Early high-risk TNBC perioperative - Merck
Discover KOL Sentiment on KEYNOTE-522 →Presented by Javier Cortés, MD (Sunday, May 31 2026 · Chicago) — the longest follow-up of an immune checkpoint inhibitor in curative-intent breast cancer.
KOL takeaway (Paolo Tarantino, MD): "Adding perioperative pembro to neoadjuvant chemo prevents ~10% recurrences and ~7% deaths from TNBC. A tough neoadjuvant regimen, but one that delivers on its promise."
Live ASCO 2026 coverage → · Source: ASCO 2026 Abstract 507 (median follow-up ~94 mo)
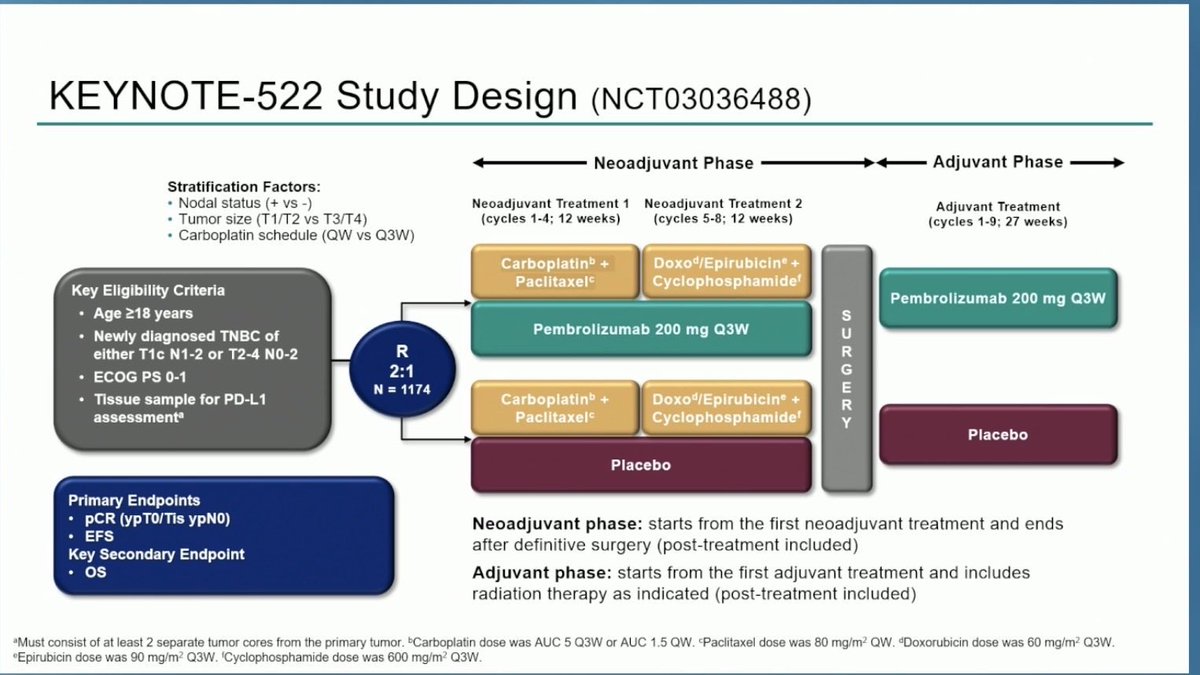
Design - Phase 3 perioperative (neoadjuvant + adjuvant) pembrolizumab + chemotherapy vs chemo + placebo in high-risk stage II-III TNBC (NCT03036488).
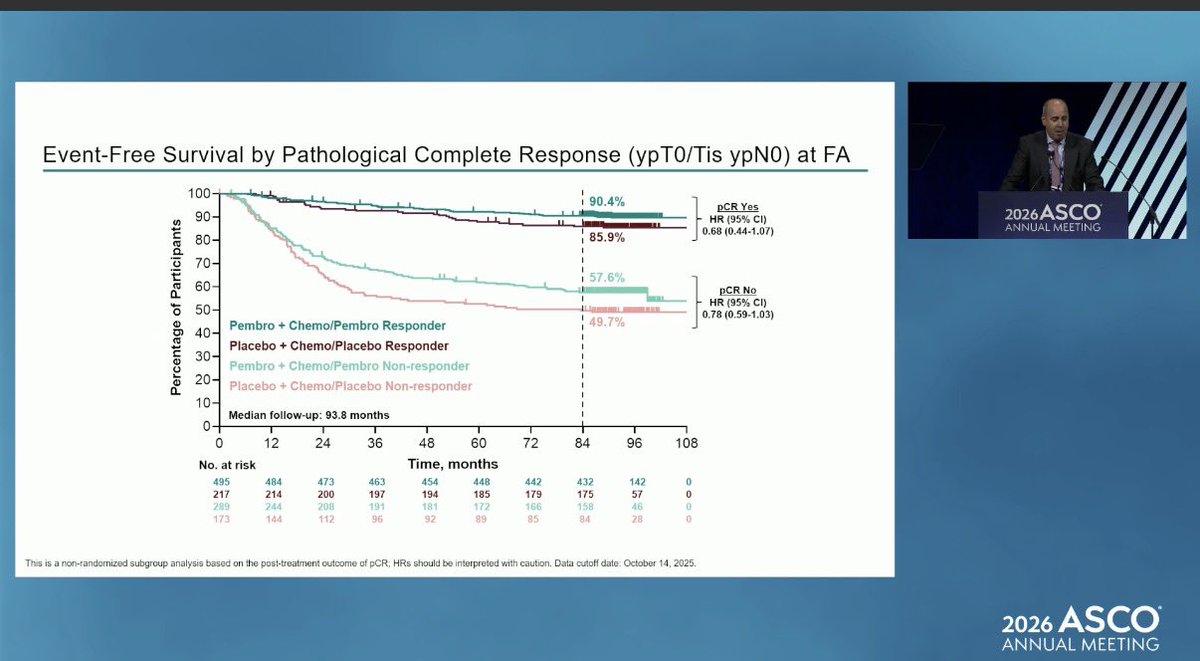
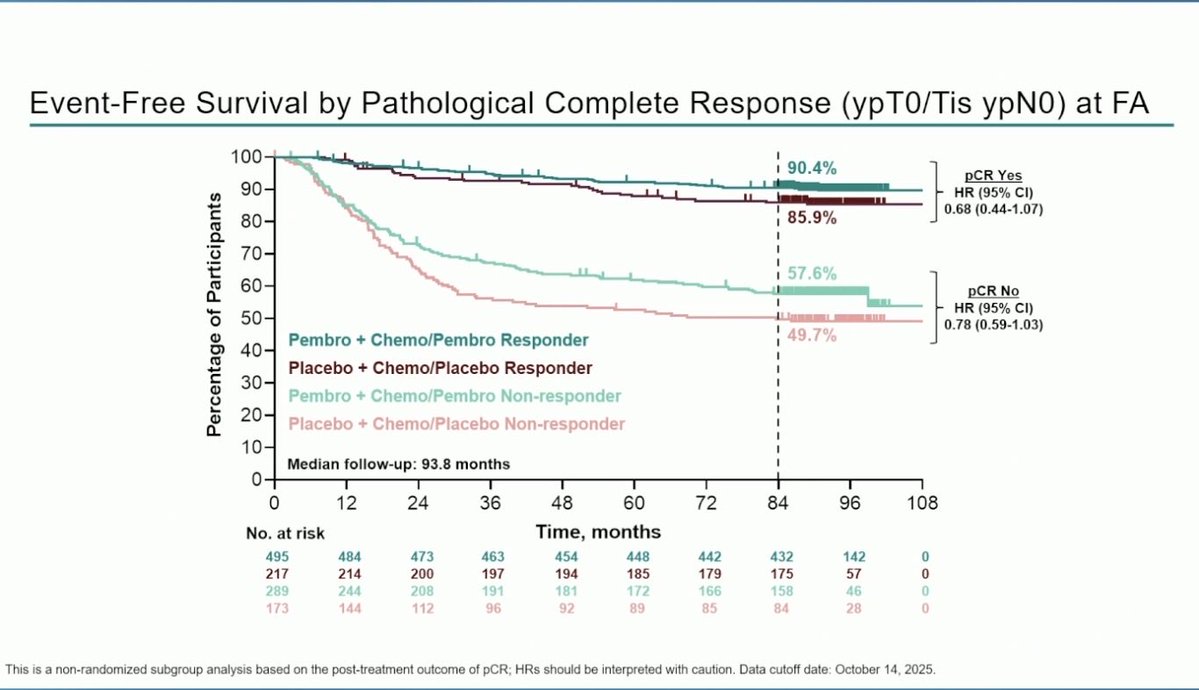
pCR - 63.0% with pembrolizumab vs 55.6% with placebo.
