Adjuvant HR+/HER2- early BC - Novartis
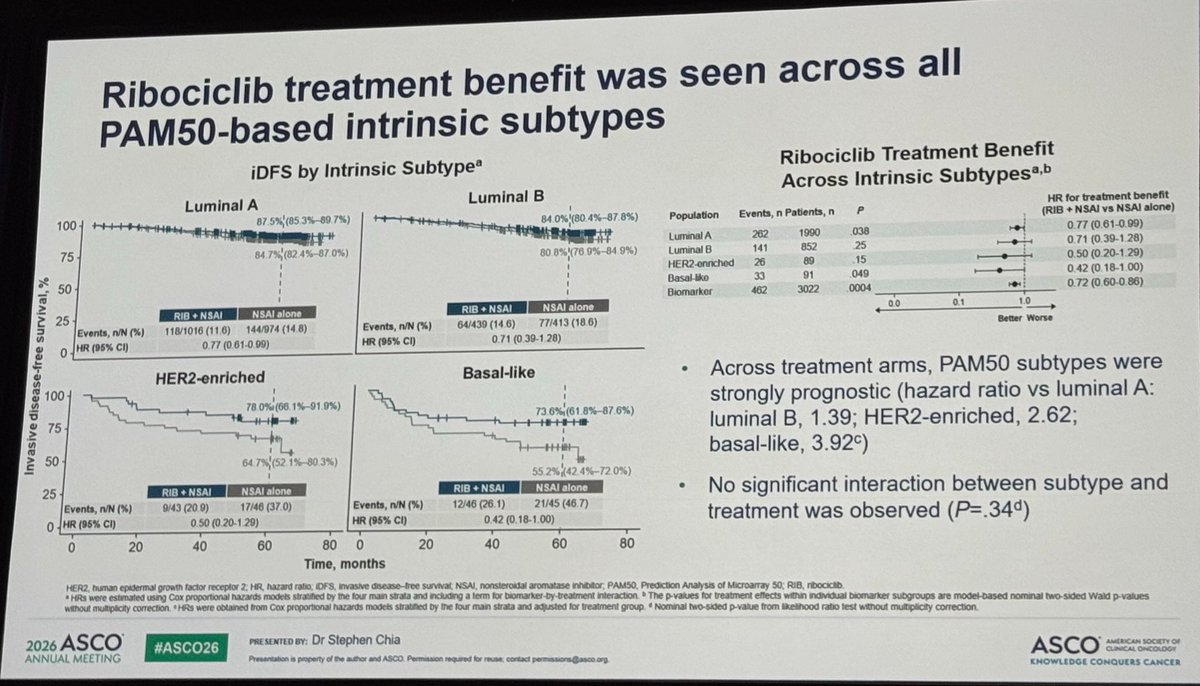
See ASCO 2026 Biomarker Analysis →Presented by Stephen K.L. Chia, MD (May 30, 2026 · Chicago) — PAM50 intrinsic subtype + gene-expression sub-analysis of 3,022 patients from the NATALEE adjuvant ribociclib + NSAI trial in HR+/HER2− early breast cancer.
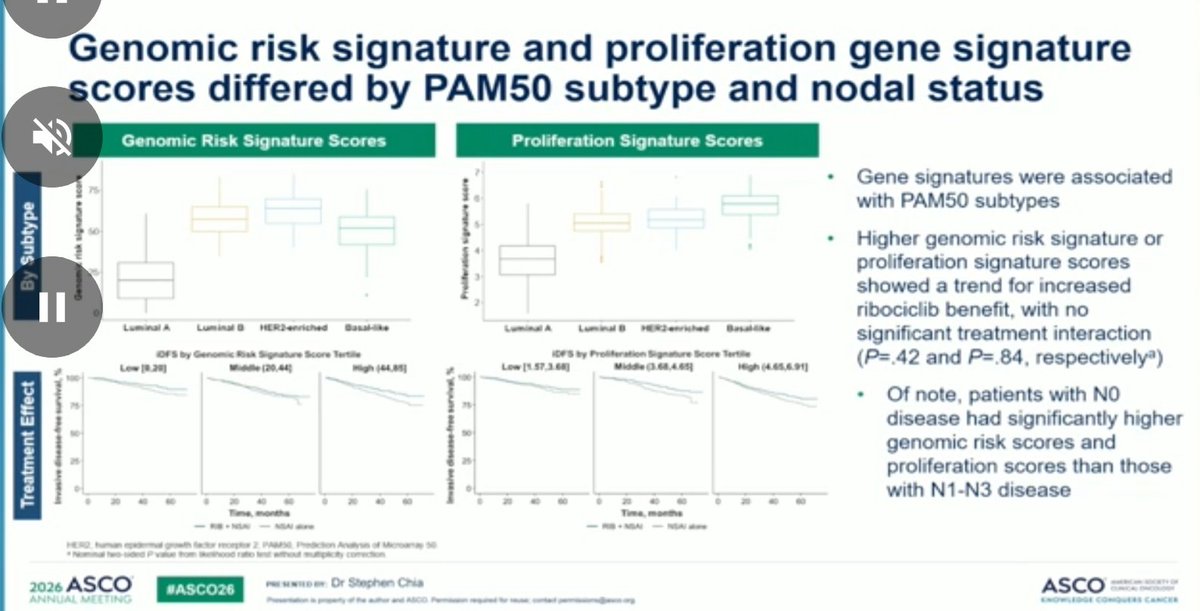
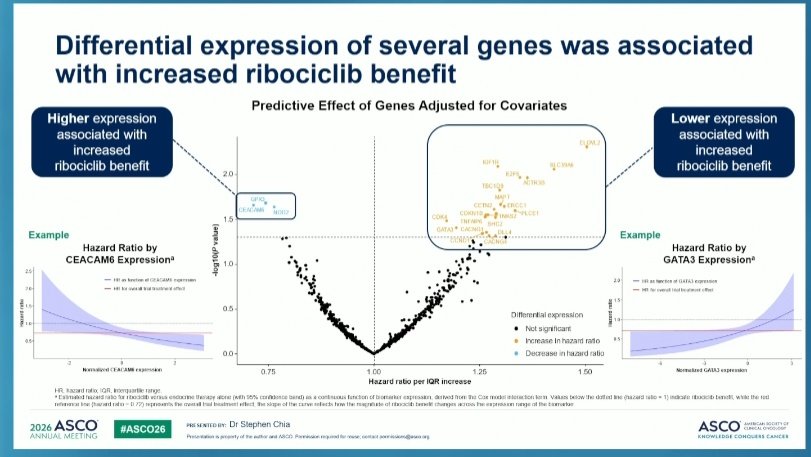
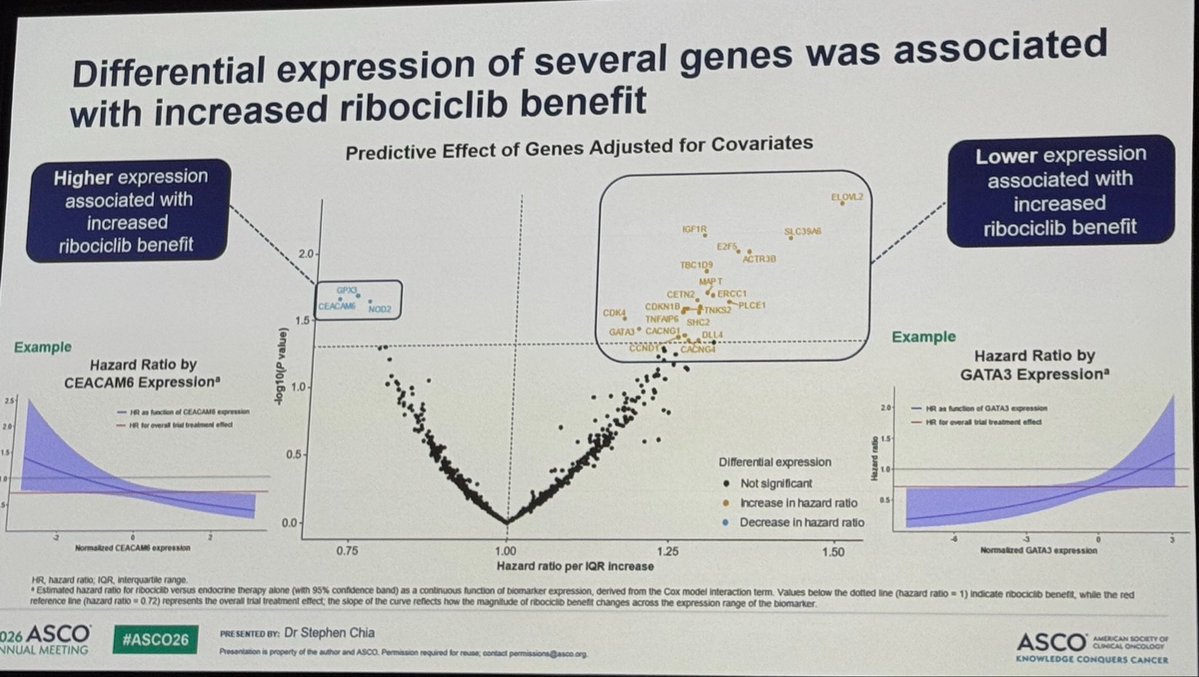
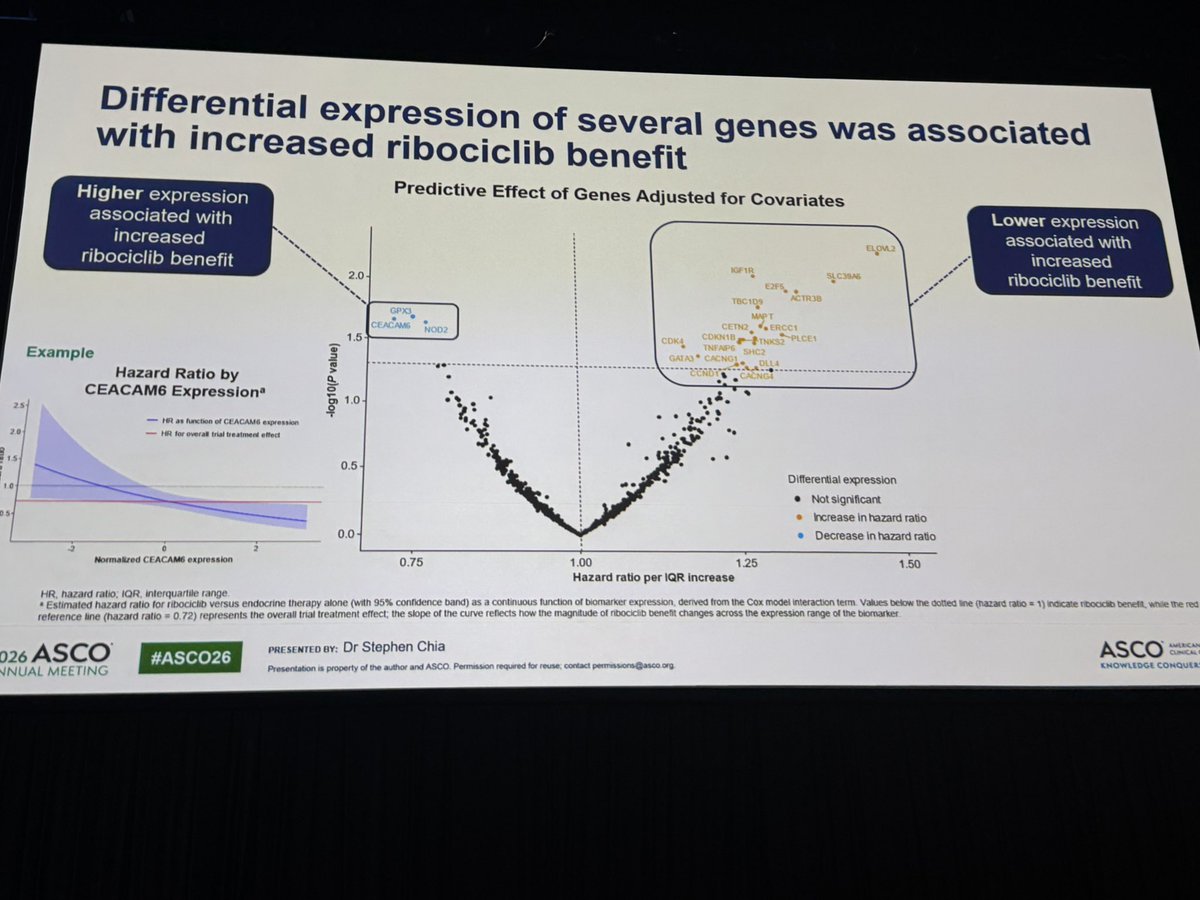
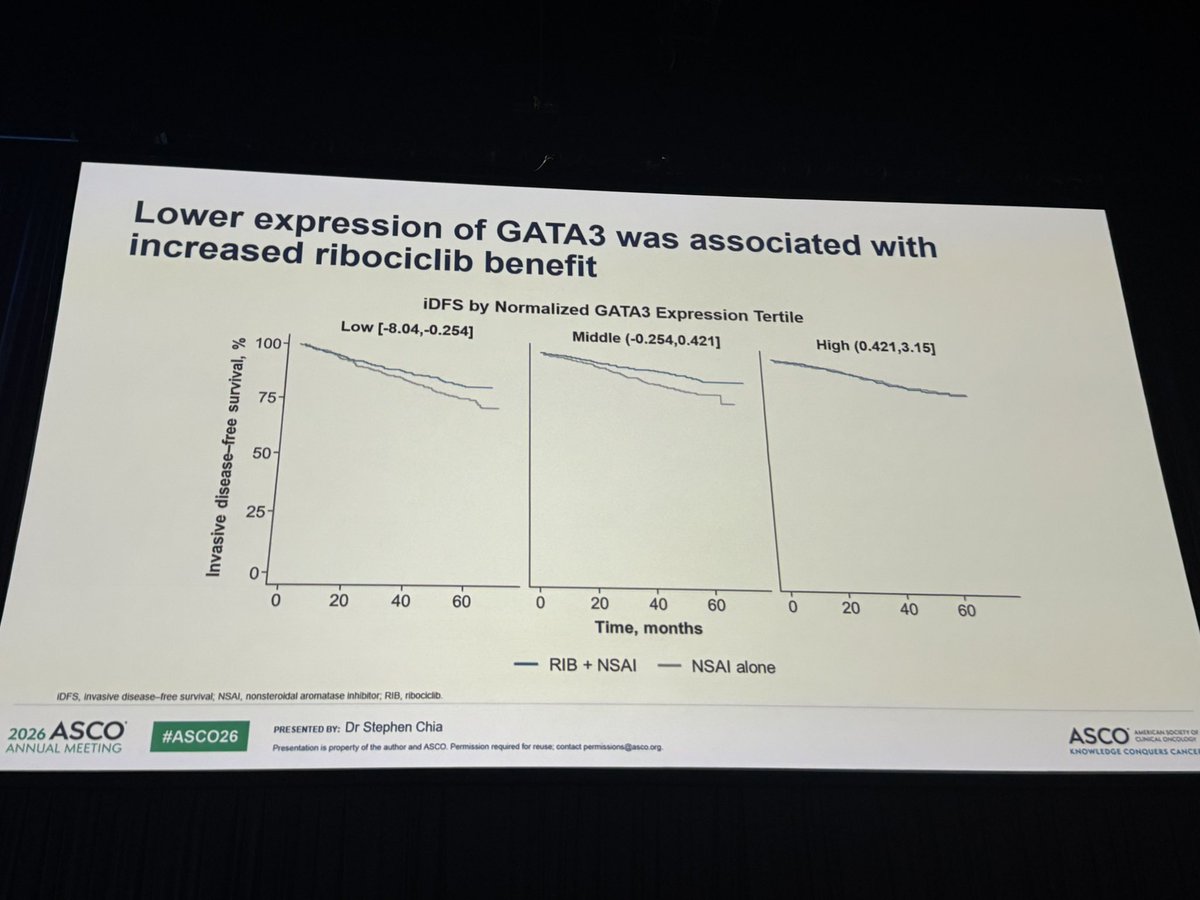
