intention to treat; NR, not reached; PFS, progression-free survival
2026 ASCO
#ASCO26
PRESENTED BY: Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
AMERICAN SOCIETY OF
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse; contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
Estimated Proportion of PFS Events With Lorlatinib
Conditional PFS beyond 2 years
PFS
Measure
estimate
Estimated proportion of PFS events
PFS at 2 years
70%
100
PFS at 7 years
55%
90
*Conditional
79%
80
70%
PFS (7Y/2Y)
20%
70
*Estimated as the ratio of the
10%
55%
Kaplan-Meier PFS estimates at 7
60
and 2 years: (55% / 70%)
5%
2%
3%
PFS, %
3%
50
2%
40
30
20
10
0
Year 1
Year 2
Year 3
Year 4
Year 5
Year 6
Year 7
No. at risk
— Lorlatinib 149 126 118 111 103 96 93 89 87 81 81 79 78 75 73 71 69 68 66 65 62 38 28 9 2 0
Patients without a PFS event in the first 24 months on lorlatinib have a
79%* probability of remaining alive and progression-free at 7 years
PFS, progression-free survival.
2026 ASCO
PRE SENTED BY: Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk)
#ASCO26
ASCO
AMERICAN SOCIETY or
CUPICAL CHICOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org.
KNOWLEDGE CONQUERS CANCER
---
Time to IC Progression in the ITT Population
Lorlatinib
Crizotinib
100
94%
92%
92%
92%
92%
92%
(n=149)
(n=147)
90
Events, n
9
66
Patients without IC progression, %
80
Time to IC
NR
16.4
70
progression,
(NR-NR)
(12.7-21.9)
60
months, median
(95% CI)
50
HR (95% CI)
0.06 (0.03-0.12)
40
30
37%
20
25%
25%
22%
22%
10
16%
Tumor assessments, including brain
0
MRI, have been performed every 8
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80
84
88
92
96
weeks up to 5 years and every 16
No. at risk
Months
weeks afterwards in all patients
— Lorlatinib 149 128 119 112 105 98 96 92 89 86 84 81 81 78 78 76 72 69 69 68 64 41 29 9 2
—
Crizotinib 147 107 75 46 34 22 19 18 12 12 10 10 9 8 8 7 6 6 6 5 2 2 0 0 0
throughout the study
No new IC progression events occurred after the first 30 months on lorlatinib
CI, confidence interval; HR, hazard ratio; IC, intracranial; ITT, intention to treat; MRI, magnetic resonance imaging; NR, not reached
2026 ASCO
#ASCO26
PRESENTED BY: Tony S. K. Mok, MD (tony@clo.cuhk.edu.hk)
ASCO
AMERICAN SOCIETY OF
DUPICAL CHCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
Current Post Hoc Analyses at 5 Years
Endpoint evaluation by BICR stopped after the 3-year analysis
Lorlatinib 100 mg once daily
Current analyses
Key eligibility criteria
n=149
Data cutoff: October 31, 2023
Stage IIIB/IV ALK+ NSCLC
No prior systemic treatment for
Stratified by:
metastatic disease
Presence of brain metastases
Investigator Assessed
ECOG PS 0-2
Randomized
(yes VS no)
PFS'
Asymptomatic treated or untreated
1:1
Ethnicity
ORR and IC ORR
CNS metastases were permitted
N=296
(Asian vs non-Asian)
DOR and IC DOR
21 extracranial measurable target
lesion (RECIST 1.1) with no prior
Crizotinib 250 mg twice daily
IC TTP
radiation required
n=147
Safety
No crossover between treatment arms was permitted
Biomarker analyses
The median duration of follow-up for PFS was 60.2 months (95% CI, 57.4-61.6) in the lorlatinib arm
and 55.1 months (95% CI, 36.8-62.5) in the crizotinib arm
CNS, central nervous system; DOR, duration of response ECOG, Eastern Cooperative Oncology Group IC, intracranial, ORR, objective response rate NSCLC, non small cell kng cancer, PFS. progression that survival, PS performance -
RECIST, Response Evaluation Criteria in Solid Tumors, TTP, time to tumor progression.