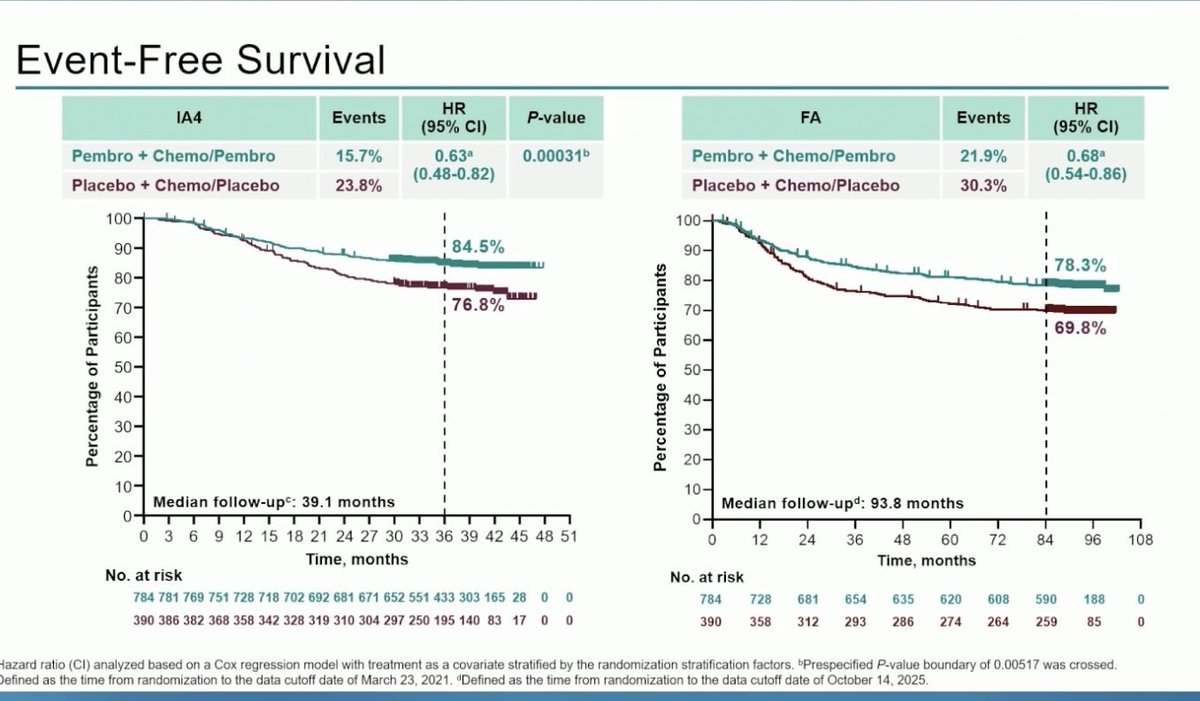
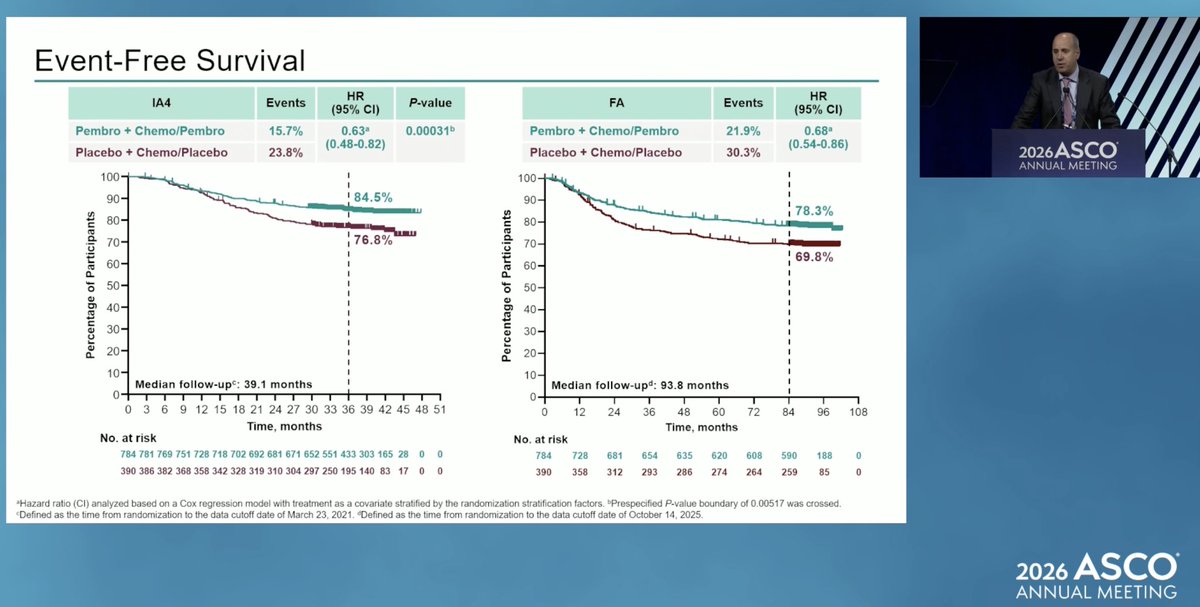
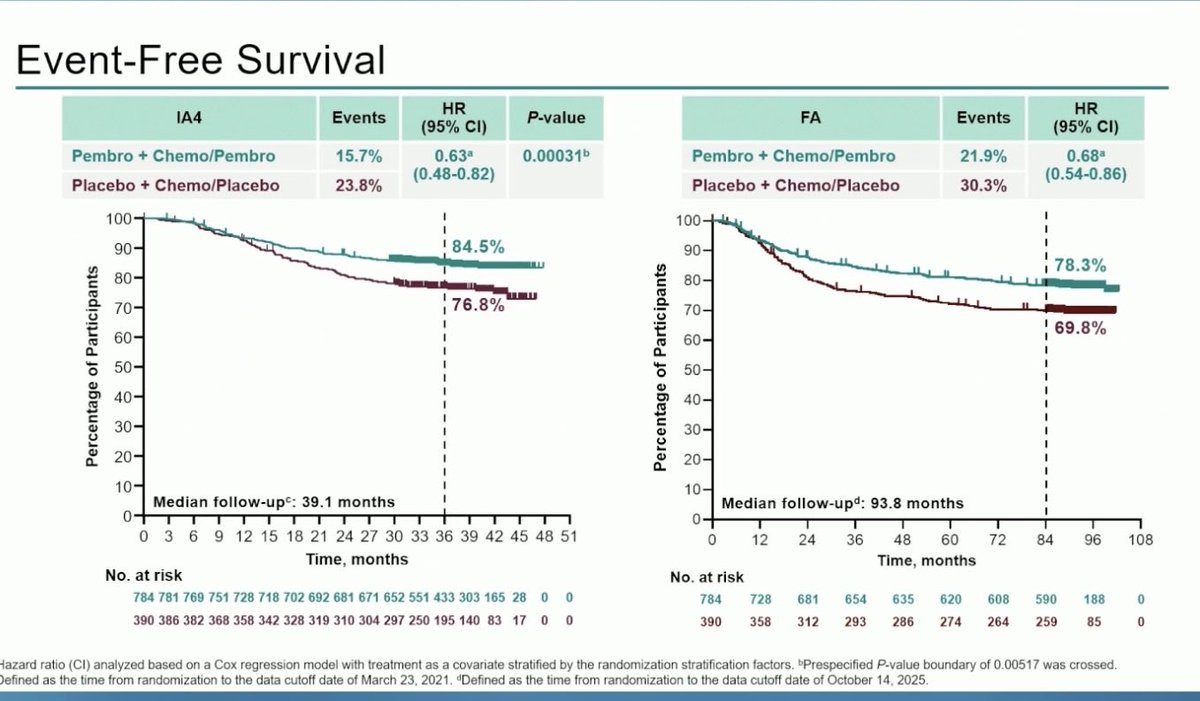
EFS - HR 0.63 (5-yr EFS 81.3% vs 72.3%); ASCO 2026 ~7.8-yr update: 7-yr EFS 78.3% vs 69.8% (HR 0.68).
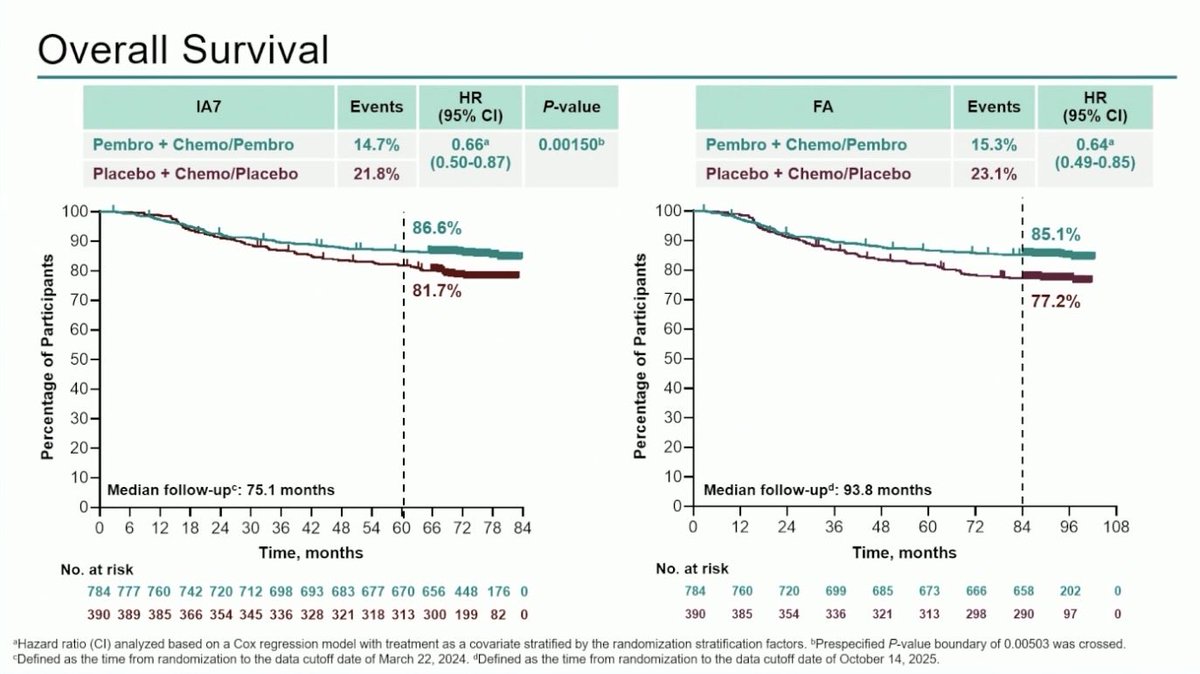
OS - Statistically significant - HR 0.66 (p=0.0015); 5-yr OS 86.6% vs 81.7%; ASCO 2026: 7-yr OS 85.1% vs 77.2% (HR 0.64).