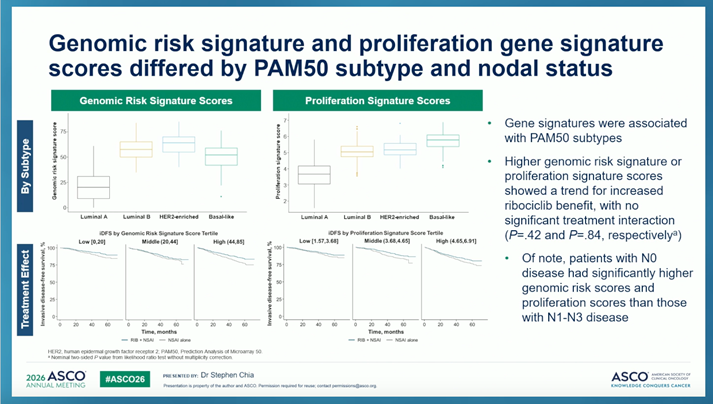
Gene-expression signal (exploratory): higher genomic risk and proliferation scores trended toward larger ribociclib benefit; higher CEACAM6 and lower GATA3 / CDK4 expression were associated with greater iDFS gain. None reached statistical significance for treatment interaction.
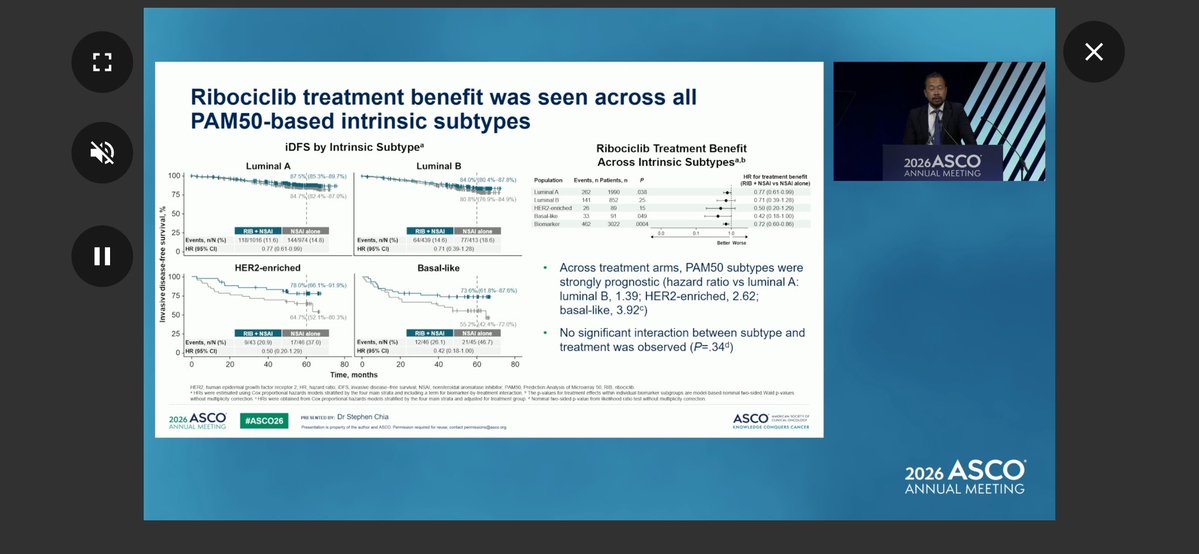
KOL takeaway — Paolo Tarantino, MD: "Interesting PAM50 sub-analysis from NATALEE, presented by Stephen Chia, showing a clear prognostic, but not predictive, role for PAM50 subtypes. Benefit from adjuvant ribociclib