Defined as the time from randomization to RECIST-defined progression or death due to any cause
2024 ASCO
#ASCO24
PRE SENTED BY: Benjamin J. Solomon (Ben.Solomon@petermac.org
ASCO
- seceive
GREA I
ANNUAL MEETING
Presentation is property of N author ed ASCO Permission required for - contact
KNOWLEDGE CONDUCES CANCER
---
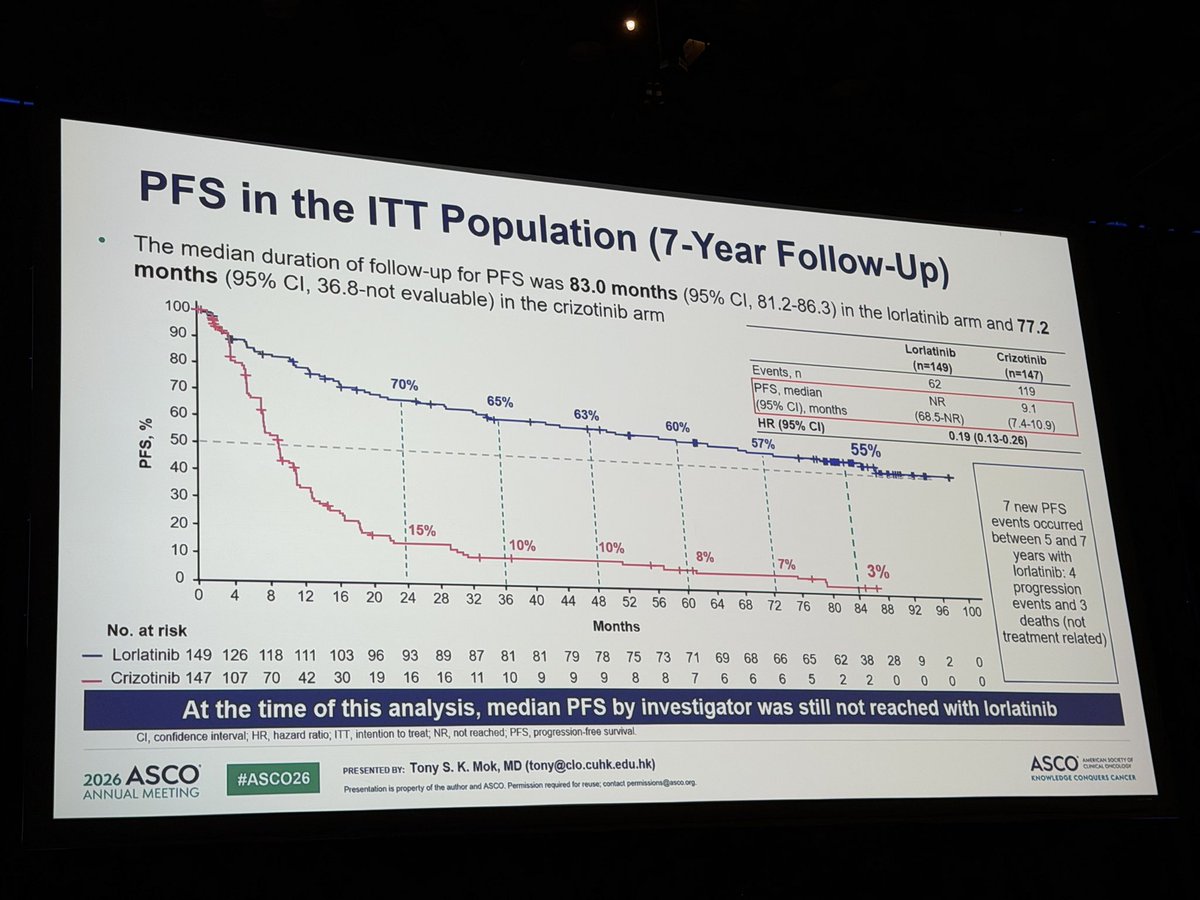
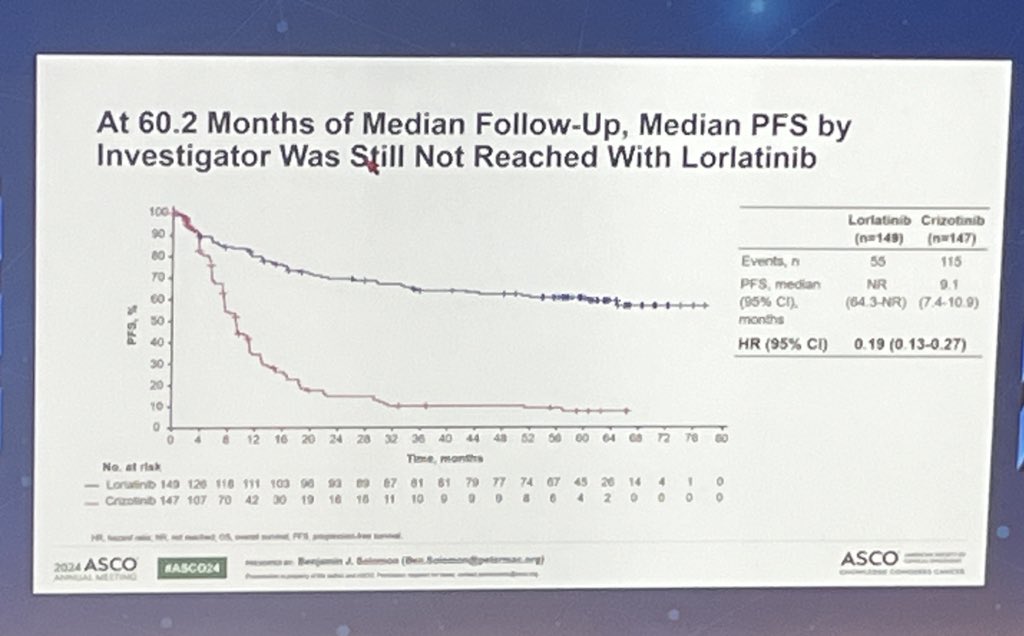
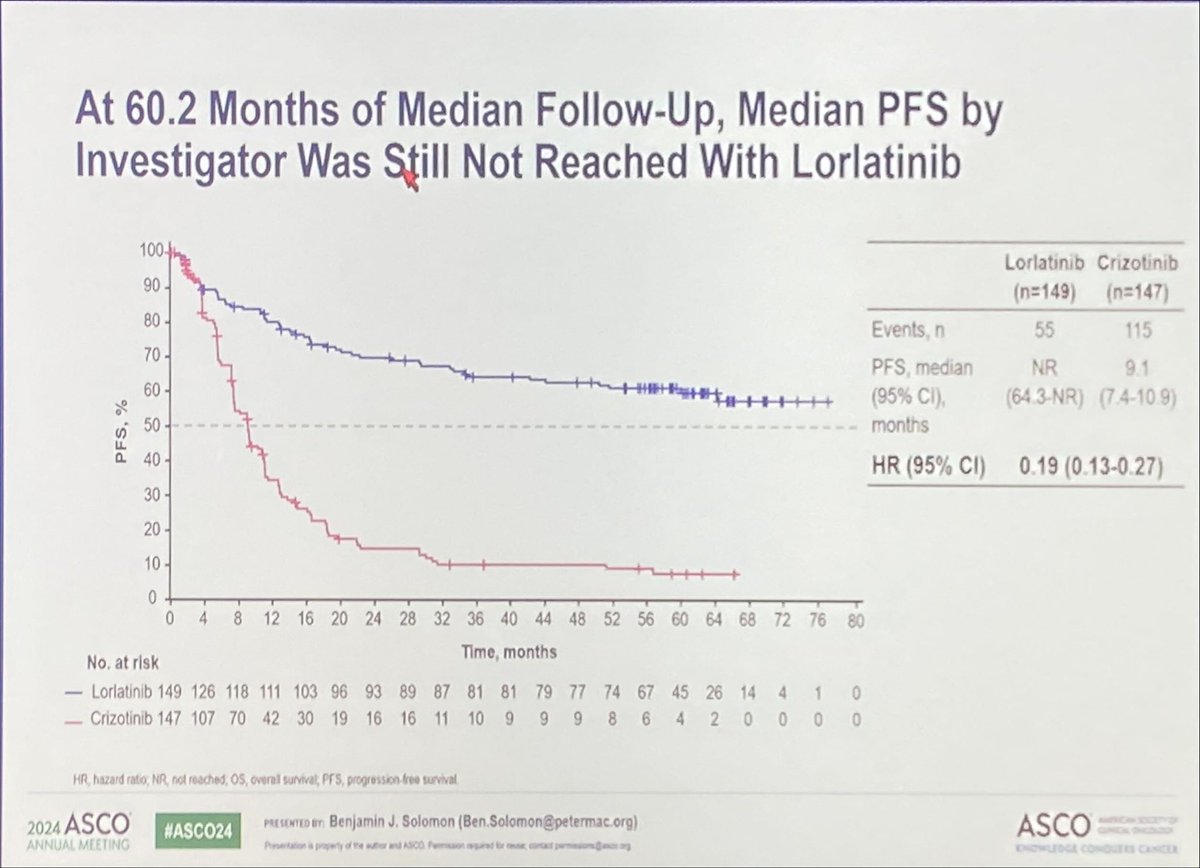
At 60.2 Months of Median Follow-Up, Median PFS by
Investigator Was Still Not Reached With Lorlatinib
100
Lorlatinib
Crizotinib
90
(n=149)
(n=147)
80
Events, n
55
115
70
PFS, median
NR
9.1
60
(95% CI),
(64.3-NR)
(7.4-10.9)
FS, %
50
months
40
HR (95% CI) 0.19 (0.13-0.27)
30
20
10
0
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80