Regulatory - FDA approved July 2021 - perioperative pembrolizumab for high-risk early-stage TNBC.
Sponsor / drug - Merck; pembrolizumab (Keytruda).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.






Top 10 by impressions - click to view on X
This is amazing and will likely become the new SoC… but… how I wish there was that third arm to tell us how much benefit there is from postOP IO (same struggle in TNBC (KN522👇), NSCLC (AEGEAN 👇),...
News Direct from Industry: "KEYNOTE 522 meets OS Endpoint in High Risk Early Stage TNBC #BreastCancer " "New OS results build on the pathological complete response...
⭐️ Mind blowing results of immunotherapy across different tumor types presented #ESMO24 now at @NEJM - Melanoma (CM 067) 10 years FU Nivo, Nivo-Ipi. - TNBC (KEYNOTE-522):...
OS results of KN-522 out in @NEJM. Terrific news: adding pembro to neoadjuvant chemo for TNBC saves lives (5% 5-year Δ). Bad news: we’re stuck with giving 5 drugs to all patients with stage...

Fantastic. But I still believe there is a fraction of people who do not benefit immunotherapy. We need a biomarker driven approach. #ASCO24 #Oncoalert
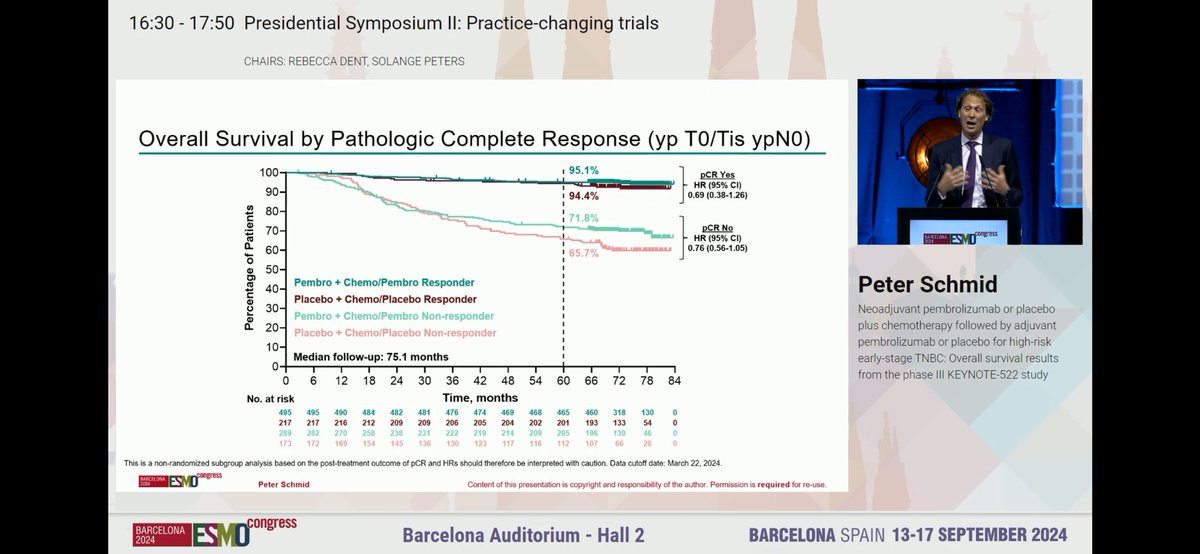
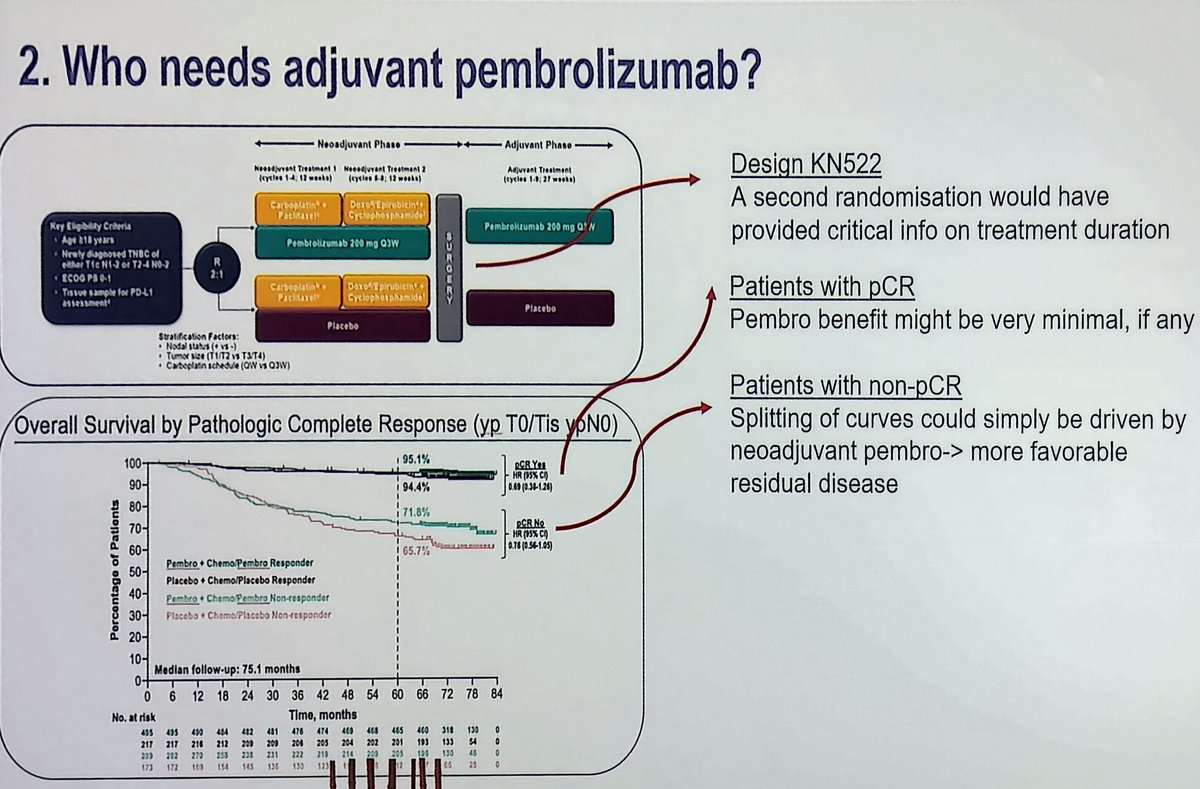
Among patients with triple-negative breast cancer, 5-year survival was 86.6% with neoadjuvant pembrolizumab with chemotherapy followed by adjuvant pembrolizumab and 81.7% with neoadjuvant...