observed across subtypes and risk scores, with larger delta in HER2-E and basal-like tumors." [source →]
Live ASCO 2026 coverage → · Source: ASCO 2026 Abstract 501 (Chia et al., n=3,022 PAM50)
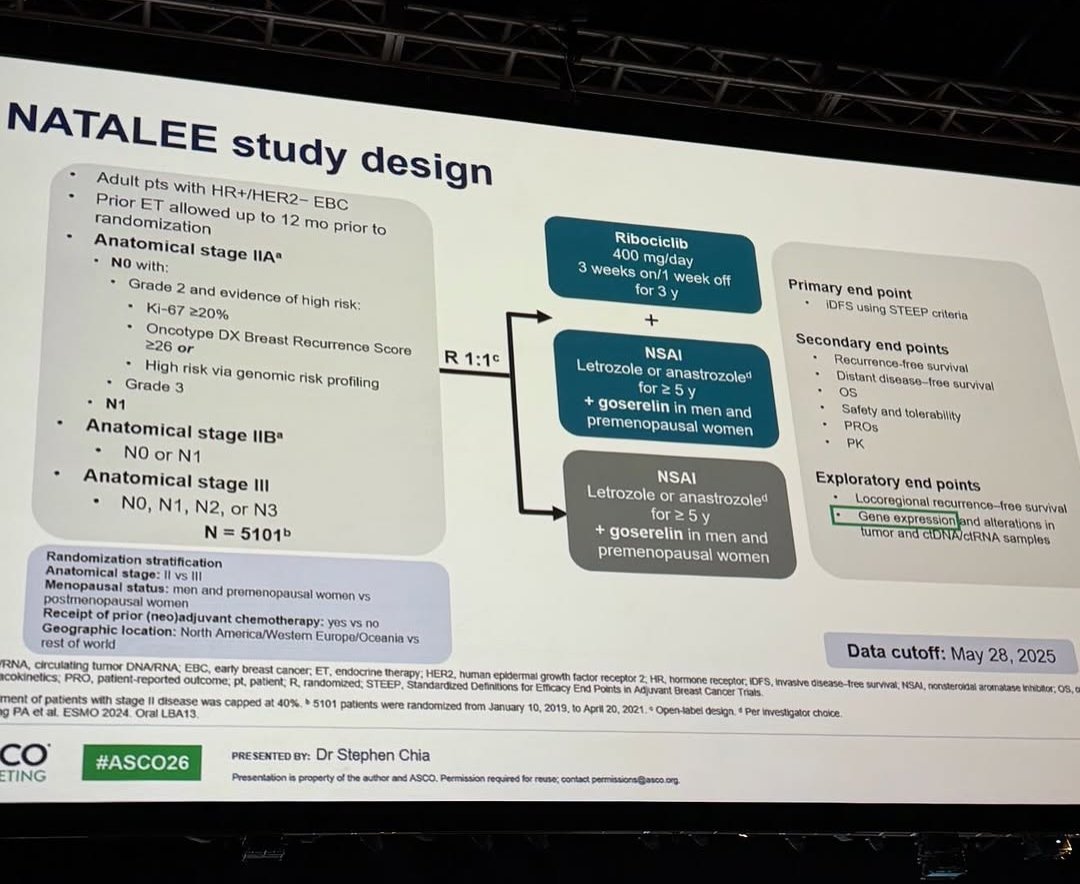
Design — Phase 3; adjuvant ribociclib (Kisqali) 400 mg + nonsteroidal AI vs AI alone, HR+/HER2- stage II-III early breast cancer, incl. node-negative (NCT03701334). (NEJM / Annals)
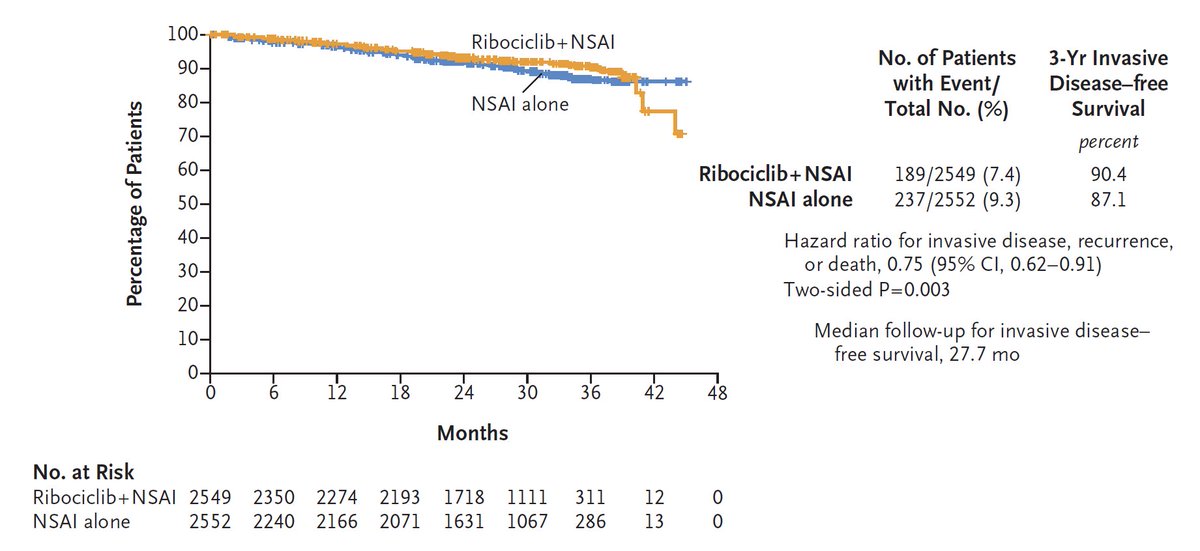
iDFS (primary) — HR ~0.749 (95% CI 0.628-0.892; p=0.0006); 3-year iDFS 90.7% vs 87.6%; benefit sustained at 4-5 year landmarks. (final iDFS analysis / ESMO Open)
OS — Immature; 5-year trend favors ribociclib (HR ~0.80, nominal). (page data)
Safety — Grade 3+ neutropenia 44.3% (febrile neutropenia 0.3%); hepatotoxicity monitored; 400 mg dose manageable. (page data)
Regulatory — FDA approved Sept 17, 2024 for adjuvant HR+/HER2- stage II-III EBC at high risk, with an AI. (FDA.gov)
Sponsor / Drug — Novartis; ribociclib (Kisqali), an oral CDK4/6 inhibitor, 400 mg 3-weeks-on/1-off for 36 months. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 20, 2026.