No. at risk
Time, months
- Lorlatinib 149 126 118 111 103 96 93 89 87 81 81 79 77 74 67 45 26 14 4 1 0
- Crizotinib 147 107 70 42 30 19 16 16 11 10 9 9 9 8 6 4 2 0 0 0 0
HR, hazard ratio, NR, not reached, os, overall survival, PFS, progression-free survival
2024 ASCO
#ASCO24
PRESENTED IT Benjamin J. Solomon (Ben.Solomon@petermac.org)
ASCO
ONE INCOUDING
ANNUAL MEETING
Presentation is property of the author and ASICO Permission required for - contact permissions)
KNOWLEDGE CONDUERS CANCELL
CROWN (NCT03052608) is the pivotal Phase 3 trial that established lorlatinib (Lorbrena) as a first-line standard of care for advanced ALK-positive NSCLC. Lorlatinib is a third-generation CNS-penetrant ALK TKI engineered to overcome resistance mutations including the broad spectrum of secondary kinase-domain alterations that emerge on earlier-generation TKIs. At ASCO 2026 (Abstract 8502, published in Annals of Oncology), investigators presented the 7-year update — the longest randomized follow-up reported for a 1L NSCLC targeted therapy — with median PFS still not reached in the lorlatinib arm and a striking sustained CNS-protection signal, reinforcing lorlatinib as the practice-defining frontline option for ALK+ NSCLC.
Population
Treatment-naïve, advanced ALK-positive NSCLC (n=296), with or without baseline CNS metastases.
Intervention
Lorlatinib 100 mg orally once daily vs crizotinib 250 mg twice daily.
Primary Endpoint
Progression-free survival by blinded independent central review (RECIST 1.1).