In the KEYNOTE-522 trial, neoadjuvant and adjuvant pembrolizumab improved pathological complete response and event-free survival among patients with early-stage triple-negative breast cancer. Learn...
very important news! Overall Survival seen in KN522!!!

After turkey and all the trimmings, have a gander at this editorial on IO in TNBC. Immunotherapy for Early-Stage Triple-Negative Breast Cancer | New England Journal of Medicine
>70% of the pts in the chemo-alone arm of KN522 are free from recurrence of TNBC at 5 years Identifying these pts is a critical challenge, to avoid exposure to potentially permanent/...
KEYNOTE-522 is a landmark Phase III, randomized, double-blind, placebo-controlled trial that established perioperative pembrolizumab (Keytruda) as the standard of care for patients with high-risk early-stage triple-negative breast cancer (TNBC). The trial randomized 1,174 patients 2:1 to receive neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab, or placebo plus chemotherapy followed by placebo. KEYNOTE-522 is the first immunotherapy-based regimen to demonstrate statistically significant improvements in pCR, EFS, and OS in early-stage TNBC, regardless of PD-L1 expression status.
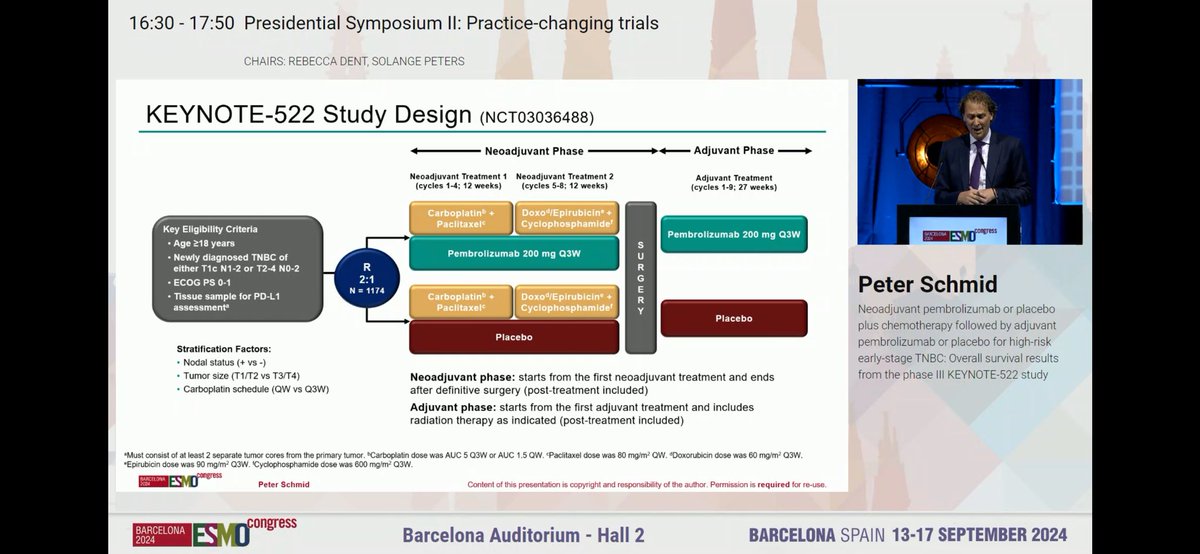
Phase III, international, multicenter, randomized (2:1), double-blind, placebo-controlled trial in patients with newly diagnosed, previously untreated high-risk early-stage TNBC. Randomization was stratified by nodal status (positive vs negative), tumor size (T1/T2 vs T3/T4), and carboplatin schedule (Q3W vs weekly). Patients were enrolled regardless of tumor PD-L1 expression.
Adults aged 18+ with newly diagnosed, previously untreated high-risk early-stage TNBC (tumor >1 cm to ≤2 cm with nodal involvement [T1c N1-N2], or tumor >2 cm regardless of nodal involvement [T2-T4 N0-N2]). ECOG PS 0-1. Enrolled regardless of PD-L1 status. 75% stage II, 25% stage III. Median age 49 years.
Neoadjuvant: pembrolizumab 200 mg Q3W + carboplatin/paclitaxel (4 cycles, 12 weeks) followed by pembrolizumab + doxorubicin or epirubicin + cyclophosphamide (4 cycles, 12 weeks), then surgery, then adjuvant pembrolizumab 200 mg Q3W (9 cycles, 27 weeks). Control arm received placebo in place of pembrolizumab with identical chemotherapy backbone.
Dual primary endpoints: pathological complete response (pCR, defined as ypT0/Tis ypN0) and event-free survival (EFS). Key secondary endpoints: overall survival (OS), safety, and alternative pCR definitions (ypT0 ypN0, ypT0/Tis).