Top 12 by impressions (ASCO 2026 leads · deduped) - click to view on X

#ASCO26 🧬 Not all HR+/HER2- early breast cancers behave the same. New biomarker analysis from NATALEE suggests adjuvant ribociclib benefits were seen across ALL PAM50 subtypes, with a possible trend toward greater benefit in genomically higher-risk disease. 📌 3022 tumor https:/

💫🌟🚨 Top 10 #BreastCancer abstracts for #ASCO26 — selected by our leads and finalized via a Delphi voting process 🗳️🔬 1️⃣ 500 — OPTIMA 2️⃣ LBA1006 — PERSEVERA BC 3️⃣ 507 — KEYNOTE-522 final analysis 4️⃣ LBA1007 — SERENA-6 5️⃣ 502 — LIDERA BC 6️⃣ LBA1000 — ASCENT-04 7️⃣ 501 — NATA

NATALEE試験において、結局、アジュバントでのRibociclibはPAM50によるサブタイプに関わらず上乗せ効果あり。 誰にでも同じぐらい効いていたとも言えるけど、いまいちいいバイオマーカーが出てこないからやらなくていい集団がいまいち見つからないCDK4/6阻害薬… #ASCO26 https://t.co/SNsmeOcYl9

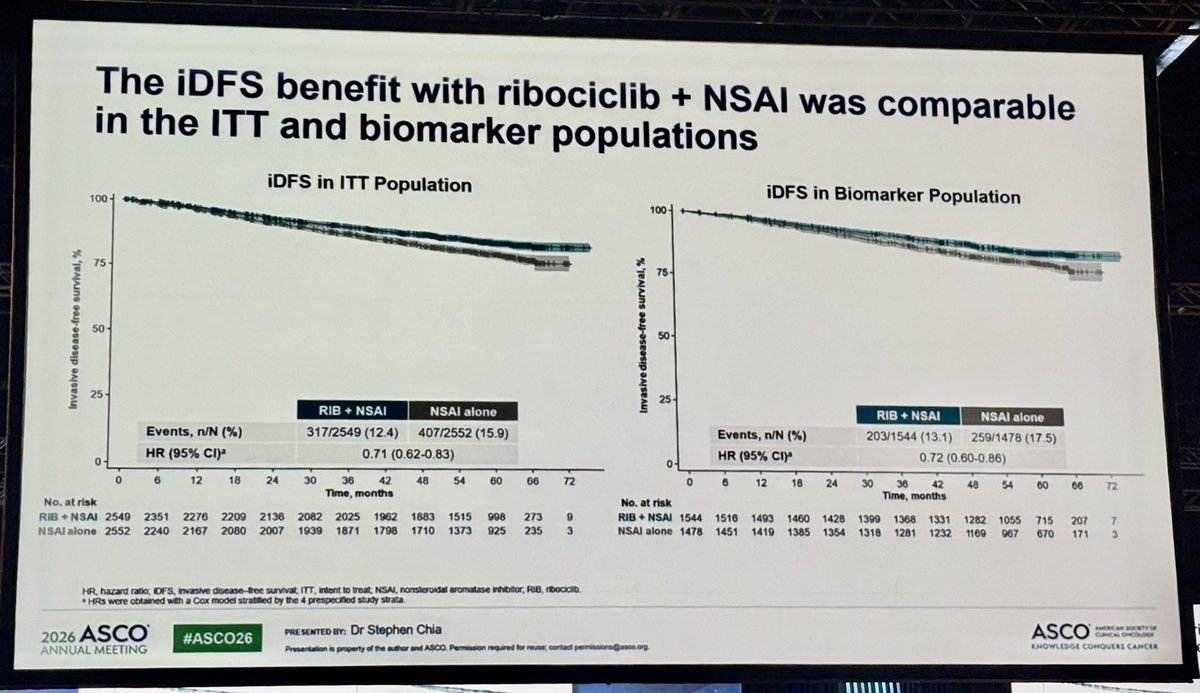
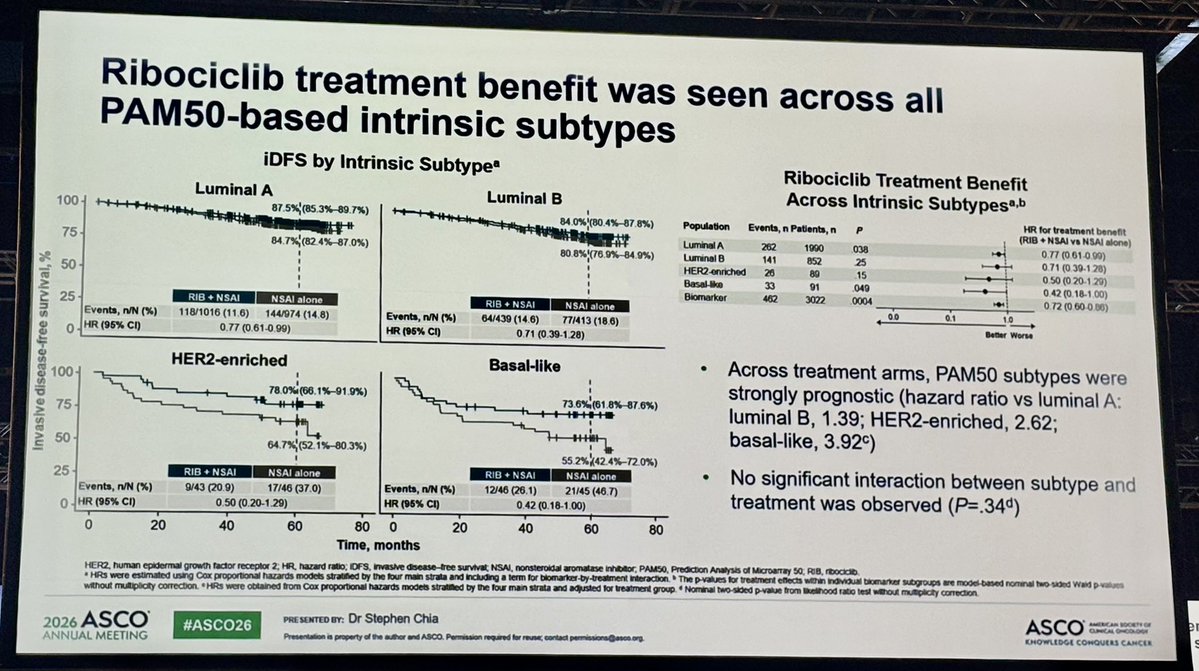
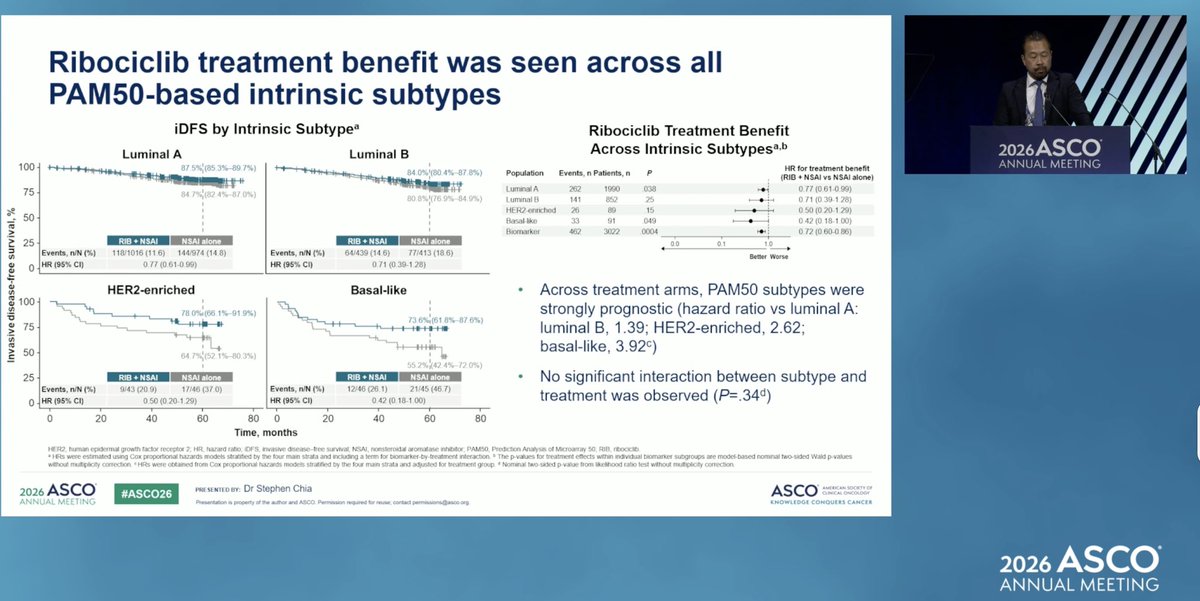
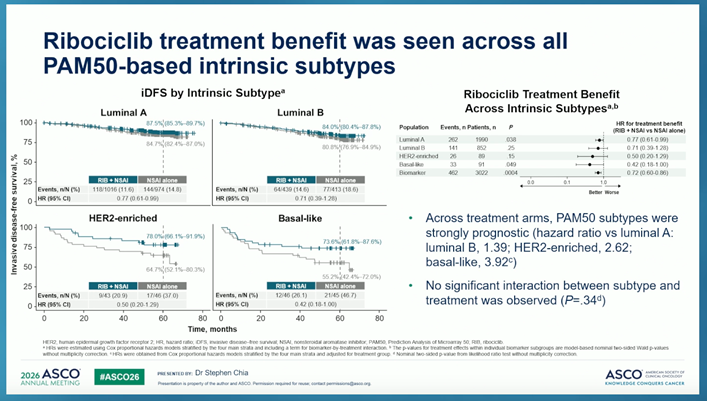
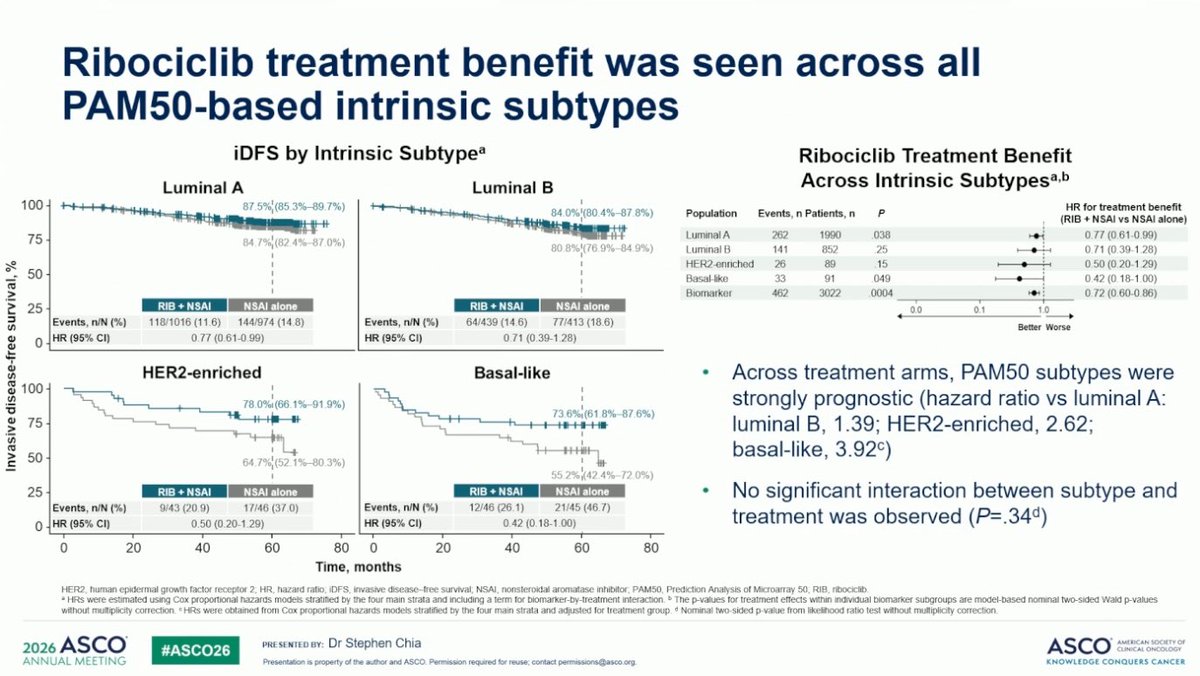
NATALEE Biomarker Analysis #ASCO26 Ribociclib + NSAI demonstrated consistent iDFS benefit across all PAM50 intrinsic subtypes in HR+/HER2− early breast cancer — regardless of luminal A, luminal B, HER2-enriched, or basal-like classification (interaction P=.34). iDFS HR: 0.71

Benefit of #ribociclib in #NATALEE: - persists across intrinsic subtypes - is greater in pts with higher risk tumors - may be variable based on certain gene expression ( ⬆️ benefit CEACAM6, ⬇️ CDK4, GATA3 etc) #ASCO26 #bcsm https://t.co/7BlAYcA46M