Key Secondary
Overall survival (key secondary), investigator-assessed PFS, objective response (ORR), intracranial ORR, intracranial time to progression, duration of response (DOR), intracranial DOR, safety, and biomarker analyses.
At a median follow-up of 83.0 months for lorlatinib (vs 77.2 mo crizotinib) at the data cutoff (Oct 31, 2025), the median PFS remains NOT REACHED with lorlatinib vs 9.1 months (95% CI, 7.4–10.9) with crizotinib — HR 0.19 (95% CI, 0.13–0.27). The 7-year PFS rate is 55% with lorlatinib vs 3% with crizotinib (5-yr rates were 60% vs 8% per Solomon JCO 2024). Among patients event-free at 24 months on lorlatinib, the conditional probability of being progression-free at year 7 is 79%. 44% of lorlatinib patients remain on first-line treatment at the cutoff — the longest sustained PFS ever reported in advanced NSCLC.
Zero new intracranial progression events have occurred after 30 months on lorlatinib. Median time to intracranial progression is NOT REACHED with lorlatinib vs 16.4 months (95% CI, 12.7–21.9) with crizotinib — HR 0.06 (95% CI, 0.03–0.12). From prior 5-yr data: 5-year intracranial PFS rate was 92% with lorlatinib in patients without baseline brain metastases. KOLs (Akhade, Shah, Halmos) have called this the most striking CNS-protection signal of any targeted therapy in solid tumors.
Long-term lorlatinib tolerability is stable: treatment-related AE-driven discontinuation was only 5% on lorlatinib vs 6% on crizotinib, with no new permanent treatment-related discontinuations after 26 months. Dose reductions (34% on lorlatinib) did not compromise long-term efficacy. Class-defining lorlatinib AEs persist (hypercholesterolemia 72%, hypertriglyceridemia 66%, peripheral edema 57%, increased weight 44%, peripheral neuropathy 44%, cognitive effects 28%); these are actively managed with statin therapy, dose modification, and counseling.
STATUSFDA-approved 1L for ALK+ NSCLC since March 2021
Lorlatinib (Lorbrena) received FDA approval for the first-line treatment of advanced ALK-positive NSCLC in March 2021, based on the primary CROWN analysis. The subsequent 5-year (Solomon JCO 2024) and 7-year (ASCO 2026 Abstract 8502) updates reinforce its position as the standard-of-care 1L ALK TKI in major guidelines (NCCN, ESMO, ASCO).
CROWN is a Phase 3 randomized trial (NCT03052608) comparing lorlatinib (Lorbrena), a third-generation ALK inhibitor, with crizotinib as first-line therapy for advanced ALK-positive non-small cell lung cancer. Progression-free survival was the primary endpoint.
What did the CROWN 7-year update show?
At the ASCO 2026 seven-year update (Abstract 8502), 7-year progression-free survival was 55% with lorlatinib versus 3% with crizotinib (HR 0.19), and median PFS was still not reached with lorlatinib - one of the longest Phase 3 follow-up results ever reported in first-line NSCLC. About 44% of patients remained on lorlatinib at seven years.
How does lorlatinib affect brain metastases in CROWN?
Lorlatinib markedly delayed central nervous system progression: the median time to intracranial progression was not reached with lorlatinib versus 16.4 months with crizotinib (HR 0.06). This strong intracranial activity is a major reason KOLs describe the regimen as practice-defining for ALK-positive disease.
Is lorlatinib FDA approved for first-line ALK-positive NSCLC?
Yes. In March 2021 the FDA approved lorlatinib (Lorbrena) for the first-line treatment of ALK-positive metastatic NSCLC as detected by an FDA-approved test.
What is the safety and tolerability profile of lorlatinib in CROWN?
Treatment-related adverse event discontinuation was low and similar between arms (about 5% with lorlatinib vs 6% with crizotinib). Lorlatinib has a characteristic profile that includes metabolic effects (hyperlipidemia), edema, weight gain, and CNS/cognitive effects; these are generally managed with dose modification, and durable long-term treatment was common in CROWN.