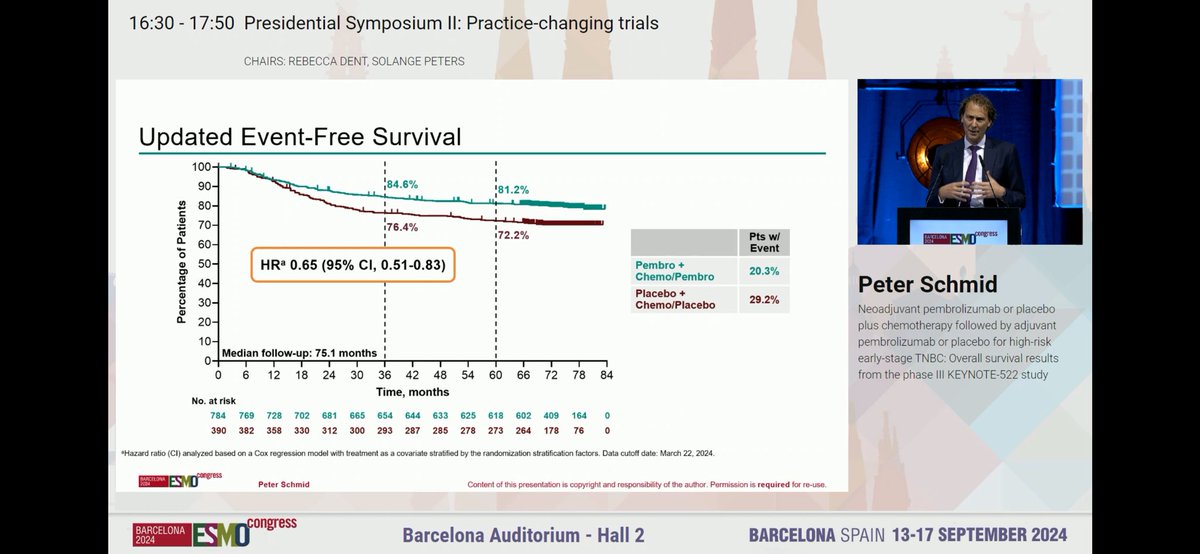
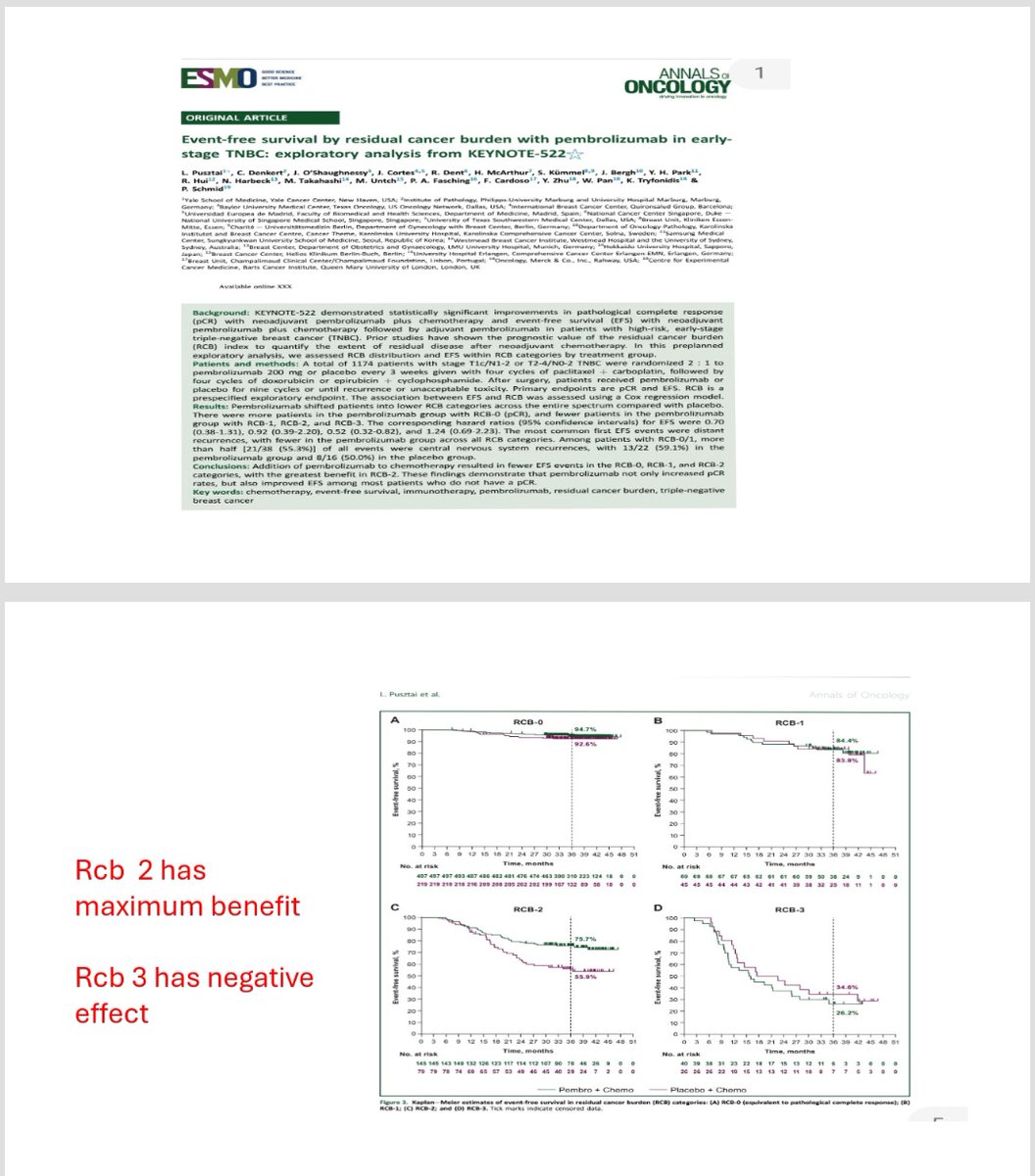
Pembrolizumab significantly improved pCR and EFS. The pCR rate was 63.0% (95% CI: 59.5–66.4) vs 55.6% (95% CI: 50.6–60.6) with placebo. At 39.1-month median follow-up, EFS HR was 0.63 (95% CI: 0.48–0.82; p=0.00031), a 37% risk reduction. The 3-year EFS rate was 84.5% vs 76.8%. At 63.1-month follow-up, 5-year EFS was 81.3% vs 72.3%. Updated analysis at 75.1-month median follow-up confirmed EFS HR of 0.65 (95% CI: 0.51–0.83), with 5-year EFS of 81.2% vs 72.2%.