リボシクリプの術後内分泌療法への追加を見たNATALEE試験のバイオマーカー別サブ解析 内因性サブタイプがluminalより他のタイプの方が差が大きく見えたり、アグレッシブな遺伝子変化のほうが大きな利益は興味深い アベマシクリブも似た話になりそう #ASCO26 https://t.co/CJo6VbLIF6

NATALEE Trial: Consistent iDFS Benefit with Ribociclib Across All PAM50 Intrinsic Subtypes in HR+/HER2− Early #BreastCancer @OncoAlert @ASCO #ASCO26 #bcsm https://t.co/Xa11SvqEDs

Prognostic and predictive impact of baseline gene expression in the NATALEE trial of adjuvant ribociclib + nonsteroidal aromatase inhibitor in HR+/HER2− early #BreastCancer Stephen K.L. Chia #ASCO26 @OncoAlert #OncoAlert https://t.co/irIGGXNUGx

New biomarker insights from NATALEE trial presented by Stephen Chia, MD 📊 Baseline gene expression shows prognostic & predictive impact in HR+/HER2- early #breastcancer treated with adjuvant ribociclib + aromatase inhibitor #ASCO26 @ASCO https://t.co/iCG3ubX768

NATALEE gene-expression analysis presented #asco26 Ribociclib benefit seen across all PAM50 intrinsic subtypes Trend toward greater benefit for higher genomic risk or proliferation signatures Expression of several gene associated with increased ribociclib benefit @OncoAlert h
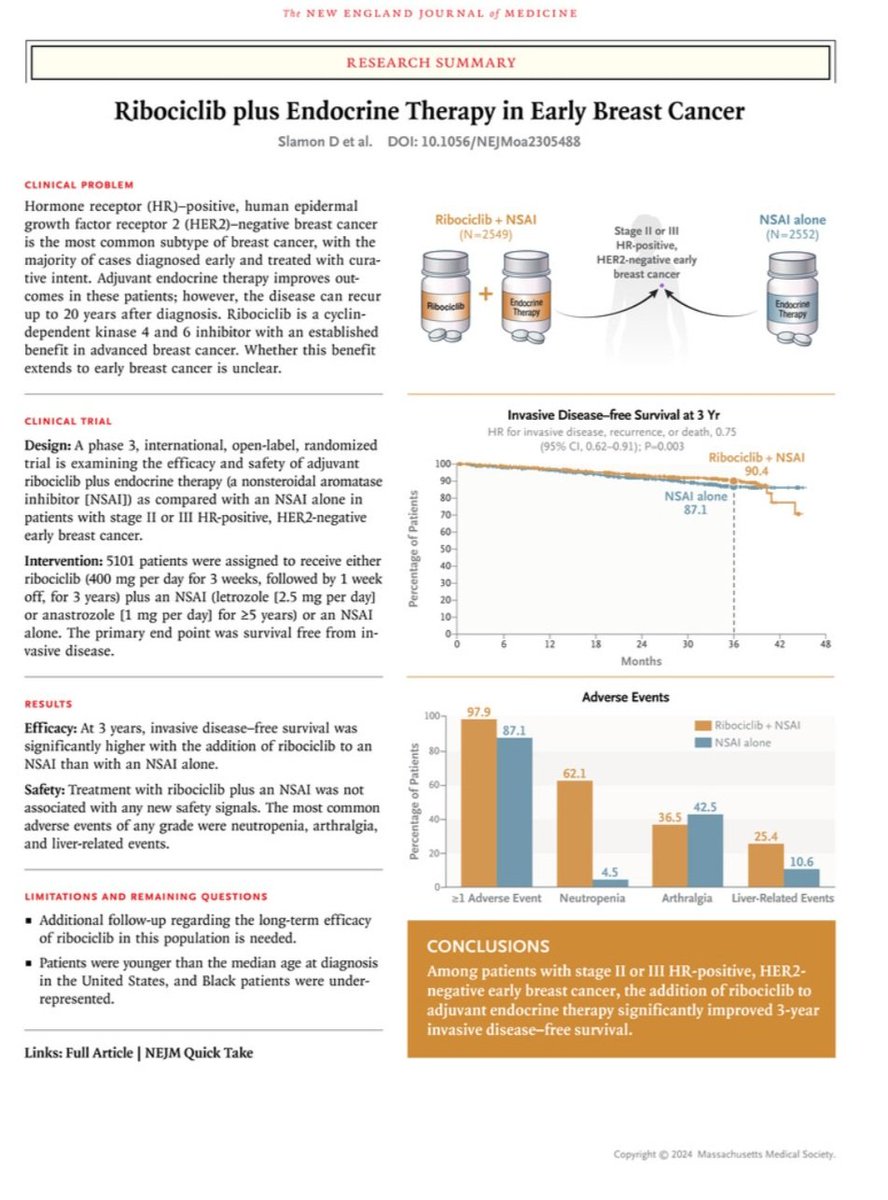
Ribociclib plus Endocrine Therapy in Early Breast Cancer : NATALEE 3y-iDFS: 90.4% vs 87.1% (HR:0.75) https://t.co/tdzIF8ctHs https://t.co/4QOTM26wu0
If you can fit a laser pointer between the curves, you can give the #ASCO24 plenary! https://t.co/TrmXCzrp3J