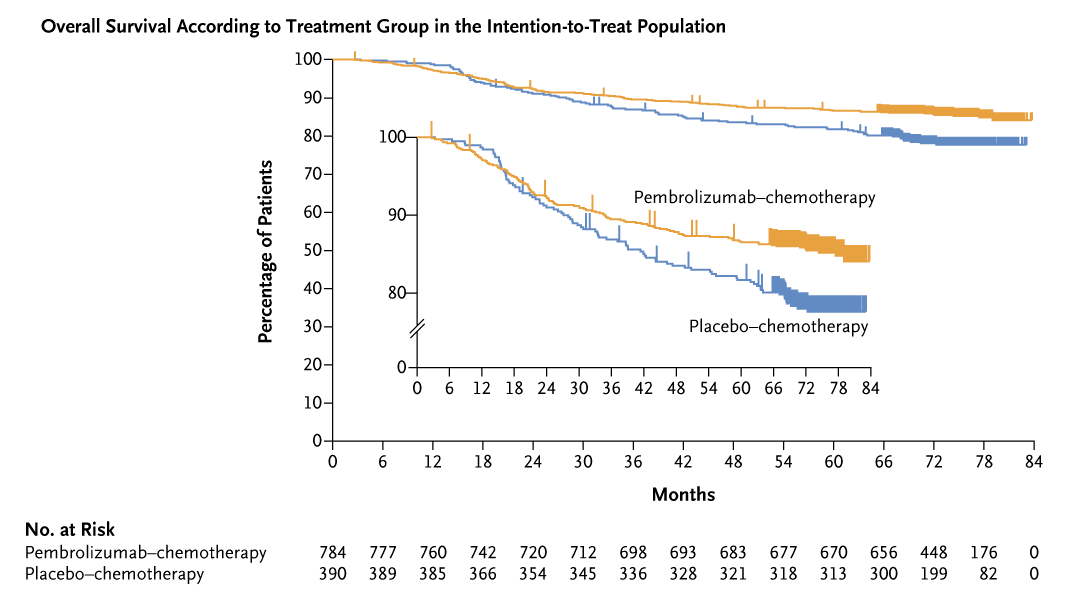
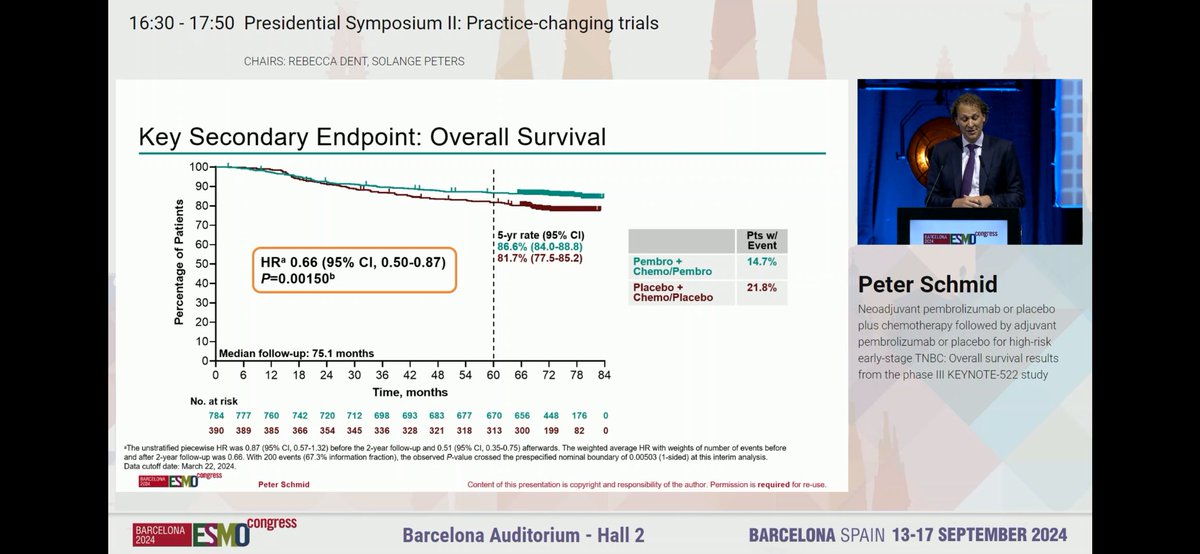
At a median follow-up of 75.1 months, the pembrolizumab regimen demonstrated a statistically significant OS benefit. OS HR was 0.66 (95% CI: 0.50–0.87; p=0.0015), a 34% reduction in risk of death. The 5-year OS rate was 86.6% (95% CI: 84.0–88.8) vs 81.7% (95% CI: 77.5–85.2). Median OS was not reached in either arm. Deaths occurred in 15% (115/784) of pembrolizumab patients vs 22% (85/390) of placebo patients.
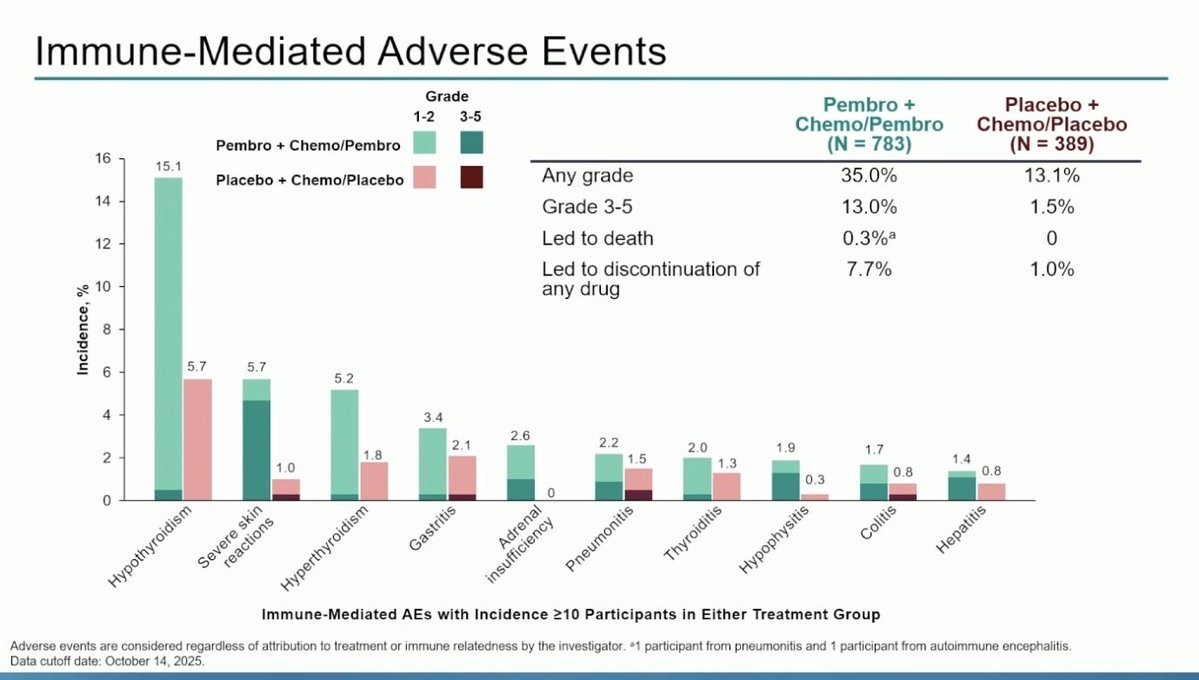
Grade 3-5 treatment-related AEs occurred in 82.4% (pembrolizumab) vs 78.7% (placebo) in combined phases. Serious adverse reactions in 44% of pembrolizumab patients; most common (≥2%): febrile neutropenia (15%), pyrexia (3.7%), anemia (2.6%). Immune-mediated AEs in 44.8% vs 22.9%; most common: infusion reactions (18.0%), hypothyroidism (15.1%). Pembrolizumab permanently discontinued in 20% due to AEs (ALT 2.7%, AST 1.5%, rash 1%). Fatal TRAEs in 0.5% (n=4) vs 0.3% (n=1). Most common AEs (≥20%): fatigue (70%), nausea (67%), alopecia (61%), rash (52%).