NATALEE is a global Phase III, multicenter, randomized, open-label trial that established adjuvant ribociclib (Kisqali) at 400 mg as the first CDK4/6 inhibitor approved for the broadest population of patients with HR+/HER2-negative stage II and III early breast cancer at high risk of recurrence. The trial randomized 5,101 patients across 20 countries to receive ribociclib plus a nonsteroidal aromatase inhibitor (letrozole or anastrozole) for 3 years with endocrine therapy for at least 5 years, or endocrine therapy alone. NATALEE uniquely included node-negative patients and used a lower 400 mg dose (versus the 600 mg metastatic dose) to optimize tolerability over the 3-year treatment duration.
Phase III, global, multicenter, randomized (1:1), open-label trial conducted at 393 centers across 20 countries in collaboration with TRIO. Stratified by menopausal status, AJCC 8th edition anatomic stage (II vs. III), prior neoadjuvant/adjuvant chemotherapy (yes vs. no), and geographic region.
Adults (men and pre- or postmenopausal women) with HR+/HER2-negative stage II or III early breast cancer at high risk of recurrence. Stage IIA T2N0 patients required grade 2 tumor with Ki-67 >=20% or high genomic risk (Oncotype DX Recurrence Score >=26, or high-risk by Prosigna/PAM50, MammaPrint, or EndoPredict), or grade 3 tumor. Node-positive disease of any stage II/III was eligible regardless of additional risk factors. Stage II comprised 40.3% and stage III comprised 59.4% of the study population.
Ribociclib 400 mg once daily (3 weeks on / 1 week off in 28-day cycles) for up to 36 months plus NSAI (letrozole or anastrozole) for at least 5 years, with goserelin for men and premenopausal women. Control arm received NSAI alone for at least 5 years.
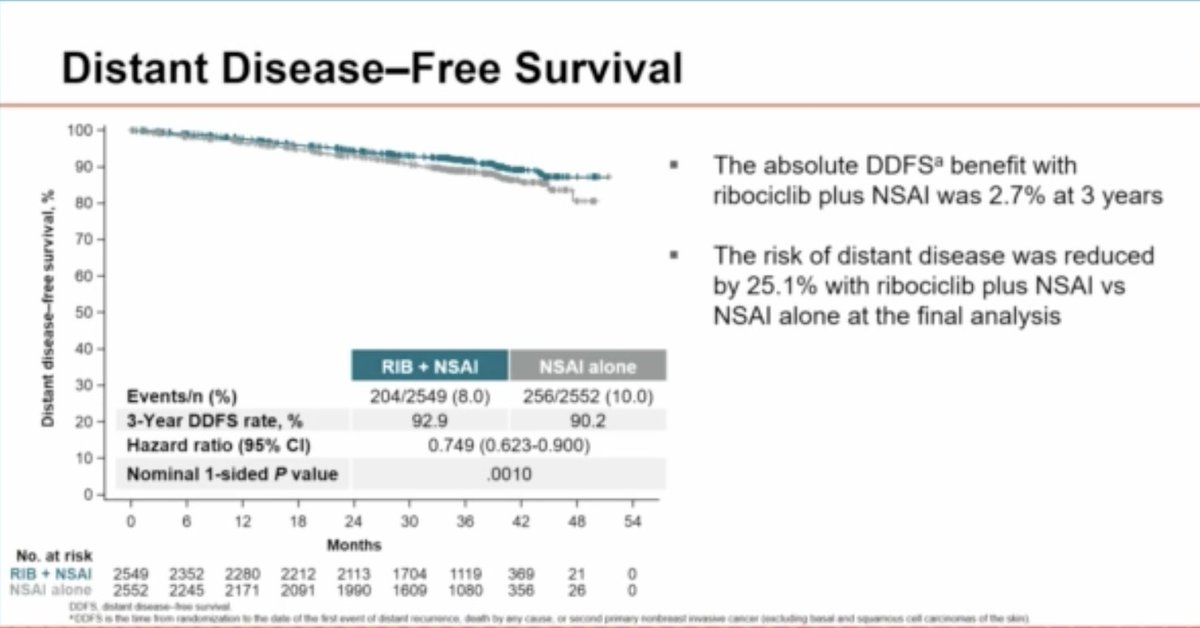
Primary endpoint: invasive disease-free survival (iDFS) per STEEP criteria. Secondary endpoints: recurrence-free survival (RFS), distant disease-free survival (DDFS), overall survival (OS), patient-reported outcomes (PROs), safety/tolerability, and pharmacokinetics. Exploratory endpoints included locoregional recurrence-free survival and time to subsequent antineoplastic therapy.
At the final iDFS analysis (median follow-up 33.3 months), ribociclib plus ET demonstrated a significant iDFS benefit with HR 0.749 (95% CI: 0.628-0.892; p=0.0006). The 3-year iDFS rates were 90.7% versus 87.6%, a 3.1% absolute benefit. At the 4-year landmark analysis (44.2 months median follow-up), the benefit was sustained with HR 0.715 (95% CI: 0.609-0.840; p<0.0001). At the 5-year analysis (58.4 months median follow-up), HR was 0.716 (95% CI: 0.618-0.829; nominal p<0.0001), with 5-year iDFS rates of 85.5% versus 81.0%, representing a 4.5% absolute improvement and a 28.4% reduction in risk of recurrence sustained approximately 2 years after completing ribociclib treatment.
Overall survival data remain immature. At the final iDFS analysis, there were 84 deaths (3%) on the ribociclib arm and 88 deaths (3%) on the ET-alone arm, with an OS HR of 0.89 (95% CI: 0.66-1.20). At the 5-year analysis, the OS trend favored ribociclib with HR 0.800 (95% CI: 0.637-1.003; nominal 1-sided p=0.026), but the trial was not powered for OS.
The 400 mg dose showed a predictable and manageable safety profile. Grade 3+ neutropenia occurred in 44.3% but rarely led to clinical complications (febrile neutropenia 0.3%, no neutropenia deaths). Hepatotoxicity occurred in 26.4% (grade 3+: 8.6%), with DILI in 0.4% including 8 Hy's Law cases, all resolving after discontinuation. QTc prolongation was infrequent at 5.3% all-grade (grade 3+: 1.0%), with no Torsades de Pointes. Treatment discontinuation due to AEs was 19.5%, primarily from elevated transaminases (ALT 7.1%) occurring early (median ~4 months). Dose interruptions occurred in 86.1% and dose reductions in 26.7%, primarily for neutropenia. Median relative dose intensity was 94.0%.
NATALEE established adjuvant ribociclib as the standard of care for the broadest population of HR+/HER2- early breast cancer patients at risk of recurrence, including those with node-negative disease. The 5-year data showing sustained benefit approximately 2 years after completing 3 years of treatment supports a durable biological effect. Key clinical debates include the optimal selection between ribociclib (NATALEE) and abemaciclib (monarchE) given their different patient populations and dosing strategies, the 3-year treatment duration versus the 2-year duration used with abemaciclib, and whether the lower 400 mg dose adequately balances efficacy and tolerability for long-term adjuvant use.
NATALEE is a Phase 3 trial of 3 years of adjuvant ribociclib (Kisqali) plus a nonsteroidal aromatase inhibitor versus endocrine therapy alone in adults with HR-positive/HER2-negative early breast cancer, including a broad population with node-negative disease (NCT03701334).
Yes. On September 17, 2024 the FDA approved Kisqali (ribociclib) in combination with an aromatase inhibitor for the adjuvant treatment of adults with HR-positive, HER2-negative stage II and III early breast cancer at high risk of recurrence. A ribociclib + letrozole co-pack was also approved.
Ribociclib plus endocrine therapy significantly improved invasive disease-free survival versus endocrine therapy alone (HR approximately 0.749; 95% CI 0.628-0.892; p=0.0006), with 3-year iDFS rates of about 90.7% versus 87.6%. The benefit was sustained at 4- and 5-year landmark analyses. Overall survival data remain immature.
NATALEE enrolled a broader population — including some node-negative, higher-risk patients — and used a lower 400 mg ribociclib dose for 3 years, whereas monarchE (abemaciclib) was limited to node-positive high-risk disease. This makes adjuvant ribociclib an option for a wider range of HR+/HER2- early breast cancer patients.
Ribociclib (Kisqali) is a CDK4/6 inhibitor developed by Novartis.
Want the aggregated read across all of this drug's trials? See Physician sentiment on KISQALI® (ribociclib) — KOL Pulse's breakdown of oncologist opinion on ribociclib, the CDK4/6 inhibitor studied in NATALEE.