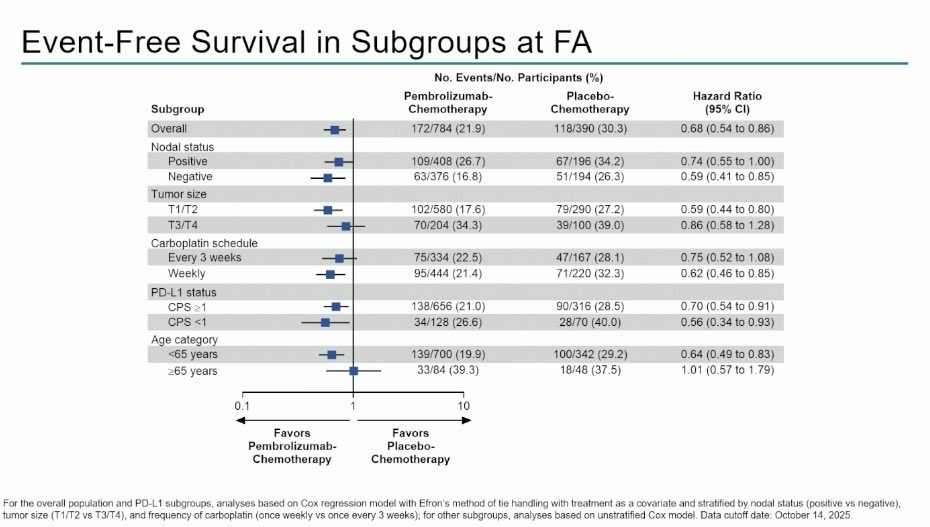
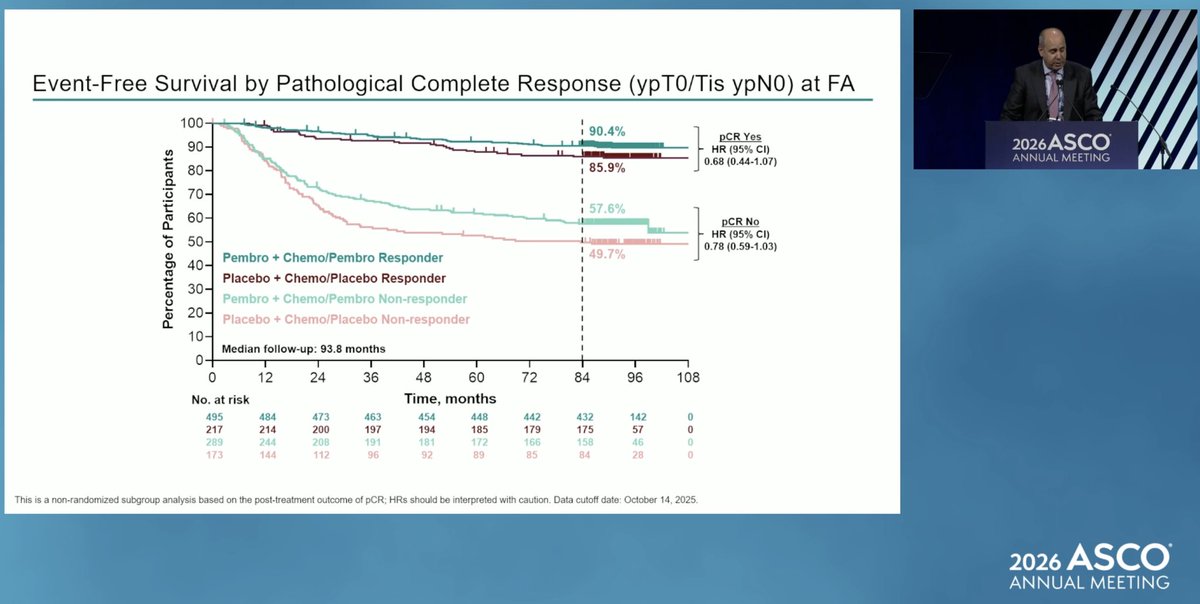
KEYNOTE-522 established perioperative pembrolizumab plus chemotherapy as the standard of care for high-risk early-stage TNBC, with durable pCR, EFS, and OS benefits regardless of PD-L1 status. It is the first and only immunotherapy-based regimen to show a statistically significant OS improvement in this setting. Key clinical debates include optimal management of patients who do not achieve pCR (escalation strategies), the role of PD-L1 status in treatment decisions despite the all-comers benefit, and the contribution of each treatment phase (neoadjuvant vs adjuvant pembrolizumab) to the observed benefit.
KEYNOTE-522 is a Phase 3 randomized trial (NCT03036488) testing perioperative pembrolizumab (Keytruda) - neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab - versus neoadjuvant chemotherapy plus placebo in high-risk early-stage (stage II-III) triple-negative breast cancer. Its co-primary endpoints were pathologic complete response (pCR) and event-free survival (EFS).
The pCR rate was 63.0% with pembrolizumab versus 55.6% with placebo, EFS favored pembrolizumab (HR 0.63; 5-year EFS 81.3% vs 72.3%), and overall survival was significantly improved (HR 0.66, p=0.0015; 5-year OS 86.6% vs 81.7%). The ASCO 2026 update at roughly 7.8-year follow-up reported 7-year EFS of 78.3% vs 69.8% (HR 0.68) and 7-year OS of 85.1% vs 77.2% (HR 0.64). It is the first immunotherapy-based regimen to show a statistically significant OS improvement in early-stage TNBC.
Yes. In July 2021 the FDA approved pembrolizumab (Keytruda) in combination with neoadjuvant chemotherapy and then continued as a single agent in the adjuvant setting for the treatment of high-risk early-stage TNBC. The approval covers the perioperative regimen tested in KEYNOTE-522, regardless of PD-L1 expression.
Grade 3-5 treatment-related adverse events occurred in 82.4% of pembrolizumab patients versus 78.7% with placebo, and immune-mediated adverse events were more frequent with pembrolizumab (44.8% vs 22.9%), most commonly infusion reactions and hypothyroidism. Pembrolizumab was permanently discontinued in about 20% of patients. Immune-related toxicity monitoring is required.
The regimen is intended for patients with high-risk early-stage (stage II-III) triple-negative breast cancer. Benefit was seen regardless of PD-L1 expression, so PD-L1 testing is not required to select patients for this perioperative approach.